Introduction
Extraskeletal osteosarcoma (ESOS) is a rare and
highly invasive tumor (1–3,5–8).
Retroperitoneal ESOS is usually diagnosed at an advanced stage due
to the insidious onset (2–9). The lungs and liver are the most common
sites of metastases (1,7–10). The
present study reports a case of gastric parietal implantation
metastasis and peritoneum multiple metastases on retroperitoneal
ESOS. The literature on retroperitoneal ESOS is also reviewed.
Case report
A 52-year-old male was hospitalized with
intermittent pain in the right abdomen that had persisted for one
week. The medical history revealed hypertension, but no history of
trauma and radiation exposure or a family history of genetic
diseases. Physical examination showed a large, hard, immobile mass
with a smooth surface, ~6×6 cm in size. Laboratory tests revealed a
small increase in the serum creatinine level to 120 μmol/l (normal
range, 40–110 μmol/l), while the remaining results, including that
for alkaline phosphatase (ALP), were normal. An abdominal computed
tomography (CT) scan (Fig. 1)
showed a large, dense mass, with calcification, located below the
right kidney, an oppressed upper ureter and thickening of the renal
fascia. An exploratory laparotomy discovered a stiff calcified
immobile retroperitoneal mass of 5×6 cm, with a wide base below the
right kidney. The mass could not be completely resected of its
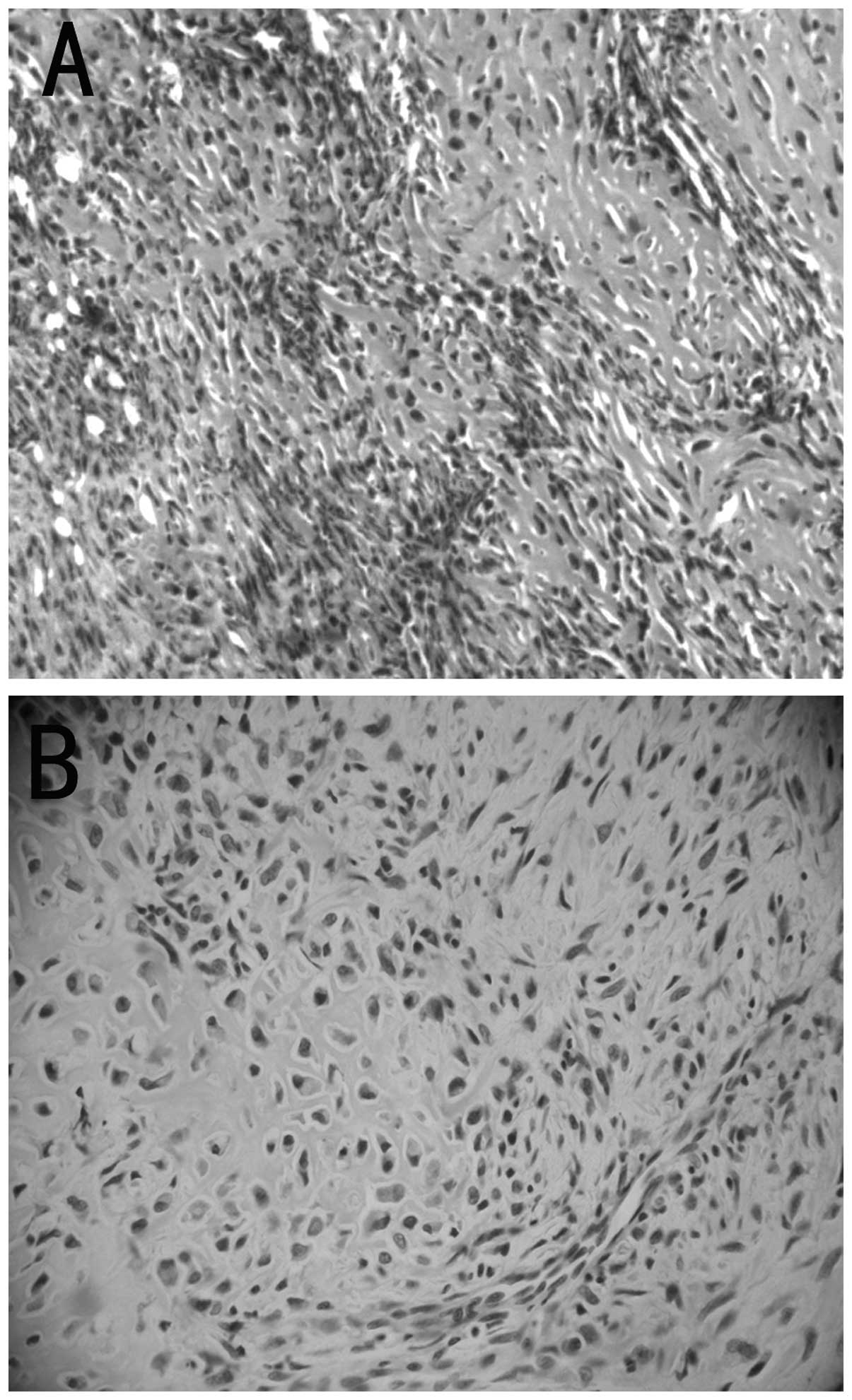
attachment to the surrounding organs. Pathology revealed that the
tumor was composed of spindle- and polygonal-shaped tumor cells,
with a banded or irregular osteoid matrix. The tumor cells
exhibited varying degrees of atypia and visible mitotic figures
(Fig. 2). From these results, a
diagnosis of extraskeletal osteosarcoma was formed.
Immunohistochemistry showed the positive expression of vimentin and
S-100, whereas examination of cytokeratin, cluster of
differentiation (CD)117, CD34, epithelial membrane antigen,
melanoma, B-cell lymphoma-2 and CD99 staining was negative.
Two months after the surgery, CT imaging (Fig. 1B) revealed a retroperitoneal ESOS
near the right upper ureter, with a large amount of calcification.
The imaging also revealed multiple metastases of the hepatic
capsular, renal fascia and peritoneum. After four months, the
patient underwent a second exploratory laparotomy due to tumor
relapse. The surgery demonstrated that the retroperitoneal mass of
~10×10 cm in size was closely adhered to the right kidney,
ileocecum and the posterior abdominal wall. There was significant
chondroid tissue present on the omental tumors, which were 0.5×1.5
cm in size. Only the omental metastases were cut, and cytoreductive
surgery was not viable due to the multiple metastases of the
abdominal cavity and the severe adhesion with the retroperitoneal
tissue. Pathological examination showed that the tumor tissue was
predominantly composed of spindle-shaped cells and differentiated
immature bone tissue. The cells showed mild-moderate atypia and
were ordered in a storiform arrangement, with visible mitotic
figures. From these results, a diagnosis of an omental osteosarcoma
was formed.
The patient was administered two courses of
chemotherapy, where each cycle lasted 28 days. During each cycle
Endostar (15 mg/day for the first 14 days), cisplatin (100
mg/m2 on the first day) and epirubicin (25
mg/m2 for the first three days) were administered
intravenously, but this had minimal efficacy. Five months after the
second surgery, the patient experienced vomiting and an incomplete
intestinal obstruction was suspected. The patient therefore
underwent a third exploratory laparotomy. The surgery revealed a
25×30-cm right retroperitoneal mass oppressing the descending
section of the duodenum and surrounded the descending colon, and a
1.1×1.2-cm implantation metastasis nodule in the outer membrane of
the gastric body anterior wall (Fig.
1C). The liver and spleen exhibited no metastatic nodules. A
gastrojejunostomy and ileocolonic anastomosis were performed, and
the pathology (Fig. 2B) revealed
components of an osteosarcoma in the outer stomach wall, in
accordance with a gastric wall osteosarcoma metastasis. The serum
ALP level gradually increased to 199 U/l (normal range, 40–130
U/l). The patient eventually succumbed to retroperitoneal ESOS one
year after the first surgery.
Discussion
ESOS represents <4% of all osteosarcomas and 1–2%
of all soft-tissue sarcomas (1–3). There
is a male bias for osteosarcoma, and the gender ratio is 1.9:1.0
(2). The most common sites of ESOS
are the soft tissues of the limbs and the retroperitoneum (11). Retroperitoneal ESOS is a typical
osteosarcoma, identified in the retroperitoneal soft tissue with no
attachment to the bones or bone periosteum, and producing osteoid
or cartilage matrix (12). The
incidence rate of retroperitoneum ESOS accounts for 17% of ESOS
(8,13). ESOS occurs predominantly in elderly
individuals over 50 years old, which differs from osteosarcoma
(14). In total, 10 cases of
retroperitoneal ESOS, including the present case, have been
reported in the literature (1–9)
(Table II); these included five
males and five females at a gender ratio of 1:1. The average ages
of the male and female cases are 64.8 and 68.6 years respectively,
with a range of 52–80 years. Five tumors (50%) occurred in the
right abdomen, three in the left abdomen (30%), one in the pelvis
(10%) and one tumor location was unavailable. Three cases presented
with hydronephrosis or hydroureterosis due to tumor compression.
All 10 patients exhibited calcification to varying degrees, which
facilitated diagnosing the disease. The minimum diameter of the
tumors was >5 cm. Nine cases (90%) occurred with surrounding
invasive or distant metastases, and one case was not mentioned.
Eight cases (80%) were treated with surgery combined with
chemotherapy, including one case with interventional therapy, and
the treatments of two cases were unavailable. None of these
treatment options improved the survival rate.
 | Table IIReported cases of retroperitoneal
ESOS. |
Table II
Reported cases of retroperitoneal
ESOS.
| Case no. | Gender/age,
years | Location | Symptoms of tumor
compression | Tumor
calcification | Tumor size, cm | Surrounding
invasion | Therapy | Reference no. |
|---|
| 1 | Female/66 | Right iliac
fossa | Bilateral
hydronephrosis | Calcification | NA | Invasion | Chemotherapy | (1) |
| 2 | Female/67 | Inferior left
renal | Left Ureter
Obstruction | Calcification | 17 | Invasion | Surgery | (2) |
| 3 | Female/74 | Above left renal | Null | Calcification | 16 | Invasion | Interventional
therapy and chemotherapy | (3) |
| 4 | Female/74 | Right renal
region | Null | Calcification | NA | Invasion | N/A | (4) |
| 5 | Male/80 | Peripheral right
renal | N/A | Calcification | 10 | Invasion | Surgery | (5) |
| 6 | Female/62 | Rright renal
region | Null | Calcification | 14 | Invasion | Surgery | (6) |
| 7 | Male/58 | Anterior left
renal | Null | Calcification | 6.5 | Invasion | Chemotherapy | (7) |
| 8 | Male/68 | Inferior right
renal | N/A | Calcification | 19 | NA | N/A | (8) |
| 9 | Male/66 | NA | N/A | Calcification | NA | Invasion | Surgery | (9) |
| 10 | Male/52 | Inferior right
renal | Right kidney
hydronephrosis | Calcification | 6 | Invasion | Surgery and
chemotherapy | Present case |
A total of 93% of cases of retroperitoneal ESOS
showed increasing soft-tissue masses with insidious onset, and
65–80% of patients experienced pain (2). The onset of retroperitoneal ESOS is
commonly asymptomatic due to the large lacuna volume of the
retroperitoneum, which provides sufficient space for tumor growth.
In the present case, once the disease had progressed to a certain
stage, the patient experienced discomfort in the abdomen from the
tumor oppression to the surrounding tissue. In this case, the
patient was not hospitalized until there was discomfort to the
urinary system, caused by the tumor oppression to the right ureter.
Retroperitoneal ESOS is peculiarly prone to recurrence and
metastasis, as the tumor often invades the surrounding vital
organs, making it difficult to completely excise the mass. There is
no specific tumor marker for the auxiliary diagnosis of ESOS.
However, Narayanan (15) found that
in ESOS, the ALP level was often increased, which was established
as a prognostic factor. The serum ALP level of this patient was
normal at the onset of the ESOS, but rose gradually with the
progression of the disease.
Retroperitoneal ESOS is usually discovered by
imaging, which identifies a homogeneous soft-tissue mass with
calcification. A calcified retroperitoneal mass may have a wide
variety of differential diagnoses, which include several benign and
malignant conditions (1,16–20).
Malignant lesions include malignant fibrous histiocytomas,
malignant stromal tumors and extraskeletal chondrosarcomas, and the
differential diagnoses for these are commonly based on
histopathology. In the present case, the histopathology of the
primary retroperitoneal tumor, omentum and gastric metastases all
revealed that the patient was suffering from a retroperitoneal
ESOS, however, the data from the histological assessment showed
large variation. Therefore, the diagnosis of ESOS should be based
on a combination of clinical, radiographical and pathological
findings (10). X-ray of the ESOS
showed a soft-tissue mass with or without calcification, while CT
characteristic imaging revealed a calcified, high-density mass.
Magnetic resonance imaging of the calcification and bone tumors of
ESOS is not as informative as CT, but it is superior to CT in
identifying the tissue components and determining the association
between the tumor boundaries and the surrounding tissue (21). Enhanced CT manifestations of ESOS
can be diversiform (13),
hypervascular or poorly vascular. As ESOS exhibits a variety of
histological manifestations, CT-guided biopsy is recommended only
when lymphoma or germ cell tumors are suspected (22). The diagnoses of the majority of
patients are therefore confirmed based on the pathological findings
during or following surgery.
The comprehensive treatment of ESOS is based on
surgical intervention, and the effects of chemotherapy and
radiotherapy are poor. There has been one previous study (3) on an interventional surgery for ESOS,
however, the effects require further evaluation. The main treatment
for retroperitoneal ESOS is surgery, but caution is recommended
since the volume of the tumor may be too large to be removed
completely. It has been reported that improved survival can be
observed following radical resection and wide excision at the time
of the first surgery (4,23). Lee et al (24) identified that more aggressive
surgical treatment for recurrence was useful for local control, but
did not decrease the incidence of mortality due to the disease.
Therefore the advantages and disadvantages of pre-operative and
intraoperative should be evaluated. Premature surgery will increase
the rate of the transfer, which could be otherwise avoided. As in
the present case, the possibility of malignancy should be taken
into account in retroperitoneal tumors due to the attachment to the
surrounding tissue. A more appropriate surgical approach could be
applied, such as a kidney ventriculostomy instead of cytoreductive
surgery, to relieve hydronephrosis. In the present case, the
surgery could not remove the tumor completely or prolong the life
of the patient. This may have also increased the possibility of
metastasis. When the patient underwent the second surgery, there
was no medical value in resecting the primary tumor, therefore,
only the omental lesions were removed. The patient was administered
chemotherapy, but the effects were unsatisfactory. Five months
after the second surgery, the patients experienced continual
vomiting and underwent a third exploratory laparotomy due to an
incomplete intestinal obstruction. The surgeries included a
gastrojejunostomy and ileocolonic anastomosis, and cytoreductive
surgery was not performed. It is important to consider
retroperitoneal ESOS in the differential diagnosis of a
retroperitoneal mass in order to guide the management of surgery
and determine the most effective treatment for the disease.
The five-year survival rate for patients with ESOS
is <37% (4,25). The volume of the tumor is an important factor
in the prognosis of ESOS, a volume >5 cm is usually associated
with a poor prognosis (10). In the
present case, complete removal of the retroperitoneal tumor was
difficult, as the volume was too large, therefore, the prognosis
was extremely poor. The most common metastases of ESOS occur in the
lung and liver (1,7–10).
However, in the present case, a gastric wall implantation
metastasis was identified, which has rarely been reported in the
literature.
Abbreviations:
|
ESOS
|
extraskeletal osteosarcoma
|
|
ALP
|
alkaline phosphatase
|
|
CD
|
cluster of differentiation
|
|
CT
|
computed tomography
|
References
|
1
|
Uccello M, Malaguarnera M, Giordano M, et
al: A large calcified retroperitoneal extraskeletal osteosarcoma
with consequent bilateral hydronephrosis. Eur Rev Med Pharmacol
Sci. 16:977–982. 2012.
|
|
2
|
Higgins JA, Slam K, Agko M, et al:
Retroperitoneal extraskeletal osteosarcomas. Am Surg. 76:1440–1442.
2010.
|
|
3
|
Zhang HJ, Yang JJ, Lu JP, et al:
Retroperitoneal extraskeletal osteosarcoma: imaging findings and
transarterial chemoembolization. Cardiovasc Intervent Radiol.
33:430–434. 2010.
|
|
4
|
Sordillo PP, Hajdu SI, Magill GB, et al:
Extraosseous osteogenic sarcoma: A review of 48 patients. Cancer.
51:727–734. 1983.
|
|
5
|
Soh BH, Han WK, Lee SH, et al:
Retroperitoneal extraskeletal osteosarcoma misconstrued as a
primary renal tumor. Korean J Urol. 47:1124–1126. 2006.
|
|
6
|
Arai H, Rino Y, Nishii T, et al:
Well-differentiated extraskeletal osteosarcoma arising from the
retroperitoneum that recurred as anaplastic spindle cell sarcoma.
Case Rep Med. 2010:3275912010.
|
|
7
|
Hamdan A, Toman J, Taylor S, et al:
Nuclear imaging of an extraskeletal retroperitoneal osteosarcoma:
respective contribution of 18FDG-PET and (99 m) Tc oxidronate
(2005:1b). Eur Radiol. 15:840–844. 2005.
|
|
8
|
van Rijswijk CS, Lieng JG, Kroon HM, et
al: Retroperitoneal extraskeletal osteosarcoma. J Clin Pathol.
54:77–78. 2001.
|
|
9
|
Maredia R, Ward DL, Moreno AJ, et al:
Extensive extraskeletal osteosarcoma in the liver and abdomen as
demonstrated by bone scintigraphy. Clin Nucl Med. 22:717–718.
1997.
|
|
10
|
Bane BL, Evans HL, Ro JY, et al:
Extraskeletal osteosarcoma. A clinicopathologic review of 26 cases.
Cancer. 65:2762–2770. 1990.
|
|
11
|
Chung EB and Enzinger FM: Extraskeletal
osteosarcoma. Cancer. 60:1132–1142. 1987.
|
|
12
|
Allan CJ and Soule EH: Osteogenic sarcoma
of the somatic soft tissues. Clinicopathologic study of 26 cases
and review of literature. Cancer. 27:1121–1133. 1971.
|
|
13
|
Wesseling FJ, Tjon A, Tham RT, Breed W, et
al: Retroperitoneal extraskeletal osteosarcoma. AJR Am J
Roentgenol. 155:1139–1140. 1990.
|
|
14
|
Tao SX, Tian GQ, Ge MH, et al: Primary
extraskeletal osteosarcoma of omentum majus. World J Surg Oncol.
19:252011.
|
|
15
|
Narayanan S: Alkaline phosphatase as tumor
marker. Ann Clin Lab Sci. 13:133–136. 1983.
|
|
16
|
Nishimura H, Zhang Y, Ohkuma K, et al: MR
imaging of soft-tissue masses of the extraperitoneal spaces.
Radiographics. 21:1141–1154. 2001.
|
|
17
|
Kransdorf MJ: Benign soft-tissue tumors in
a large referral population: distribution of specific diagnoses by
age, sex, and location. AJR Am J Roentgenol. 164:395–402. 1995.
|
|
18
|
Kransdorf MJ: Malignant soft-tissue tumors
in a large referral population: distribution of specific diagnoses
by age, sex, and location. AJR Am J Roentgenol. 164:129–134.
1995.
|
|
19
|
Nishino M, Hayakawa K, Minami M, et al:
Primary retroperitoneal neoplasms: CT and MR imaging findings with
anatomic and pathologic diagnostic clues. Radiographics. 23:45–57.
2003.
|
|
20
|
Khong PL, Lam KY, Ooi CG, et al: Mature
teratomas of the adrenal gland: imaging features. Abdom Imaging.
27:347–350. 2002.
|
|
21
|
Davidson AJ, Hartman DS and Goldman SM:
Mature teratoma of the retroperitoneum: radiologic, pathologic, and
clinical correlation. Radiology. 172:421–425. 1989.
|
|
22
|
Secil M, Mungan U, Yorukoglu K, et al:
Case 89: Retroperitoneal extraskeletal osteosarcoma. Radiology.
237:880–883. 2005.
|
|
23
|
Rao U, Cheng A and Didolkar MS:
Extraosseous osteogenic sarcoma: clinicopathological study of eight
cases and review of literature. Cancer. 41:1488–1496. 1978.
|
|
24
|
Lee JS, Fetsch JF, Wasdhal DA, et al: A
review of 40 patients with extraskeletal osteosarcoma. Cancer.
76:2253–2259. 1995.
|