Introduction
Keratocystic odontogenic tumors (KCOTs) are benign
tumors that comprise ~11% of all cysts of the jaws, worldwide
(1–2). KCOTs are characterized by aggressive
behavior and a high recurrence rate following surgical treatment.
The disease commonly occurs between the ages of 10–30 years,
predominantly in the mandibular molar region and ascending ramus
(2). KCOTs are often asymptomatic,
however, patients may occasionally present with swelling, pain and
discharge (3–5). A number of therapies have been used in
the management of KCOTs. Conservative treatments include simple
enucleation, with or without curettage, decompression and
marsupialization. Aggressive treatments, including peripheral
osteotomy, cryotherapy with liquid nitrogen and resection, have
also been reported (6). For the
optimum management, it is necessary to assess the full extent of
the lesion by a computed tomography (CT) scan. The present study
reports the case of a patient with a giant KCOT involving the right
zygoma and maxillary sinus, which was treated using a modified
method (7,8). In this treatment modality, grinding of
the peripheral bone and cryotherapy were used following enucleation
in order to remove potentially remaining tumor tissue. Written
informed consent was obtained from the patient.
Case report
A 25-year-old male presented to the Qingdao
Municipal Hospital (Shandong, China) with a two-month history of
painless swelling on the right side of the face. The medical
history of the patient was unremarkable. On clinical examination, a
large swelling was identified on the right side of the face that
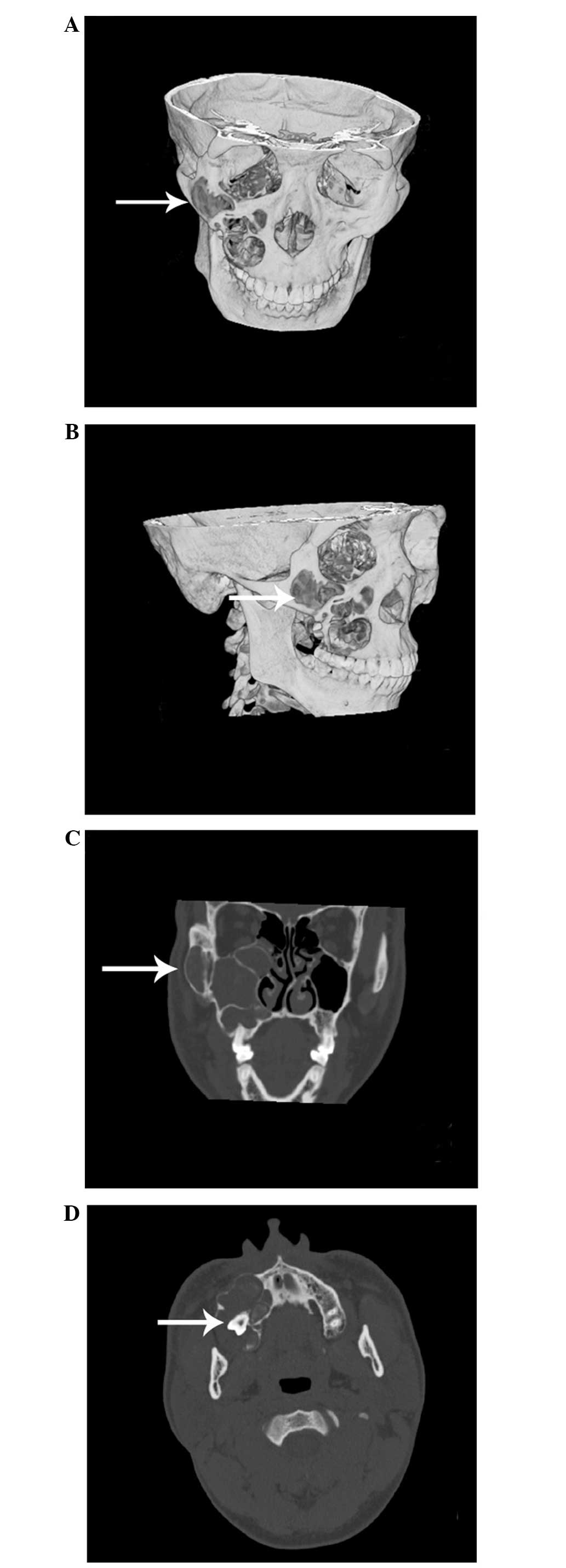
was hard and bony on palpitation. A CT scan revealed a giant,
multilocular and hypodense lesion of ~6.5×5.0 cm in size, with a
well-defined margin (Fig. 1). The
lesion involved the majority of the right maxillary bone, maxillary
sinus and zygomatic bone. The third molar tooth was completely
impacted (Fig. 1). Based on these
observations, a tentative diagnosis of a cyst was proposed.
Under general anesthesia, the lesion was enucleated
as a whole, using the Caldwell-Luc approach. The tooth that was
associated with the lesion was simultaneously removed to avoid
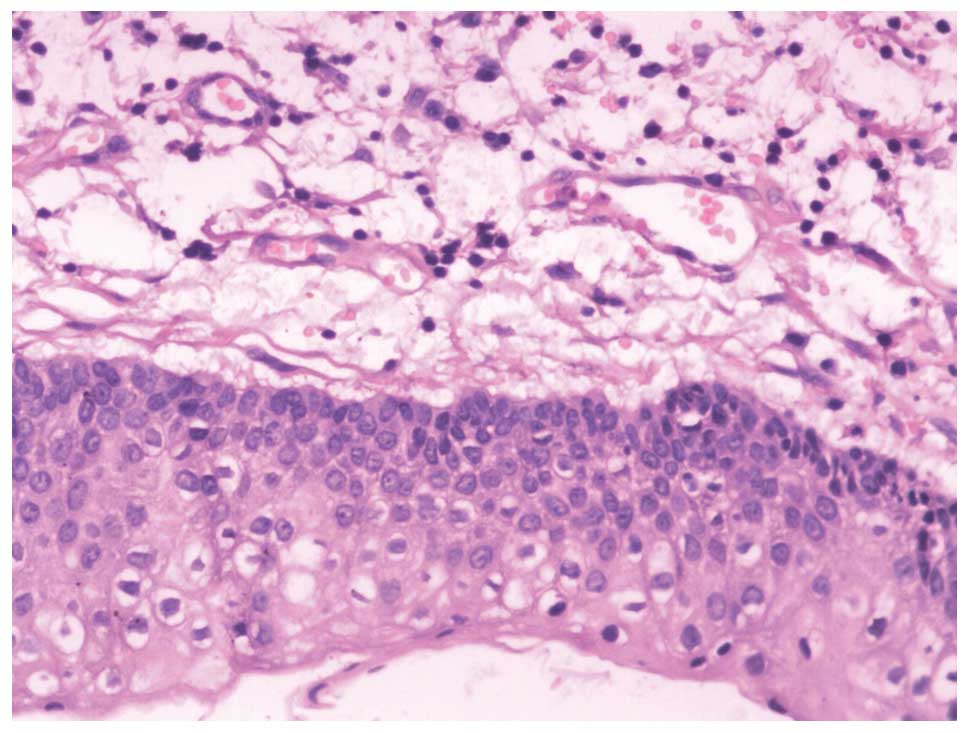
tumor fragmentation. Histological examination during the procedure
identified a cystic tumor. The wall of the cyst was lined with a
stratified squamous epithelium and a corrugated keratinized lining
(Fig. 2). A diagnosis of KCOT was
determined. To eliminate the possibility of residual cystic tissue,
the margin surrounding the lesion was ground and then frozen with
liquid nitrogen three times. Prior to the freezing of the surgical
site, the adjacent tissues were protected using dry gauze pads.
Subsequently, the patient exhibited a good recovery and no
recurrence has been observed within the eight-month follow-up
duration.
Discussion
KCOTs are benign, unilocular or multilocular, but
locally aggressive, developmental cystic neoplasms that were first
described by Philipsen in 1956 (8).
KCOTs are believed to arise from the dental lamina and are
associated with impacted teeth. KCOTs can present as solitary or
multiple lesions; the latter is usually one of the components of
inherited naevoid basal cell carcinoma syndrome. PTCH, a tumor
suppressor gene located on chromosome 9q22.3-q31, is associated
with the development of KCOTs (5).
This gene is part of the Hedgehog signaling pathway and has been
revealed to be associated with several epithelial tumors,
suggesting that the disease is neoplastic in nature (4).
Clinically, the majority of patients with KCOTs
present with pain, swelling, a mass with discharge or aggressive
growth or localized asymptomatic swelling. KCOTs occur most
frequently in the mandible, accounting for 65–83% of cases.
Overall, <1% of KCOTs occur in the sinus (9). In the present case, the involvement of
the giant KCOT with the majority of the zygoma and maxillary sinus
was unusual. To the best of our knowledge, this is the only
reported case in the English literature. KCOTs most often grow
along the anterior-posterior direction within the jaws, without
causing evident bone expansion, leading to the delayed appearance
of symptoms and clinical signs (10). Thus, the tumor may reach a size as
large as that reported in the current study. In addition, the
extremely large size and the involvement of the zygoma suggest that
there was aggressive expansion of the tumor in the present
case.
Although various treatment modalities have been used
in the management of KCOTs, the most effective treatment remains
controversial. Blanas et al (11) reviewed treatment options for KCOTs,
including simple curettage, enucleation, marsupialization and
resection. All of these treatments may lead to recurrence, with the
exception of resection (12). In
previous years, there has been a tendency to use decompression and
irrigation to prevent recurrence of the disease. The benefits of
this technique are due to the minimal surgical morbidity and the
decreased damage to the associated structures (13). In the present case, the cystic tumor
was extremely large in size and invaded the majority of the
zygomatic-maxillary complex. Therefore, the modality of
decompression of the cyst was not selected due to the lower repair
capacity of the maxillary sinus compared with the other
maxillofacial bones. A modified treatment was used in the present
case to prevent the recurrence of the tumor. Following conventional
enucleation, the thin bone around the lesion was ground with a
drill and frozen with liquid nitrogen to eliminate potential
residual cystic tissue or satellite microcysts. In contrast to
Carnoy’s solution, liquid nitrogen can induce cell necrosis and
preserve inorganic bone structures, which destroys osteogenic and
osteoconductive properties (14).
This cryotherapy technique preserves the bone framework and leads
to improved repair and bone height recovery. In the eight-month
follow-up period, no recurrence of the KCOT was observed. A
long-term follow-up, however, is required.
In conclusion, KCOT involving the zygoma, usually
caused by a large tumor size, is extremely rare. In the present
case, a modified treatment with enucleation, grinding and
cryotherapy was demonstrated to be an effective treatment for KCOT.
Resection of a large-sized tumor may not be adequate as it may
cause extensive tissue destruction. The results of the present
study indicate that modified treatment may present a reasonable
treatment option for giant KCOTs.
References
|
1
|
Eryilmaz T, Ozmen S, Findikcioglu K,
Kandal S and Aral M: Odontogenic keratocyst: an unusual location
and review of the literature. Ann Plast Surg. 62:210–212. 2009.
|
|
2
|
Praetorius F and Ledesma-Montes C:
Calcifying cystic odontogenic tumour. World Health Organization
classification of tumours (Pathology and genetics of head and neck
tumours). Barnes L, Eveson JW, Reichart P and Sidransky D: IARC
press; Lyon, France: pp. 3132005
|
|
3
|
Bodner L, Shohat S and Ulmansky M: Unusual
cyst of the zygoma. J Oral Maxillofac Surg. 40:229–231. 1982.
|
|
4
|
Bhargava D, Deshpande A and Pogrel MA:
Keratocystic odontogenic tumour (KCOT) - a cyst to a tumour. Oral
Maxillofac Surg. 16:163–170. 2012.
|
|
5
|
Madras J and Lapointe H: Keratocystic
odontogenic tumour: reclassification of the odontogenic keratocyst
from cyst to tumour. Tex Dent J. 125:446–454. 2008.
|
|
6
|
Ghali GE and Connor MS: Surgical
management of the odontogenic keratocyst. Oral Maxillofac Surg Clin
North Am. 15:383–392. 2003.
|
|
7
|
Tolstunov L and Treasure T: Surgical
treatment algorithm for odontogenic keratocyst: combined treatment
of odontogenic keratocyst and mandibular defect with
marsupialization, enucleation, iliac crest bone graft, and dental
implants. J Oral Maxillofac Surg. 66:1025–1036. 2008.
|
|
8
|
Philipsen HP: Om keratocystedr
(Kolesteratomer) and kaeberne. Tandlaegebladet. 60:963–971.
1956.(In Danish).
|
|
9
|
Voorsmit RA, Stoelinga PJ and van Haelst
UJ: The management of keratocysts. J Maxillofac Surg. 9:228–236.
1981.
|
|
10
|
Güler N, Sençift K and Demirkol O:
Conservative management of keratocystic odontogenic tumors of jaws.
Scientific World Journal. 2012:6803972012.
|
|
11
|
Blanas N, Freund B, Schwartz M and Furst
IM: Systematic review of the treatment and prognosis of the
odontogenic keratocyst. Oral Surg Oral Med Oral Pathol Oral Radiol
Endod. 90:553–558. 2000.
|
|
12
|
Gustafson G, Lindahl B, Dahl E and
Svensson A: The nevoid basal cell carcinoma syndrome - Gorlin’s
syndrome. Multiple jaw cysts and skin cancer. Swed Dent J.
13:131–139. 1989.
|
|
13
|
Cakur B, Miloglu O, Yolcu U, Göregen M and
Gürsan N: Keratocystic odontogenic tumor invading the right
maxillary sinus: a case report. J Oral Sci. 50:345–349. 2008.
|
|
14
|
Tonietto L, Borges HO, Martins CA, Silva
DN and Sant’Ana Filho M: Enucleation and liquid nitrogen
cryotherapy in the treatment of keratocystic odontogenic tumors: a
case series. J Oral Maxillofac Surg. 69:e112–e117. 2011.
|