Introduction
Adenoid cystic carcinoma is a rare, inert and
invasive tumor. The occurrence rate only accounts for 1% of head
and neck tumors and 22% of salivary gland tumors (1,2). The
carcinoma commonly occurs in the minor salivary gland of the upper
jaw, followed by the parotid and submandibular glands. Adenoid
cystic carcinoma tends to invade the nerves and cause distant
hematogenous metastasis (3), which
is usually observed in the lungs (4), whereas renal metastasis is commonly
observed in lung, breast and other cancers (5). Renal metastasis of a submandibular
gland adenoid cystic carcinoma is rare. In addition, adenoid cystic
carcinoma has a slow clinical progression and there is a long
survival time associated with the tumor. In clinical practice,
singular adenoid cystic carcinoma metastases are usually surgically
removed. Pre-operative whole-body positron emission tomography
(PET)/computed tomography (CT) is of great importance in the
treatment of distant metastases of adenoid cystic carcinoma,
particularly metastases to uncommon sites. The results of PET/CT
examination are valuable when making treatment plans (6). The present study reports the case of a
patient in whom a rare partial metastasis to the right kidney was
detected by whole-body PET/CT following previous surgery for a
submandibular gland adenoid carcinoma. Written informed consent was
obtained from the patient.
Case report
A 26-year-old male, who had undergone post-operative
radiotherapy for a left submandibular gland adenoid cystic
carcinoma three years previously, presented to Hubei Cancer
Hospital (Wuhan, China) the hospital due to an increasing level of
pain in the right side of the waist, which had persisted for 10
days. No other discomfort, such as hematuria or edema, was
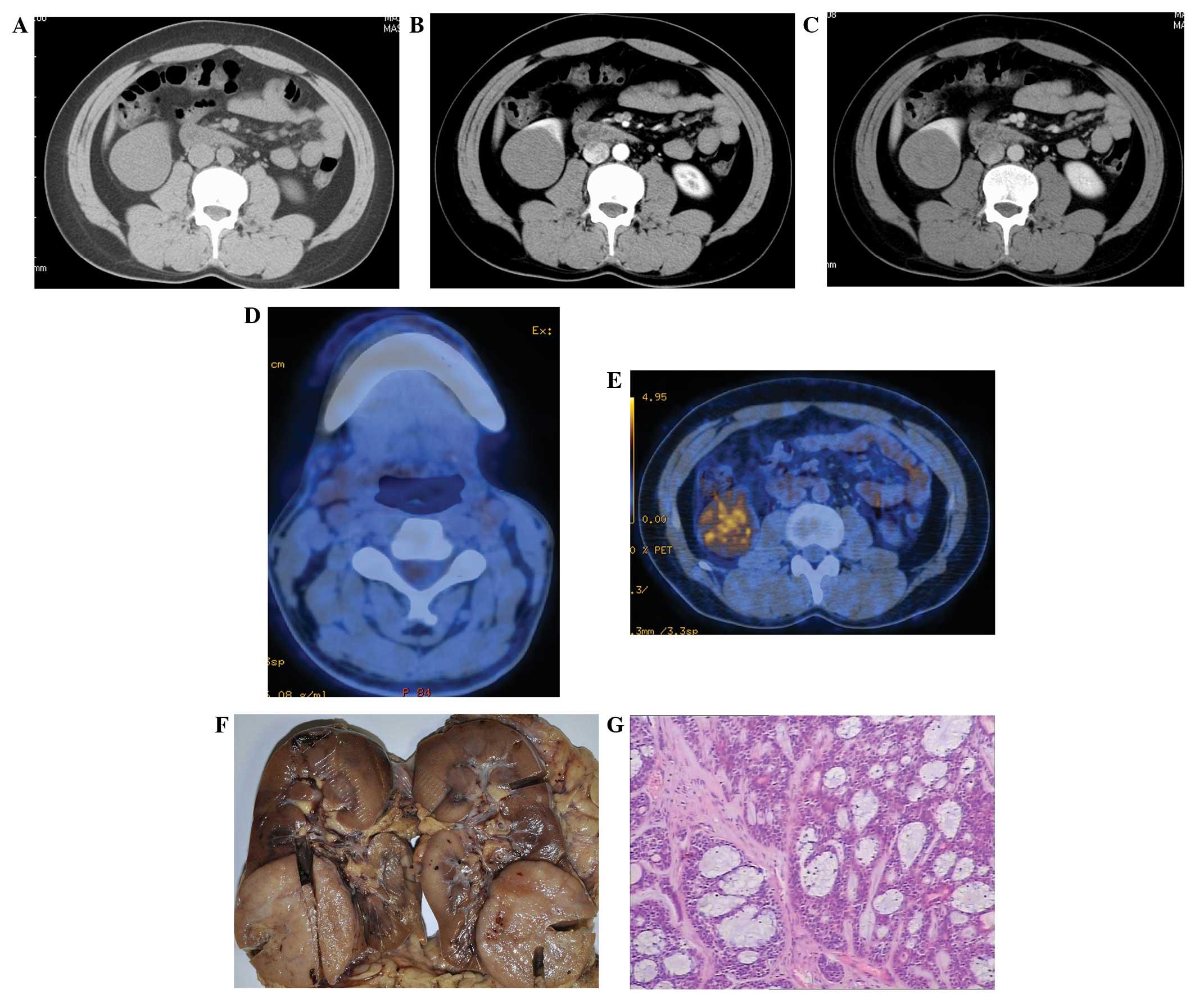
reported. Tests for tumor markers were found to be negative. An
enhanced CT scan revealed an enlarged right kidney with a slightly
lower-density mass that was 5.5×5.0×5.0 cm in size in the lower
right portion (Fig. 1A), with a CT
value of 36±5 HU. The mass had clear edges and an even density. A
slightly enhanced right kidney mass was observed in the arterial
phase (Fig. 1B), with a CT value of
48±5 HU. The degree of mass enhancement in the venous phase was
greater than that in the arterial phase (Fig. 1C), with a CT value of 68±5 HU. The
patient was diagnosed with a right kidney tumor using CT. On
PET/CT, post-operative changes were observed in the left
submandibular gland (Fig. 1D). The
imaging results for the kidneys were abnormal. A lump-shaped
moderate radioactive concentration shadow was observed in the lower
right kidney (Fig. 1E), with a
maximum standardized uptake value of 5.03. No evident abnormal
radioactive concentration shadow was observed in any other part of
the body. A right radical nephrectomy was performed at the Hubei
Cancer Hospital.
The right kidney was 15.0×15.0×10.0 cm in size at
the time of the surgery. A 5.0×6.0×5.0-cm hard mass could be
observed in the lower kidney (Fig.
1F), with a gray-white color and an intact tumor capsule.
However, the previously the normal capsule of lower kidney had been
invaded by the tumor. The renal fascia was smooth and no
significantly enlarged lymph nodes were observed in the renal
hilum. The finding from the examination of an intraoperative rapid
frozen section indicated an epithelial malignant tumor. Based on
the post-operative hematoxylin-eosin staining, which was compatible
with a right kidney adenoid cystic carcinoma (Fig. 1G), combined with the patient’s
medical history, a renal metastasis of the submandibular gland
adenoid cystic carcinoma was considered to be the diagnosis. The
mass was resected and the patient received no further
treatment.
Discussion
Based on autopsy reports, the incidence rate of
renal metastasis is 3–15%, and this mainly originates from lung
(19.8–23.3%), mammary gland (12.3%), stomach (11.1–15.1%) and colon
cancers (22.2%) and melanoma (14.8%) (5,7). Renal
metastasis is caused by hematogenous metastases of primary tumors,
usually multiple or multifocal. The patient in the present case
only presented with a singular metastasis in the lower right
kidney, which made the mass difficult to clinically diagnose.
Submandibular gland adenoid cystic carcinoma is rare and to the
best of our knowledge, has never been reported in the literature.
Metastatic renal carcinoma does not have clear symptoms or exhibit
hematuria in the majority of cases. In the present case, the
patient exhibited no clear clinical symptoms, with the exception of
an increasing level of pain in the right side of the waist.
Microscopic hematuria has a low incidence rate in metastatic renal
carcinoma. This is mainly due to the renal metastasis being located
in the vascular plexus cortex adjacent to the glomeruli, therefore,
it relatively infrequently invades the urothelium (8). The patient in the present case did not
have evident urinary symptoms. Only the increasing pain level in
the waist was observed, caused by the large tumor size stimulating
the renal fascia.
Diverse CT features of renal metastasis have been
reported in the literature, mainly presenting as solid or cystic
masses and hemorrhagic or diffuse lesions (8). The patient in the present case
possessed a singular solid mass with a slightly lower density, as
revealed by a CT scan. The mass had clear edges. The lesion was
large and shared an indistinct boundary with the kidney capsule.
Angiography of the renal metastasis revealed a hypovascular tumor.
The majority of renal metastases are slightly enhanced, according
to the literature (9). The present
patient had a slightly enhanced lower right kidney mass in the
arterial phase of CT enhancement (mean CT value, 36±5 HU; CT value
in the arterial phase, 48±5 HU). The degree of mass enhancement in
the venous phase was greater compared with the arterial phase (mean
CT value, 68±5 HU). The enhancement pattern was different to that
of classic primary renal carcinoma. The hemodynamic features of
primary renal carcinoma exhibit a fast-in, fast-out enhancement
pattern, with cancellation of the contrast agent in the venous
phase (10). Therefore, the
analysis of the enhancement features of this lesion provided the
basis for the clinical diagnosis in the present study.
The 18F-fluorodeoxyglucose
(18F-FDG) PET features of metastatic renal carcinoma are
relatively infrequently reported in the literature (11). The patient in the present case
mainly exhibited high FDG intake, indicating a significantly
increased glucose intake by the tumor. Thus, diagnosis of a
malignant lesion was considered. However, it remained difficult to
determine whether the tumor was a primary or metastatic renal
carcinoma. Metastatic renal carcinoma is usually a manifestation of
malignant tumor systemic metastasis, normally with metastases in
other parts of the body. However, in the present case, the only
lesion identified was in the right kidney, and this was found
through systemic PET/CT examination. Eventually a surgical
resection treatment plan was clinically developed. In conclusion,
careful analysis of multiple imaging findings combined with a
review of the medical history of a patient could increase the
accuracy of imaging diagnosis. PET/CT findings provide an essential
basis for making treatment plans for renal metastasis.
References
|
1
|
Jaso J and Malhotra R: Adenoid cystic
carcinoma. Arch Pathol Lab Med. 135:511–515. 2011.
|
|
2
|
Kokemueller H, Eckardt A, Brachvogel P and
Hausamen JE: Adenoid cystic carcinoma of the head and neck - a 20
years experience. Int J Oral Maxillofac Surg. 33:25–31. 2004.
|
|
3
|
Barrett AW and Speight PM: Perineural
invasion in adenoid cystic carcinoma of the salivary glands: a
valid prognostic indicator? Oral Oncol. 45:936–940. 2009.
|
|
4
|
Manoharan M, Gomez P, Reyes MA and Soloway
MS: Metastatic adenoid cystic carcinoma to the kidney in a young
woman. Urology. 68:1343.e11–1343.e12. 2006.
|
|
5
|
Pagani JJ: Solid renal mass in the cancer
patient: second primary renal cell carcinoma versus renal
metastasis. J Comput Assist Tomogr. 7:444–448. 1983.
|
|
6
|
Tewari A, Padma S and Sundaram PS:
Detection of atypical metastases in recurrent adenoid cystic
carcinoma of parotid gland. J Cancer Res Ther. 9:148–150. 2013.
|
|
7
|
Choyke PL, White EM, Zeman RK, Jaffe MH
and Clark LR: Renal metastases: clinicopathologic and radiologic
correlation. Radiology. 162:359–363. 1987.
|
|
8
|
Honda H, Coffman CE, Berbaum KS, et al: CT
analysis of metastatic neoplasms of the kidney. Comparison with
primary renal cell carcinoma. Acta Radiol. 33:39–44. 1992.
|
|
9
|
Bailey JE, Roubidoux MA and Dunnick NR:
Secondary renal neoplasms. Abdom Imaging. 23:266–274. 1998.
|
|
10
|
Macari M and Bosniak MA: Delayed CT to
evaluate renal masses incidentally discovered at contrast-enhanced
CT: demonstration of vascularity with deenhancement. Radiology.
213:674–680. 1999.
|
|
11
|
Ho L, Wassef H, Henderson R and Seto J:
Renal metastasis from primary colon cancer on FDG- PET-CT. Clin
Nucl Med. 34:596–597. 2009.
|