Introduction
Travis et al (1) proposed pulmonary large cell
neuroendocrine carcinoma (LCNEC) as a novel category of
neuroendocrine tumor in 1991. Although certain studies have
reported cases of pulmonary LCNEC (1,2), its
clinicopathological features have not been fully characterized due
to its rarity. The present study describes a case of pulmonary
LCNEC exhibiting extensive pagetoid spread in the bronchial
epithelium. Due to the unexpected nature of the pagetoid spread,
difficult surgical decisions were determined during the initial
surgical procedure. Written informed consent was obtained from the
patient.
Case report
In February 2010, a 75-year-old male presented to
Hyogo Cancer Center (Akashi, Japan) with an abnormal chest X-ray
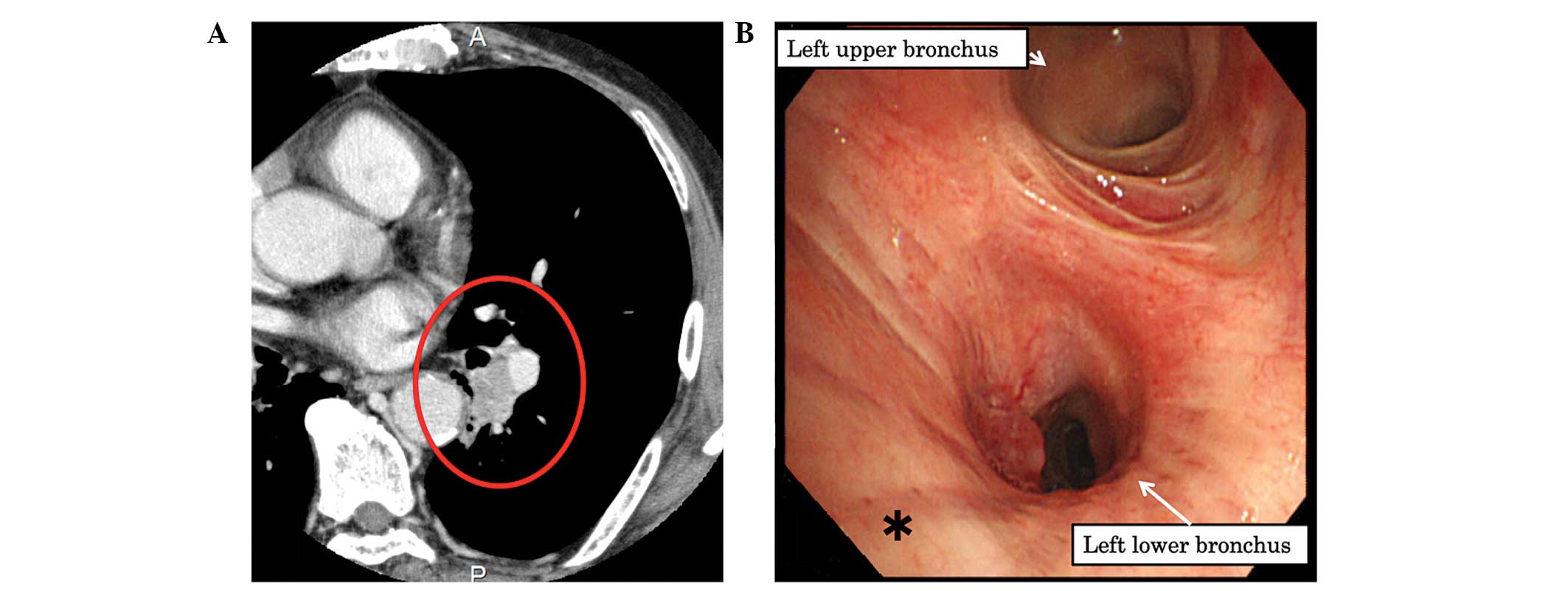
shadow. Chest computed tomography (CT) revealed a 25×21-mm tumor in
the hilum of the left lower lobe without any indication of
lymphadenopathy or metastasis (Fig.
1A). Positron emission tomography-CT demonstrated a marked
accumulation of fluorodeoxyglucose in the tumor, with a maximum
standardized uptake value of 7.82. This indicated that the lesion
was a type of lung cancer, stage
cT1bN0M0. Staging was designated
using the TNM classification according to the 7th edition of the
American Joint Committee on Cancer Staging Manual and the Revised
International System for staging lung cancer (3). Spirometry determined the patient’s
forced vital capacity to be 3.40 liters, which was 103.1% of the
predicted value; the forced expiratory volume in 1 sec was 1.84
liters and 68.8% of the predicted value. A bronchoscopy examination
demonstrated that the tumor was completely obstructing the B6 left
lower lobe. The tumor and the area around the second carina closer
to the carina in the bronchial airway were biopsied to estimate the
nature of the invasive area (Fig.
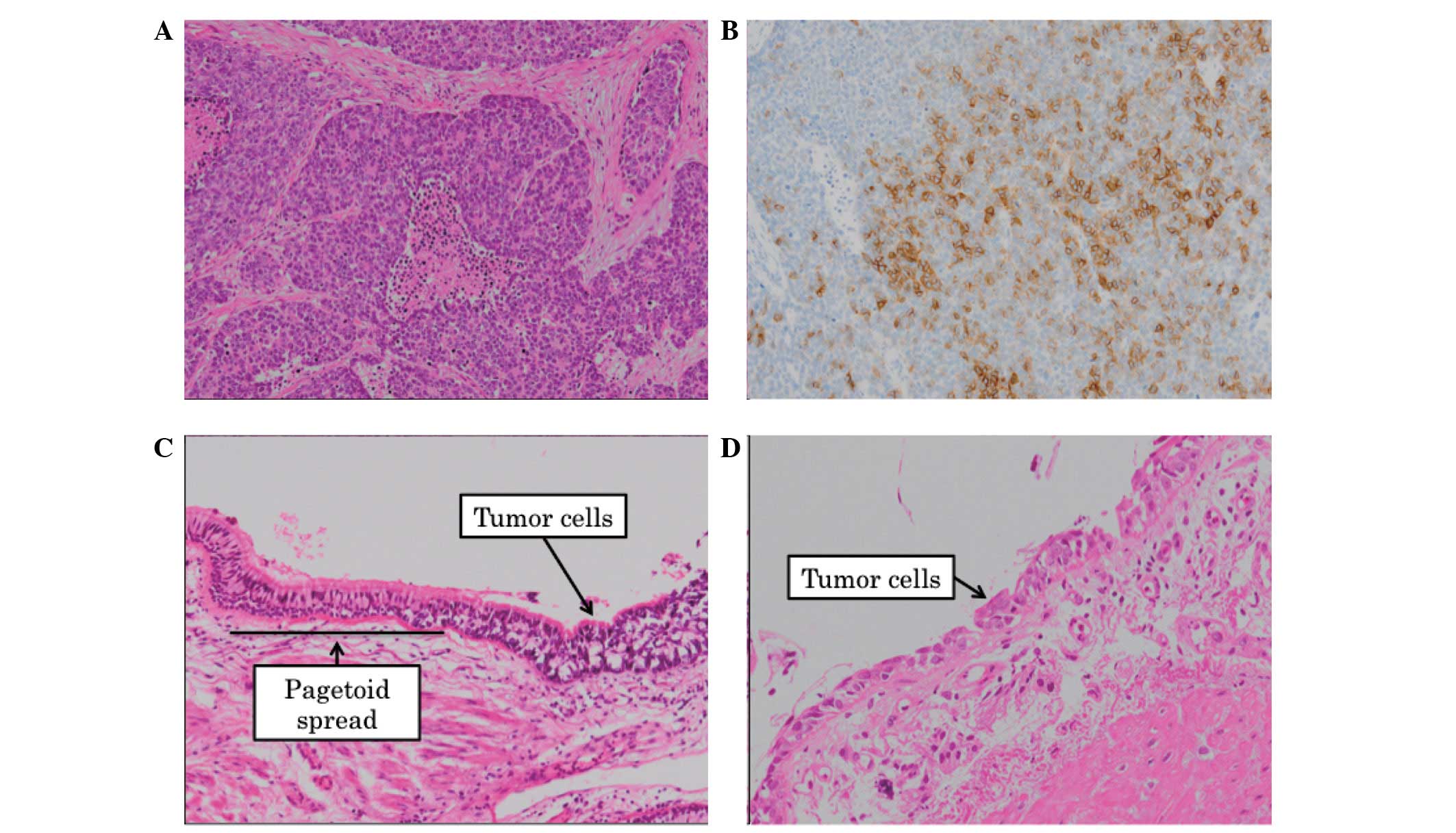
1B). Pathology revealed a suspected LCNEC with the central side
appearing to be intact (Fig. 2A and
B). A left lower sleeve lobectomy with mediastinal lymph node
dissection was planned.
During surgery, there were no signs of macroscopic
bronchial invasion by the tumor. Based on the preoperative
diagnosis, the left lower lobe, including aspects of the left main
bronchus was resected to achieve a sufficient surgical margin.
Although the central bronchial excision line was >25 mm away
from the tumor, examination of frozen sections of the central
segment revealed the presence of tumor cells. Consequently, further
resection of the left main bronchus, 10 mm closer to the carina,
was performed; however, microscopy revealed that tumor cells
remained. A pneumonectomy was considered, however, a complete
resection was not guaranteed due to uncertainty regarding the
extent of the tumor spread. Considering the age and lung function
of the patient, a pneumonectomy was not performed and the surgery
was concluded with a sleeve lobectomy and was determined to be a
microscopically incomplete resection.
Pathology of the postoperative sample revealed that
the tumor was a stage pT1bN0M0
LCNEC, pathologic stage 1A (3) and
that there was extensive one layer invasion to the central side in
the bronchial epithelium, termed pagetoid spread (Fig. 2C). Careful review of the biopsied
specimen during a preoperative bronchoscopy revealed that the tumor
invasion was already present as pagetoid spread surrounding the
second carina (Fig. 2D).
Following surgery, a bronchoscopy was performed and
the bronchial tissues between the trachea and the anastomotic site
were biopsied; however, no tumor cells were identified. It was
presumed that the tumor cells were present only at the very
near-side of the anastomotic site. Subsequently, adjuvant
radiotherapy (25 fractions of 50 Gy) was administered according to
the National Comprehensive Cancer Network guidelines (4). The patient remained healthy without
any signs of recurrence for 30 months following the surgery, as
determined by systemic work-up including enhanced chest CT, brain
magnetic resonance imaging and bone scintigraphy.
Discussion
The term pagetoid spread refers to a rare pattern of
infiltration of cancer cells when a massive carcinoma is identified
beneath the intraepithelial spread. Paget’s disease of the breast
is well known to exhibit this pattern of infiltration, however, it
is also observed in extramammary areas, such as the genital region
(5). With regard to the lungs,
diffuse idiopathic pulmonary neuroendocrine cell hyperplasia
(DIPNECH) demonstrates a similar type of progression (6). Although DIPNECH is considered to be a
precursor lesion of carcinoid tumors (6), the present case was pathologically
diagnosed as a pulmonary LCNEC. Furthermore, 25 mm of
macroscopically tumor-free bronchial margin is considered to be
safe to perform a lung cancer resection (7). Despite the bronchial margin from the
tumor edge being >35 mm, tumor cells remained in the present
case. This case was exceptional due to the rare spreading pattern
and the extent of the tumor invasion.
Preoperative diagnosis was complex for this rare
spreading pattern due to the single layer of tumor cells in the
bronchial epithelium. An accurate assessment of the tumor invasive
area may contribute to a more effective therapeutic strategy.
Although it is difficult to determine a final diagnosis of LCNEC
using only biopsy specimens (8), a
diagnosis of ‘possible LCNEC’ has been proposed by the
International Association for the Study of Lung Cancer Study Group,
the American Thoracic Society and the European Respiratory Society
Classification for Small Biopsies (9). When biopsy specimens meet the criteria
of ‘possible LCNEC’, clinicians and surgeons should pay particular
attention to the bronchial margin from the tumor, as LCNEC may
manifest as extensive pagetoid spread.
References
|
1
|
Travis WD, Linnoila RI, Tsokos MG, et al:
Neuroendocrine tumors of the lung with proposed criteria for
large-cell neuroendocrine carcinoma. An ultrastructural,
immunohistochemical, and flow cytometric study of 35 cases. Am J
Surg Pathol. 15:529–553. 1991.
|
|
2
|
Doddoli C, Barlesi F, Chetaille B, et al:
Large cell neuroendocrine carcinoma of the lung: an aggressive
disease potentially treatable with surgery. Ann Thorac Surg.
77:1168–1172. 2004.
|
|
3
|
Edge SB, Byrd DR, Compton CC, Fritz AG,
Greene FL and Trotti A: AJCC Cancer Staging Handbook. 7th edition.
Springer; New York: 2009
|
|
4
|
NCCN clinical practice guidelines in
oncology: Non-small cell lung cancer. National comprehensive cancer
network. http://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf.
Accessed January 17, 2013
|
|
5
|
Mahdi H, Thrall M, Agoff N and Doherty M:
Pagetoid adenocarcinoma in situ of the cervix with pagetoid spread
into the vagina. Obstet Gynecol. 118:461–463. 2011.
|
|
6
|
Davies SJ, Gosney JR, Hansell DM, et al:
Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia: an
under-recognised spectrum of disease. Thorax. 62:248–252. 2007.
|
|
7
|
Kara M, Dizbay Sak S, Orhan D and Kavukçu
S: Proximal bronchial extension with special reference to tumor
localization in non-small cell lung cancer. Eur J Cardiothorac
Surg. 20:350–355. 2001.
|
|
8
|
den Bakker MA, Willemsen S, Grünberg K, et
al: Small cell carcinoma of the lung and large cell neuroendocrine
carcinoma interobserver variability. Histopathology. 56:356–363.
2010.
|
|
9
|
Travis WD, Brambilla E, Noguchi M, et al:
International association for the study of lung cancer/american
thoracic society/european respiratory society international
multidisciplinary classification of lung adenocarcinoma. J Thorac
Oncol. 6:244–285. 2011.
|