Introduction
As the second most common type of cancer in females
worldwide, cervical cancer is characterized by a range of minor to
severe neoplastic changes in the epithelium. More than 80% of the
estimated 530,000 novel cases and 275,000 mortalities due to
cervical cancer each year occur in the developing countries
(1). The most common symptoms of
cervical cancer are unusual vaginal bleeding and persistent vaginal
discharge that is blood-stained or smells unpleasant. Unusual
vaginal bleeding is more likely to be present at earlier stages of
the disease (2). Cervical cancer
diagnoses made at an earlier stage according to International
Federation of Gynecology and Obstetrics (FIGO) (stages 1a1 to 1b2)
are associated with higher survival rates (80–99%) compared with
diagnoses made at a later stage (stages III–IV) which have
associated five-year survival rates of 20–50%) (2).
An abdominal radical hysterectomy (RAH) with pelvic
lymphadenectomy is the standard treatment for cervical cancer
patients at stages Ia2-IIa. For patients who develop locally
advanced cervical cancer, the standard of care has evolved from
external beam radiation therapy (EBRT) alone, to EBRT plus
brachytherapy, to combined EBRT plus brachytherapy with concurrent
chemotherapy (3)
Cervical carcinoma metastasizes predominantly via
direct extension and the lymph nodes, while the hematogenous route
is relatively rare. Lung and supraclavicular lymph nodes are common
sites for distant invasion. Lung and supraclavicular lymph nodes
are common sites for distant invasion. Bone metastasis is rare,
predominantly involving the vertebrae, followed by the pelvic bone,
while uncommon in the distal appendicular bone (4,5). Bone
metastasis is indicative of a poor prognosis and patient quality of
life is severely affected. The present study reports a case of
isolated tibial metastases secondary to cervical carcinoma, with a
review of the relevant literature. Written informed consent was
obtained from the patient.
Case report
Clinical presentation
On February 20th 2010, a 43-year-old female was
admitted to the Affiliated Hospital of Qingdao University (Qingdao,
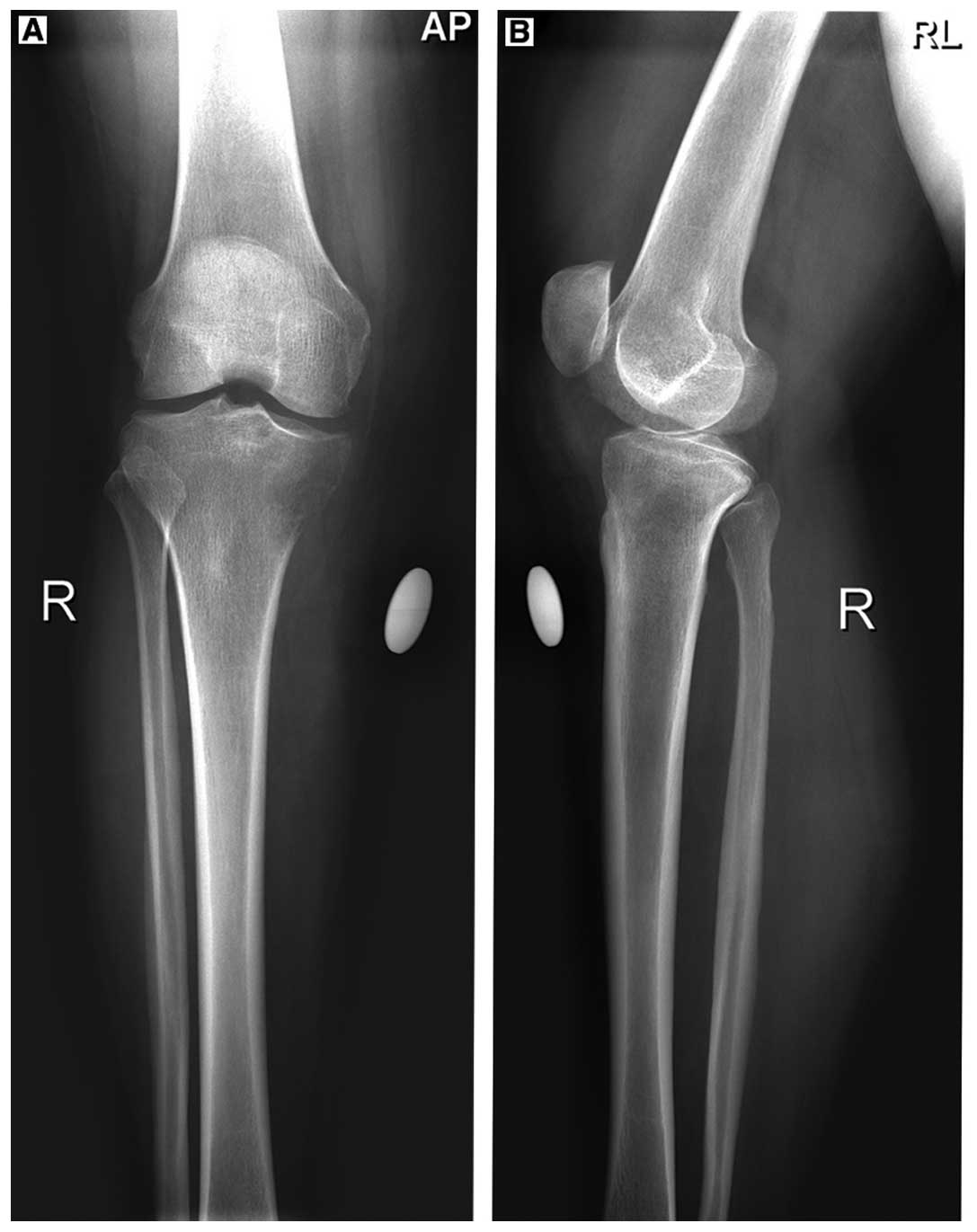
China), with progressive right knee pain of three months. Physical
examination revealed a marginally swollen right knee with medial
tenderness and limited flexion activity. X-ray indicated the
presence of a space-occupying lesion in the right knee medial tibia
platform (Fig. 1). Subsequently,
the patient was diagnosed with a right tibial tumor.
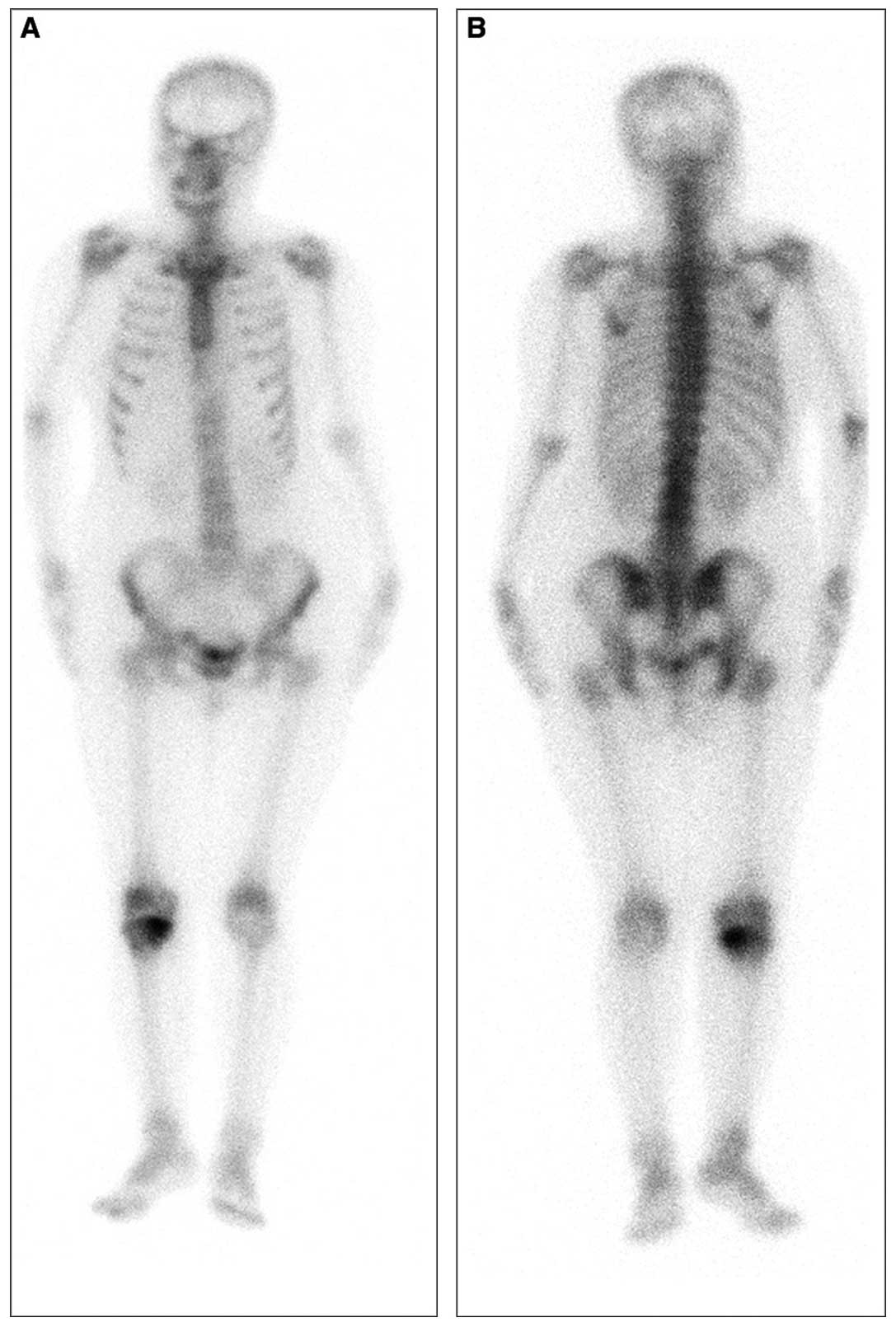
Emission computed tomography (ECT) demonstrated an
abnormal concentration of radioactive material in the inner side of
the upper tibia. The bones of the rest of the body were normal
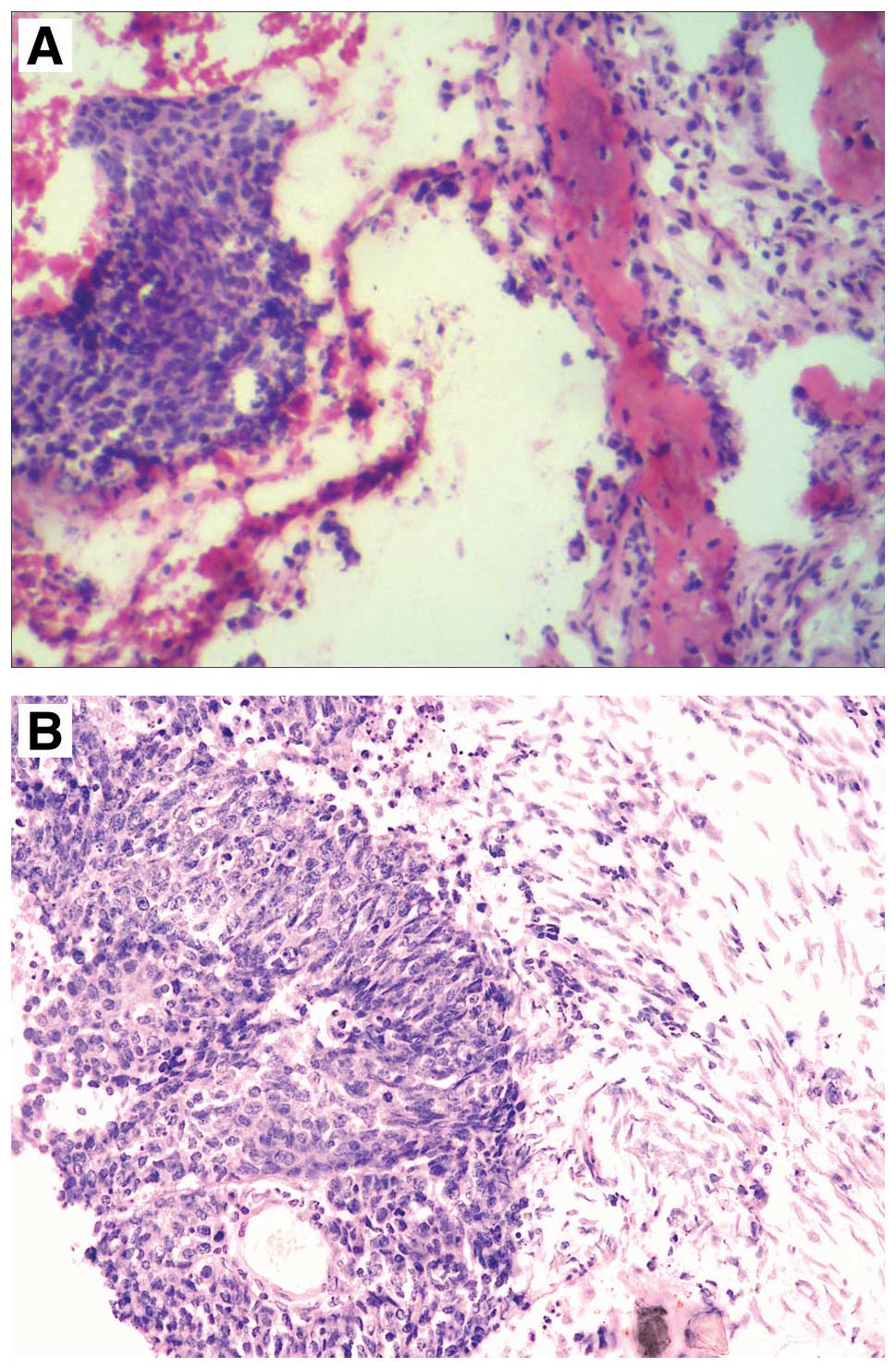
(Fig. 2). Biopsy of proximal tibiae
revealed the presence of poorly differentiated metastatic squamous
cell carcinoma (Fig. 3). The
patient underwent right tibia tumor resection and an allogeneic
bone graft.
Further examination by a gynecologist revealed that
the patient exhibited prolonged menstruation accompanied by
subclinical vaginal discharge for three months. Gynecological
examination identified a mildly erosive cervix, with a marginally
hypertrophic anterior lip and the uterine body was at a size
comparable to that observed in females who are ~40 days pregnant;
however, no adnexal masses were identified. Color Doppler
ultrasound revealed a highly vascularized hypo echoic lesion
extending from the lower segment of the uterine body to the cervix
(5.3×3.3×4.0 cm) with an irregular shape and unclear boundary from
the endometrium. Computed tomography (CT) revealed an enlarged
uterine body lesion, occupying the left inguinal area and multiple
hyper-density masses in the mediastinum. Liquid-based cervical
cytology indicated negativity for intraepithelial lesions or
malignancy. The levels of tumor markers were all within normal
ranges; serum cancer antigen 125 (CA125), CA199 and
carcinoembryonic antigen levels were 19.15 kU/l, 2.57 kU/l and 0.73
μg/l, respectively. The pathology of fractional curettage and
cervical biopsy revealed poorly differentiated squamous cell
carcinoma in the cervical canal and lower segment of the uterine
cavity. The patient was diagnosed with FIGO stage Ib2 cervical
squamous cell carcinoma with tibial metastasis (6).
Treatment and outcome
The patient underwent extensive hysterectomy,
bilateral adnexectomy, and pelvic and para-aortic lymph node
dissection. Intra-operative examination revealed that the size of
the uterus was comparable to that of a female who is ~40 days
pregnant, and the lower segment was enlarged. The right common and
external iliac lymph nodes, as well as the para-aortic lymph nodes,
were enlarged and hard. Interventional chemotherapy with 60 mg
cisplatin and 500 mg fluorouracil was administered via the
bilateral internal iliac arteries. Postoperative histopathological
examination revealed poorly differentiated cervical squamous cell
carcinoma with para-aortic lymph node metastasis (Fig. 3) and endometrial complex
hyperplasia, with regional moderately atypical hyperplasia. The
patient underwent six courses of chemotherapy with cisplatin and
paclitaxel, as well as pelvic radiotherapy. Following chemotherapy,
the patient was evaluated by pelvic and thoracic CT, as well as
tibia and fibula X-rays. The results of the additional examinations
were normal. During the follow-up period of 41 months, no
metastasis or recurrence was identified.
Discussion
Cervical carcinoma is one of the most common types
of malignant tumor in females. The incidence of bone metastasis is
clinically confirmed as ~1.1–8.2% (7–10).
However, based on autopsy data, bone metastasis incidence is as
high as 8.6–17.9%, which is significantly higher than that
identified clinically (11,12). In a study by Yoon et al
(13), 105 patients with bone
metastasis with invasive carcinoma of the uterine cervix were
retrospectively analyzed. The authors demonstrated that
adenocarcinoma, advanced stage (IIB–IV) and initial multiple bone
metastases contribute to earlier bone metastasis. Cervical squamous
cell carcinomas metastasize predominantly via direct extension and
the lymph nodes, while the hematogenous route is relatively rare.
Bone metastasis is rare, predominantly involving the vertebrae,
followed by the pelvic bone, while uncommon in the distal
appendicular bone (4,5). A number of studies have reported cases
of isolated localized metastasis to the fibula, patella and
humerus, arising from cancer of the uterine cervix (14–16).
To the best of our knowledge, the present case of isolated tibial
metastasis arising from cervical squamous cell carcinoma is even
rarer. In the present case, the patient exhibited no evidence of a
clinical gynecological disorder until the tibial tumor was
diagnosed.
In clinical practice, bone metastases arising from
malignant tumors usually present as severe and progressive pain in
metastatic sites, and pathological fracture may occur (10). X-ray, total bone ECT examination,
needle biopsy of the local lesion and positron emission tomography
(PET)-CT scans are useful methods used to detect lesions of
advanced cervical carcinoma (17).
The diagnostic criteria of bone metastasis are as follows (18): (i) Local intermittent or persistent
bone pain; (ii) total body bone ECT examination showing abnormal
radioactive material accumulation at the site of the lesion, the
concentration of which is higher than that of the contralateral or
adjacent areas; (iii) X-ray, CT or magnetic resonance imaging
examination demonstrating the presence of osteolytic or
osteoblastic changes, bone uplift and pathological fractures; and
(iv) follow-up confirming persistent existence or further
extensions of the lesion. Diagnosis is established if the criteria
of (i), (ii) and (iv) or (i), (iii) and (iv) are met. Biopsy is the
‘gold standard’ for the detection of bone metastasis arising from
cervical carcinoma (19). Clinical
manifestations, combined with corresponding imaging examination
such as X-ray, CT or MRI and histopathology contribute to the early
diagnosis of bone metastasis arising from cervical carcinoma. The
predominant symptom exhibited in the present case was progressively
aggravated pain in the right knee. ECT examination revealed
radioactive material accumulation in the proximal end of the right
tibia, and biopsy confirmed the pathology of poorly differentiated
squamous cells. Finally, the detection of a lesion exhibiting the
same phenotype in the cervix further confirmed the diagnosis.
Malignant tumors with bone metastases require
standardized guidelines regarding the therapeutic options. Current
treatments focus on pain relief, prolonging patient life and
preservation of patient quality of life (15). Previous studies have shown that
short-cycle radiotherapy can be as effective as long-cycle
radiotherapy in alleviating pain caused by bone metastases
(20). Generally, surgical
management or fixation of pathological fracture is recommended in
cases of good ECOG performance status (21) with solitary bone metastasis,
supplemented by palliative radiotherapy (22). Pasricha et al (14) indicated that surgery combined with
concurrent chemoradiotherapy may achieve better effects for
patients with metastases who are in good physical condition.
Diphosphonates used in palliative treatment have been demonstrated
to be effective in relieving pain, reducing the occurrence of
pathological fractures and improving quality of life; however, they
did not prolong survival time (23). Another study found that
PET-CT-guided treatments improved the overall survival rates of
patients with locally advanced cervical cancer (24). The patient in the present case
underwent aggressive treatment of the primary tumor, supplemented
with chemotherapy. A positive response to treatment was observed
and the patient was free of disease at the 41-month follow-up
visit.
Pasricha et al (14) presented a case of FIGO stage IIB
cervical carcinoma. The patient developed fibula metastasis nine
months following radiotherapy and underwent surgical excision of
metastatic lesion; however, the patient refused further salvage
chemotherapy. The patient succumbed to the disease 48 months
following the presentation of primary symptoms. Furthermore,
Corrado et al (15)
presented a patient with poorly differentiated cervical
adenosquamous carcinoma in stage IIB who underwent surgical
resection of a femoral metastatic lesion. After three months the
patient succumbed to the disease as concurrent chemoradiotherapy
was refused. It has been reported that bone metastasis usually
occurs within two years of the diagnosis of the primary tumor.
Patients generally succumb to the disease within 18 months of the
diagnosis of bone metastasis, which indicates a poor prognosis
(22). Abdul-Karim et al
(11) analyzed 20 cases of cervical
carcinoma with bone metastases and found that 71% of bone
metastases occurred within two years of diagnosis. Zhao et
al (24) performed a clinical
analysis of eight patients with bone metastases from uterine
malignant tumor, and found that occurrence times were similar to
those reported in a study by Abdul-Karim et al (11). Previous studies have shown that the
prognosis of patients with bone metastasis was associated with
metastatic site (isolated or multiple bone metastases), and whether
lymph nodes or other organs were involved (24). Other factors, including whether
treatments of primary malignant tumor were standardized or
therapeutic options for bone metastases such as surgery, EBRT, EBRT
plus brachytherapy, or combination EBRT plus brachytherapy with
concurrent chemotherapy, have been found to contribute to the
prognosis (24).
The primary symptom presented by the patient in the
current case was local pain in the metastatic bone without evident
manifestation of the primary tumor. Therefore, a detailed
investigation of medical history and comprehensive physical
examination are required when clinicians diagnose patients with
local bone pain, in order to avoid any delay in treatment. The
patient underwent surgery (RAH with a pelvic lymphadenectomy) for
the primary tumor when a definitive diagnosis had been made, which
was then followed by chemoradiotherapy. The patient responded well
to the treatments, and was free of recurrence and metastasis at the
41-month follow-up visit. Therefore, this case indicated that
aggressive and acurate treatments are beneficial for advanced
cancer patients with bone metastases. A combination of standardized
surgical treatment and chemoradiotherapy must be recommended to
achieve the best outcome and improve patient quality of life.l
References
|
1
|
Pan QJ, Hu SY, Guo HQ, et al: Liquid-based
cytology and human papillomavirus testing: a pooled analysis using
the data from 13 population-based cervical cancer screening studies
from China. Gynecol Oncol. 133:172–179. 2014.
|
|
2
|
Low EL, Simon AE, Lyons J, et al: What do
British women know about cervical cancer symptoms and risk factors?
Eur J Cancer. 48:3001–3008. 2012.
|
|
3
|
Banerjee R and Kamrava M: Brachytherapy in
the treatment of cervical cancer: a review. Int J Womens Health.
28:555–564. 2014.
|
|
4
|
Friedlander M and Grogan M; U.S.
Preventative Services Task Force. Guidelines for the treatment of
recurrent and metastatic cervical cancer. Oncologist. 7:342–347.
2002.
|
|
5
|
Kanayama T, Mabuchi S, Fujita M and Kimura
T: Calcaneal metastasis in uterine cervical cancer: a case report
and a review of the literature. Eur J Gynaecol Oncol. 33:524–525.
2012.
|
|
6
|
Pecorelli S: Revised FIGO staging for
carcinoma of the vulva, cervix, and endometrium. Int J Gynaecol
Obstet. 105:103–104. 2009.
|
|
7
|
Barmeir E, Langer O, Levy JI, Nissenbaum
M, DeMoor NG and Blumenthal NJ: Unusual skeletal metastases in
carcinoma of the cervix. Gynecol Oncol. 20:307–316. 1985.
|
|
8
|
Matsuyama T, Tsukamoto N, Imachi M and
Nakano H: Bone metastasis from cervix cancer. Gynecol Oncol.
32:72–75. 1989.
|
|
9
|
Ratanatharathorn V, Powers WE, Steverson
N, Han I, Ahmad K and Grimm J: Bone metastasis from cervical
cancer. Cancer. 73:2372–2379. 1994.
|
|
10
|
Thanapprapasr D, Nartthanarung A,
Likittanasombut P, et al: Bone metastasis in cervical cancer
patients over a 10-year period. Int J Gynecol Cancer. 20:373–378.
2010.
|
|
11
|
Abdul-Karim FW, Kida M, Wentz WB, et al:
Bone metastasis from gynecologic carcinomas: a clinicopathologic
study. Gynecol Oncol. 39:108–114. 1990.
|
|
12
|
Disibio G and French SW: Metastatic
patterns of cancers: results from a large autopsy study. Arch
Pathol Lab Med. 132:931–939. 2008.
|
|
13
|
Yoon A, Choi CH, Kim HJ, et al:
Contributing factors for bone metastasis in uterine cervical
cancer. Int J Gynecol Cancer. 23:1311–1317. 2013.
|
|
14
|
Pasricha R, Tiwari A, Aggarwal T and Lal
P: Carcinoma of uterine cervix with isolated metastasis to fibula
and its unusual behavior: report of a case and review of
literature. J Cancer Res Ther. 2:79–81. 2006.
|
|
15
|
Corrado G, Santaguida S, Zannoni G,
Scambia G and Ferrandina G: Femur metastasis in carcinoma of the
uterine cervix: a rare entity. Arch Gynecol Obstet. 281:963–965.
2010.
|
|
16
|
Malek M, Kanafi AR, Pourghorban R and
Nafisi-Moghadam R: Isolated humeral metastasis in uterine cervical
cancer: a rare entity. J Clin Imaging Sci. 2:802012.
|
|
17
|
Huh JW, Min JJ, Lee JH, Kim HR and Kim YJ:
The predictive role of sequential FDG-PET/CT in response of locally
advanced rectal cancer to neoadjuvant chemoradiation. Am J Clin
Oncol. 35:340–344. 2012.
|
|
18
|
Pomeranz SJ, Pretorius HT and Ramsingh PS:
Bone scintigraphy and multimodality imaging in bone neoplasia:
strategies for imaging in the new health care climate. Semin Nucl
Med. 24:188–207. 1994.
|
|
19
|
Sadik M, Suurkula M, Hoglund P, Jarund A
and Edenbrandt L: Improved classifications of planar whole-body
bone scans using a computer-assisted diagnosis system: a
multicenter, multiple-reader, multiple-case study. J Nucl Med.
50:368–375. 2009.
|
|
20
|
McQuay HJ, Carroll D and Moore RA:
Radiotherapy for painful bone metastases: a systematic review. Clin
Oncol (R Coll Radiol). 9:150–154. 1997.
|
|
21
|
Buccheri G, Ferrigno D and Tamburini M:
Karnofsky and ECOG performance status scoring in lung cancer: a
prospective, longitudinal study of 536 patients from a single
institution. Eur J Cancer. 32A:1135–1141. 1996.
|
|
22
|
Blythe JG, Cohen MH, Buchsbaum HJ and
Latourette HB: Bony metastases from carcinoma of cervix.
Occurrence, diagnosis, and treatment. Cancer. 36:475–484. 1975.
|
|
23
|
Dunstan CR, Felsenberg D and Seibel MJ:
Therapy insight: the risks and benefits of bisphosphonates for the
treatment of tumor-induced bone disease. Nat Clin Pract Oncol.
4:42–55. 2007.
|
|
24
|
Zhao Y, Wang JL, Wei LH and Bao DM:
Clinical analysis of eight cases of bone metastasis of uterine
carcinomas. Zhonghua Fu Chan Ke Za Zhi. 41:822–825. 2006.(In
Chinese).
|