Introduction
Carcinosarcoma of the breast is a malignant
sarcomatoid metaplasia of epithelial carcinoma. It is defined as a
mixed tumor containing carcinomatous and malignant nonepithelial
components of mesenchymal origin without a transitional zone
between them. Carcinosarcoma exhibits different behavior when
compared with carcinomas or sarcomas of the breast and is rare,
accounting for <0.1% of all breast malignancies, worldwide
(1). Bone metastasis with breast
carcinosarcoma is particularly uncommon. In the current study, a
case of breast carcinosarcoma and intraductal carcinoma occurring
simultaneously in the right breast of a patient exhibiting multiple
bone metastases is presented. Written informed consent was obtained
from the patient’s family.
Case report
A 51-year-old Mongolian female presented to the
Department of Medical Oncology of the Second Affiliated Hospital of
Zhejiang University (Hangzhou, China) with the complaint of lumbago
that had persisted for two months. The patient’s first-degree
relatives had no history of cancer. On physical examination, a
0.5×0.5-cm mass was identified in the right breast near the areola.
Bilateral axillary examination revealed no lymphadenopathy.
Sonography detected two masses near the areola of the right breast;
one mass measured 0.6×0.5 cm and the second mass measured 0.9×0.6
cm and was proximal to the ectopectoralis. Ultrasound examination
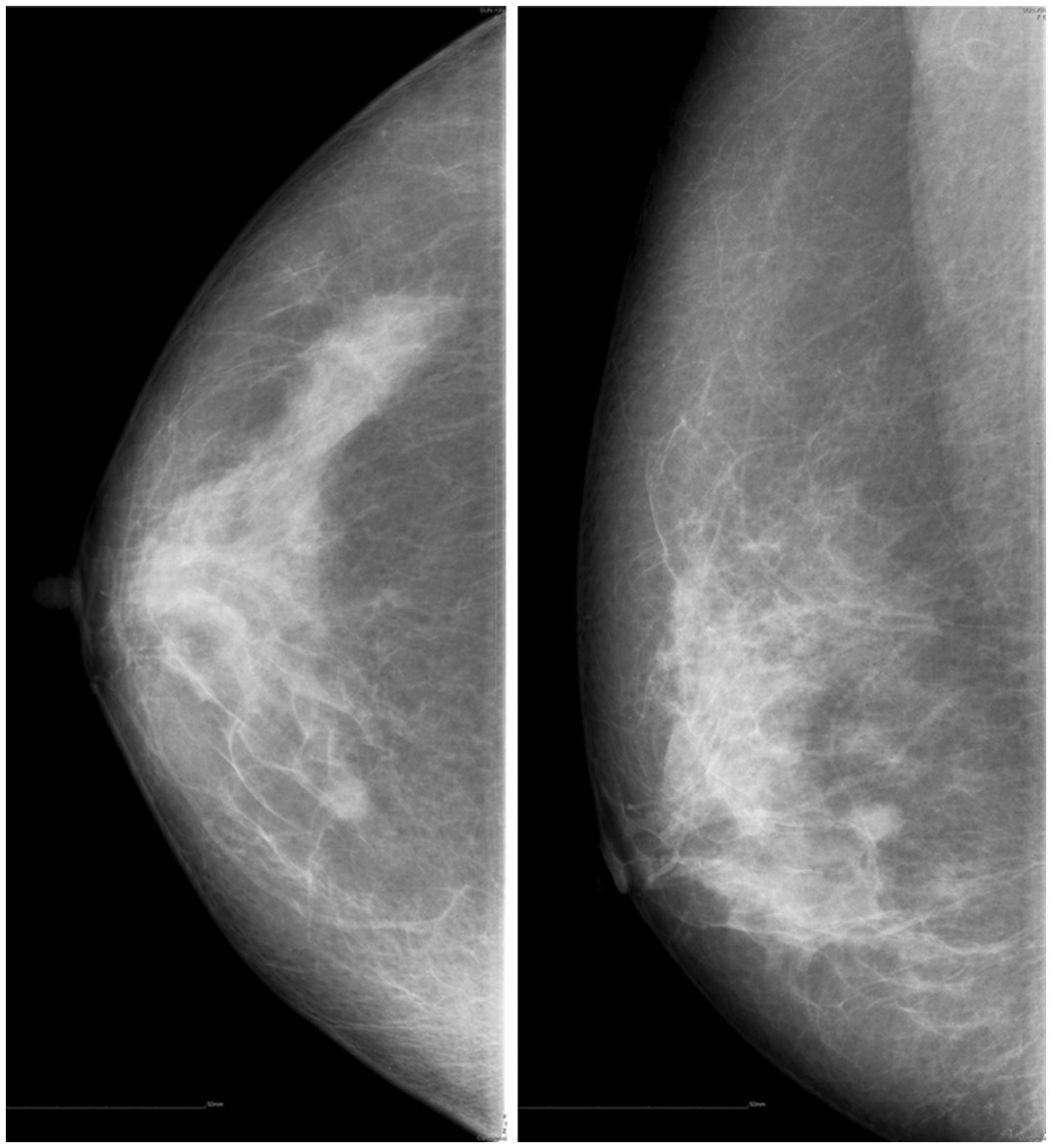
of the bilateral axillary fossa was unremarkable. However, the
patient’s mammogram was abnormal and revealed two masses in the
right breast, which were situated in the upper inner and upper
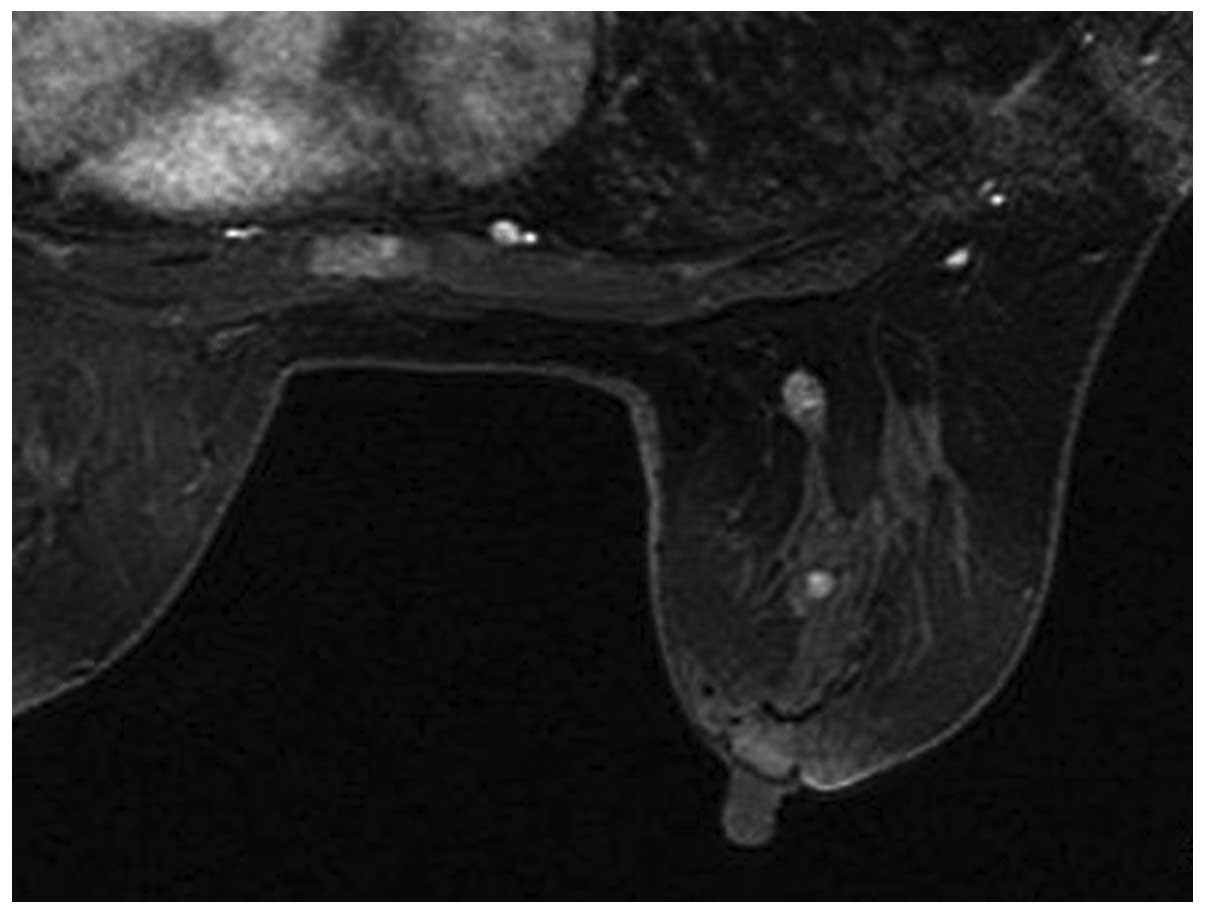
outer quadrants (Fig. 1). Magnetic
resonance imaging (MRI) of the breast also revealed two nodules
near the areola of the right breast (Fig. 2). The first node was 7 mm in
diameter and located within the catheter, 30 mm from the nipple and
was enhanced significantly following injection of a contrast agent.
The second node was 8 mm in diameter and was proximal o the basilar
section of the right breast. Positron emission tomography/computed
tomography revealed an 8.1-mm soft tissue nodule with a sublobe in
the upper inner quadrant of the right breast (maximum standardized
uptake volume, 3.46). Radioactive enhancement was observed in
multiple bones (each side of the scapula and femur, the sternum,
the left eighth rib, and between the ninth thoracic and second
sacral vertebrae). Based on these results, the primary diagnosis
was determined as breast cancer with bone metastases.
A lumpectomy biopsy was performed to verify the
diagnosis. One 0.8×0.6-cm mass was identified in the upper inner
quadrant of the right breast. Pathological results indicated
intraductal carcinoma [estrogen receptor (ER) +, progesterone
receptor (PR) +, CerbB2 −, p63 + and E-cadherin +]. The other mass
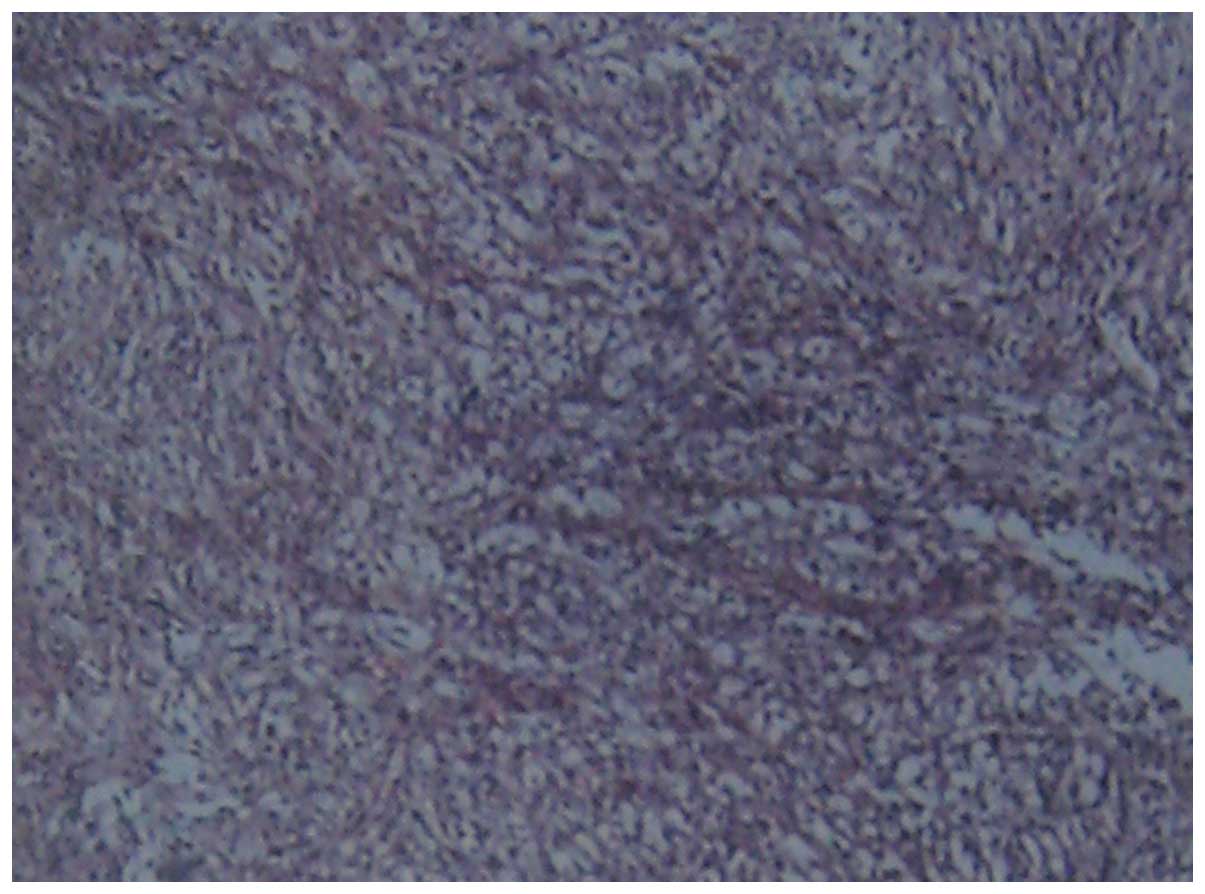
(diameter, 0.5 cm) was excised from the upper outer quadrant of the
right breast. Histological and immunohistochemical examinations
determined a diagnosis of a malignant phyllodes tumor with invasive
and poorly differentiated carcinoma (Fig. 3). Immunohistochemical examinations
demonstrated no positivity for hormonal receptors or CerbB2,
however, positivity was identified for vimentin [cytokeratin (CK)7
−, CK20 −, CK5/6 −, ER −, PR −, CerbB2 −, p63 +, vimentin +,
cluster of differentiation 10 −, cancer antigen (CA)-125 −, CA15-3
+, CK18 +, smooth muscle actin −, gross cystic disease fluid
protein 15 −, CK34BE12 −, E-cadherin +, thyroglobulin − and thyroid
transcription factor-1 −]. Similar pathological results were
identified by a biopsy of the fourth lumbar spinous process and the
final diagnosis was determined to be breast carcinosarcoma
(pT1N0M1, stage IV) according to the 7th edition of the American
Joint Committee on Cancer cancer staging manual (2). One cycle of a chemotherapy regimen
(lasting 21 days) comprising of cisplatin (40 mg, days 1–3),
doxorubicin (70 mg, day 1) and cyclophosphamide (0.8 g, day 1) was
administered. However, the patient suffered from febrile
neutropenia and septic shock ten days after completing chemotherapy
and succumbed after a month.
Discussion
Breast carcinosarcoma is a rare malignancy. Patients
often present with swelling of the breast or, more often with a
large palpable mass on clinical examination. In rare cases, nipple
discharge and retraction, or a skin ulceration may be present
(3). In the patient described in
the current case, lumbago was the only symptom. One small mass was
palpable on physical examination. Two small masses (diameters,
<1 cm) were identified by mammography and MRI. The mass had not
been identified by the patient. Hematogenous spread is the most
common route of metastasis, and the lungs and pleura are the most
common sites of distant metastasis (4). Bone metastasis from breast
carcinosarcoma has been presented in a small number of studies
(5,6). Yang et al (6) observed bone metastasis in only one of
25 patients who had undergone surgical treatment. To the best of
our knowledge, the current case is the first report of breast
carcinosarcoma presenting concurrently with bone metastases. The
particularly rare instance of an intraductal carcinoma presenting
in the same breast was also identified.
The prognosis of breast carcinosarcoma is poor
(7). It exhibits different behavior
compared with carcinoma or sarcoma of the breast and is associated
with a worse prognosis than classical breast carcinoma (8). The overall five-year survival rate is
only 49% (9). Clinicopathological
parameters, including tumor size, differentiation rate, a high
histological grade, atypia and active pleomorphic spindle cells are
important in prognosis (10).
However, no significant difference was identified when breast
carcinosarcoma was compared with high-grade receptor-negative
infiltrative carcinomas (11).
Hennessy et al (12)
examined 100 patients that presented with biphasic metaplastic
sarcomatoid carcinoma and 98 patients that exhibited
carcinosarcoma, which were identified using the Surveillance,
Epidemiology, and End Results database. The five-year overall
survival rates at stages I, II, III, and IV were identified to be
0.73, 0.59, 0.44 and 0.00, respectively. The patient in the present
study survived for only five months following the occurrence of
lumbago.
Treatment strategies for carcinosarcoma are similar
to those for breast cancer. For early stage patients, modified
radical mastectomy is an efficient and practical method in the
treatment of breast carcinosarcoma (13,14).
Axillary dissection is usually performed during the surgical
procedure, as the axillary nodes are one of the typical sites of
metastasis (incidence, 26%) from either the carcinomatous or
sarcomatous components (15). For
patients that are late stage, chemotherapy and radiotherapy may be
administered in various combinations. Evidence from existing
clinical studies regarding adjuvant chemotherapy in common types of
breast cancer indicates that anthracycline/taxane-based therapeutic
combinations may be more effective than
non-anthracycline/taxane-based chemotherapy. However, it appears
that metaplastic breast cancer is less responsive to therapy that
is comprised of conventional regimens, which are used for typical
adenocarcinoma of the breast. Hormone therapy is not recommended
due to the negative expression of hormone receptors and human
epidermal growth factor receptor 2 in the majority of cases
(16). In the present case, the
hormone receptors stained negative during immunohistochemical
analysis, and tamoxifen and aromatase inhibitors were not
recommended. Due to the occurrence of multiple bone metastases,
radiotherapy was not considered. The patient received palliative
chemotherapy (21 day cycle) with cisplatin (40 mg, days 1–3),
doxorubicin (70 mg, day 1), and cyclophosphamide (0.8 g, day 1) and
the response was poor. Previous studies have indicated no survival
advantage for patients treated with either chemotherapy or
radiation for metastatic carcinosarcoma (17). However, the precise effects of
chemotherapy or radiotherapy on breast carcinosarcoma remain
unclear due to the rarity of such cases.
In conclusion, carcinosarcoma of the breast is rare
and thus, few reports regarding this disease exist. Novel
therapeutic agents are required to improve prognosis and further
biological studies are required to identify potential molecular
targets.
Acknowledgements
The present study was supported by the National
Natural Science Foundation of China (grant nos. 81000945, 81101477
and 81102012).
References
|
1
|
Gutman H, Pollock RE, Janjan NA and
Johnston DA: Biologic distinctions and therapeutic implications of
sarcomatoid metaplasia of epithelial carcinoma of the breast. J Am
Coll Surg. 180:193–199. 1995.
|
|
2
|
Edge SB, Byrd DR, Compton CC, et al: AJCC
Cancer Staging Manual. 7th edition. Springer-Verlag; New York, NY:
2010
|
|
3
|
Beatty JD, Atwood M, Tickman R and Reiner
M: Metaplastic breast cancer: clinical significance. Am J Surg.
191:657–664. 2006.
|
|
4
|
Kijima Y, Umekita Y, Yoshinaka H, et al: A
case of breast carcinoma with cartilaginous and osseous metaplasia.
Breast Cancer. 13:214–219. 2006.
|
|
5
|
Kurian KM and Al-Nafussi A:
Sarcomatoid/metaplastic carcinoma of the breast: a
clinicopathological study of 12 cases. Histopathology. 40:58–64.
2002.
|
|
6
|
Yang YF, Liu J, Fang ZY and Gu L: Clinical
features and prognosis of 25 cases of breast carcinosarcoma.
Zhonghua Zhong Liu Za Zhi. 34:620–623. 2012.(In Chinese).
|
|
7
|
Suspitsin EN, Sokolenko AP, Voskresenskiy
DA, et al: Mixed epithelial/mesenchymal metaplastic carcinoma
(carcinosarcoma) of the breast in BRCA1 carrier. Breast Cancer.
18:137–140. 2011.
|
|
8
|
Foschini MP, Dina RE and Eusebi V:
Sarcomatoid neoplasms of the breast: proposed definitions for
biphasic and monophasic sarcomatoid mammary carcinomas. Semin Diagn
Pathol. 10:128–136. 1993.
|
|
9
|
Tokudome N, Sakamoto G, Sakai T, et al: A
case of carcinosarcoma of the breast. Breast Cancer. 12:149–153.
2005.
|
|
10
|
Esses KM, Hagmaier RM, Blanchard SA,
Lazarchick JJ and Riker AI: Carcinosarcoma of the breast: two case
reports and review of the literature. Cases J. 2:152009.
|
|
11
|
Ilhan E, Vardar E, Ozkok G, et al: A rare
tumour of the breast: carcinosarcoma. J Clin Med Res. 2:96–98.
2010.
|
|
12
|
Hennessy BT, Giordano S, Broglio K, et al:
Biphasic metaplastic sarcomatoid carcinoma of the breast. Ann
Oncol. 17:605–613. 2006.
|
|
13
|
Stefaniuk CM and Jones T: Double feature:
carcinoma and sarcoma present in a single breast tumor. Case Rep
Oncol Med. 2012:2328512012.
|
|
14
|
Santiago Pérez JT, Pérez Vázquez MR, de
Rivera Valdespino AL and Gil Valdés D: Carcinosarcoma of the
breast: a tumour with controversial histogenesis. Clin Transl
Oncol. 7:255–257. 2005.(In Spanish).
|
|
15
|
Wada H, Enomoto T, Tsujimoto M, Nomura T,
Murata Y and Shroyer KR: Carcinosarcoma of the breast:
molecular-biological study for analysis of histogenesis. Hum
Pathol. 29:1324–1328. 1998.
|
|
16
|
Tse GM, Tan PH, Putti TC, Lui PC, Chaiwun
B and Law BK: Metaplastic carcinoma of the breast: a
clinicopathological review. J Clin Pathol. 59:1079–1083. 2006.
|
|
17
|
Wargotz ES and Norris HJ: Metaplastic
carcinomas of the breast. III Carcinosarcoma. Cancer. 64:1490–1499.
1989.
|