Introduction
Pancreatic carcinoid tumors are rare malignancies.
Modlin et al (1) reported
that pancreatic carcinoid tumors account for 0.55% of all carcinoid
tumors. However, there is no globally accepted method for the
diagnosis and treatment of pancreatic cancer. In the present study,
the clinical data of 13 hospitalized patients is reviewed, and the
diagnostic and therapeutic methods are discussed.
Materials and methods
Between January 1954 and May 2010, 13 patients with
pancreatic carcinoid tumors were treated in Tianjin Medical
University Cancer Institute and Hospital (Tianjin, China). The
clinical data of these patients were collected and analyzed.
Hematoxylin-eosin and immunohistochemistry (IHC) staining of the 13
patient tissues were performed. The expression of neuron-specific
enolase (NSE), cytokeratin (CK), chromogranin A (CgA) and
synaptophysin (Syn) were observed by IHC staining. In these
experiments, 10% of cancer cells were stained brown. Staining
intensity was scored according to the percentage of positively
stained cells as follows: −, <5%: +, ≥5 but <25%; ++, 25–50%;
and +++, >50%. The clinical data of the patients was collected
by telephone or during outpatient service follow-up during the
post-operative period until August 2011. Consent was obtained from
the patient’s families.
Statistical analysis
The patient survival curve was generated by
Kaplan-Meier analysis. SPSS 13.0 was used for the statistical
analysis of the data (SPSS, Inc., Chicago, IL, USA).
Results
Patient characteristics
Between 1954 and 2010, 414 cases of carcinoid tumors
were admitted to Tianjin Medical University Cancer Institute and
Hospital and 13 patients (3.14%, 13/414), 5 male and 8 female, were
diagnosed with pancreatic carcinoid tumors. The mean age was 50
years (range, 39–64 years). Details of the patient information are
presented in Table I.
 | Table IClinical characteristics and prognosis
of patients. |
Table I
Clinical characteristics and prognosis
of patients.
| Patient no. | Year admitted | Age, years | Gender | Symptoms | Tumor marker | Location and size,
cm | Surgery | Treatment | Specific
staining | Survival, months |
|---|
| 1 | 2012 | 64 | Male | Upper abdominal
pain | Negative | Head: 6×8×4 and
homotype clumping in portal vein | PD | None | NSE+,
CK−, CgA−, Syn−
NSE+, CK−, CgA−,
Syn− | 49 |
| 2 | 2002 | 47 | Male | Jaundice | Negative | Head: 8×10 |
Choledochojejunostomy | None | | 25 |
| 3 | 2000 | 46 | Female | Osphyalgia | Negative | Body and tail:
4.5×4.5 | Splenectomy and
DP | None | NSE+,
CK−, CgA−, Syn+ | 44+ |
| 4 | 2009 | 46 | Male | Tumor detected upon
physical examination | Ferritin, 240.8
μg/l | Head: 5 | PD and
lymphadenectomy | None | NSE−,
CK−, CgA−, Syn+ | 42+ |
| 5 | 2008 | 44 | Male | Nausea, backache and
loss of weight | Negative | Head: 1 | Local excision | Cisplatin plus
docetaxel and biotherapy | NSE++,
CK+, CgA+, Syn+ | 23+ |
| 6 | 2009 | 39 | Male | Upper abdominal
pain | Negative | Head: 6.7×5.2 and
bolt in superior mesenteric venous | PD and thrombectomy
from superior mesenteric venous | 0.9 mg/day octreotide
and directional radiation | NSE+,
CK+, CgA+, Syn+ | 20+ |
| 7 | 2009 | 53 | Male | Tumor detected upon
physical examination | CEA, 5.25 μg/l | Tail: 8.5×7.9 | Splenectomy and
DP | None | NSE−,
CK+, CgA−, Syn+ | 31+ |
| 8 | 2008 | 41 | Female | Full distention and
accentuation after taking food | Negative | Head: 6.8×5.2 | Total
pancreatectomy | Octreotide | NSE+++,
CK++, CgA−, Syn+ | 25 |
| 9 | 2009 | 64 | Female | Upper abdominal
pain | Negative | Body and tail:
7×5 | Splenectomy and
DP | None | NSE−,
CK+, CgA++, Syn+ | 21+ |
| 10 | 2010 | 47 | Male | Headache | Negative | Tail: 6.2×7.8 | Splenectomy and
DP | Octreotide | NSE−,
CK+, CgA−, Syn++ | 32 |
| 11 | 2009 | 62 | Male | Diarrhea | Negative | Head: 6.5×7.0 and
liver metastasis | PD | None | NSE−,
CK+, CgA−, Syn+ | 26 |
| 12 | 2011 | 60 | Male | Upper abdominal
pain | Negative | Body and tail:
10×10 | Splenectomy and
DP | Octreotide
acetate | NSE+,
CK+, CgA+, Syn+ | 3 |
| 13 | 2005 | 42 | Male | Upper abdominal
pain and loss of weight | Negative | Head: 10 and
invasion of SMV, distal common bile duct, duodenum |
Choledochojejunostomy and
gastrojejunostomy | Cisplatin plus
docetaxel | NSE++,
CK+, CgA+, Syn− | 5+ |
Clinical presentation
Emaciation and jaundice were observed in one case,
and one patient had headache symptoms. In addition, three patients
presented with pain in the back. Epigastric pain was exhibited by
five cases, from which, two patients presented with emaciation and
nausea simultaneously; the remaining three patients were diagnosed
with pancreatic carcinoid tumors during physical examination. None
of the patients exhibited signs of carcinoid syndrome.
Laboratory examinations
One case presented with a slight increase in
carcinoembryonic antigen (CEA; 5.25 μg/l; normal range, 0–5 μg/l)
and another case exhibited characteristics of an elevated level of
ferritin (240.8 μg/l; normal range, 13–150 μg/l). None of the
patients had abnormal levels of gastrointestinal tumor markers
[carbohydrate antigen (CA)199, CEA and CA724], and an increased
5-Serotonin (5-HT) content in the serum and an elevated
5-hydroxyindoleacetic acid (5-HIAA) level in the urine were not
detected prior to the pathological diagnosis.
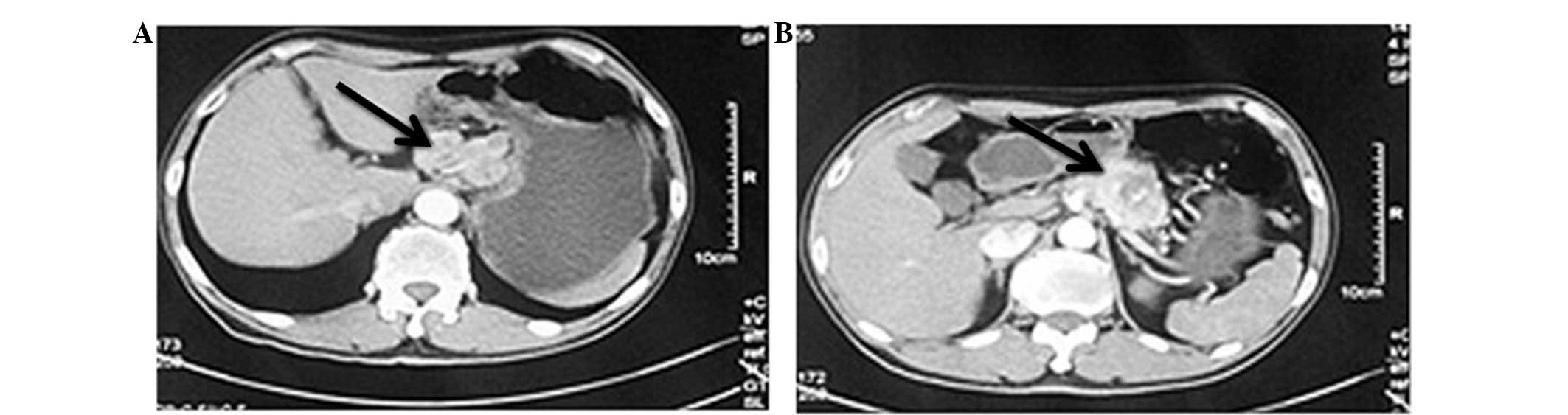
Tumor size, location, and metastasis
Pancreatic carcinoid tumors were detected in two
cases during the physical examination, without any symptoms, and
the remaining patients exhibited large-sized tumors, with a mean
diameter of 7.1 cm, as shown in Fig.
1. Tumors were found on the head of the pancreas in eight cases
and on the body and tail in the remaining five cases. Two patients
presented with hepatic metastasis, one with celiac metastasis and
one with spleen metastasis. A portal tumor thrombus was observed in
two patients.
Imaging features
Using B-mode ultrasonic detection, it was found that
the solid tumors had hypoechoic, irregular margins, non-uniform
echo in the tumor, no significant blood flow and no dilated
pancreatic ducts. The initial diagnostic report of the computed
tomography (CT) and magnetic resonance imaging scanning images
provided evidences for pancreatic neuroendocrine or islet-cell
tumors. The majority of the CT images showed heterogeneous
enhancement of the arterial phase as a characteristic of the
neuroendocrine tumor, which could be differentiated into pancreatic
ductal adenocarcinoma.
Therapy methods
In total, 10 cases were treated with radical
resection. Pancreatoduodenectomy was performed on 4 patients, 5
patients were treated with distal pancreatectomy, and local
resection was performed on the remaining patient for the small
tumor (1 cm3). For the two patients with portal tumor
thrombi, as described previously, a pancreatoduodenectomy was
performed, and the embolus was removed at the same time. However,
radical surgery could not be performed on two patients due to the
remote metastasis and they were therefore treated with
cholangiojejunostomy and gastrojejunostomy/choledochojejunostomy,
respectively. Biopsy and administration of somatostatin were
performed simultaneously. Four patients received somatostatin at a
dosage of 0.9 mg/day, the durations varied between patients.
Pathology characteristics
The tumor samples were ashen and tough. In the IHC
staining, the expression of CK, Syn, CgA and NSE was positive in
nine (69.23%), 10 (76.92%), five (38.46%) and eight (61.54%) cases,
respectively (Fig. 2).
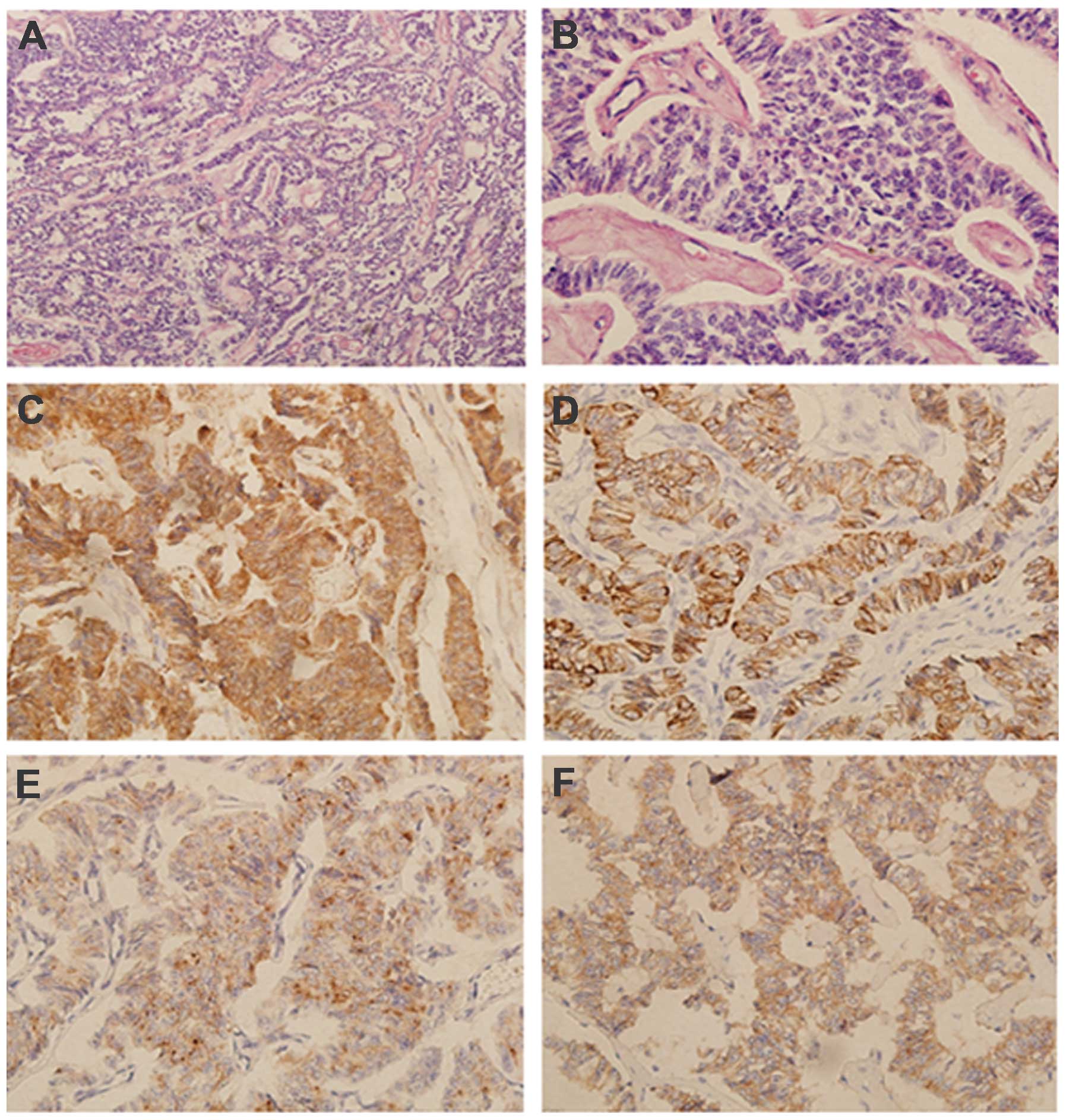 | Figure 2Hematoxylin and eosin (HE) and
specific immunohistochemical staining for NSE, Syn, CgA and CK in
samples from patient no. 3, a 46-year-old female, with a one-month
history of backache. (A) HE, ×100 magnification; (B) HE, ×400
magnification; (C) NSE+++, ×200 magnification; (D)
CK++, ×200 magnification; (E) CgA+, ×200
magnification; and (F) Syn+, ×200 magnification. Tumor
cells with identical shape, regular arrangement and abundant
cytoplasm were observed. Fine particles, and small and round nuclei
were found in the middle of the cells by eosin staining. Chromatin
was fine and uniform. Nuclear fission was often apparent. NSE, CK,
CgA and Syn particles were located in the plasma of the tumor
cells, with no expression in the intercellular substance. Computed
tomography indicated that the mass was 4.5 cm3 and
located on the tail of the pancreas. A distal pancreatectomy was
performed. This patient was followed up until August 2011, with no
signs of metastasis for 21 months. NSE, neuron-specific enolase;
CK, cytokeratin; CgA, chromogranin A; Syn, synaptophysin. |
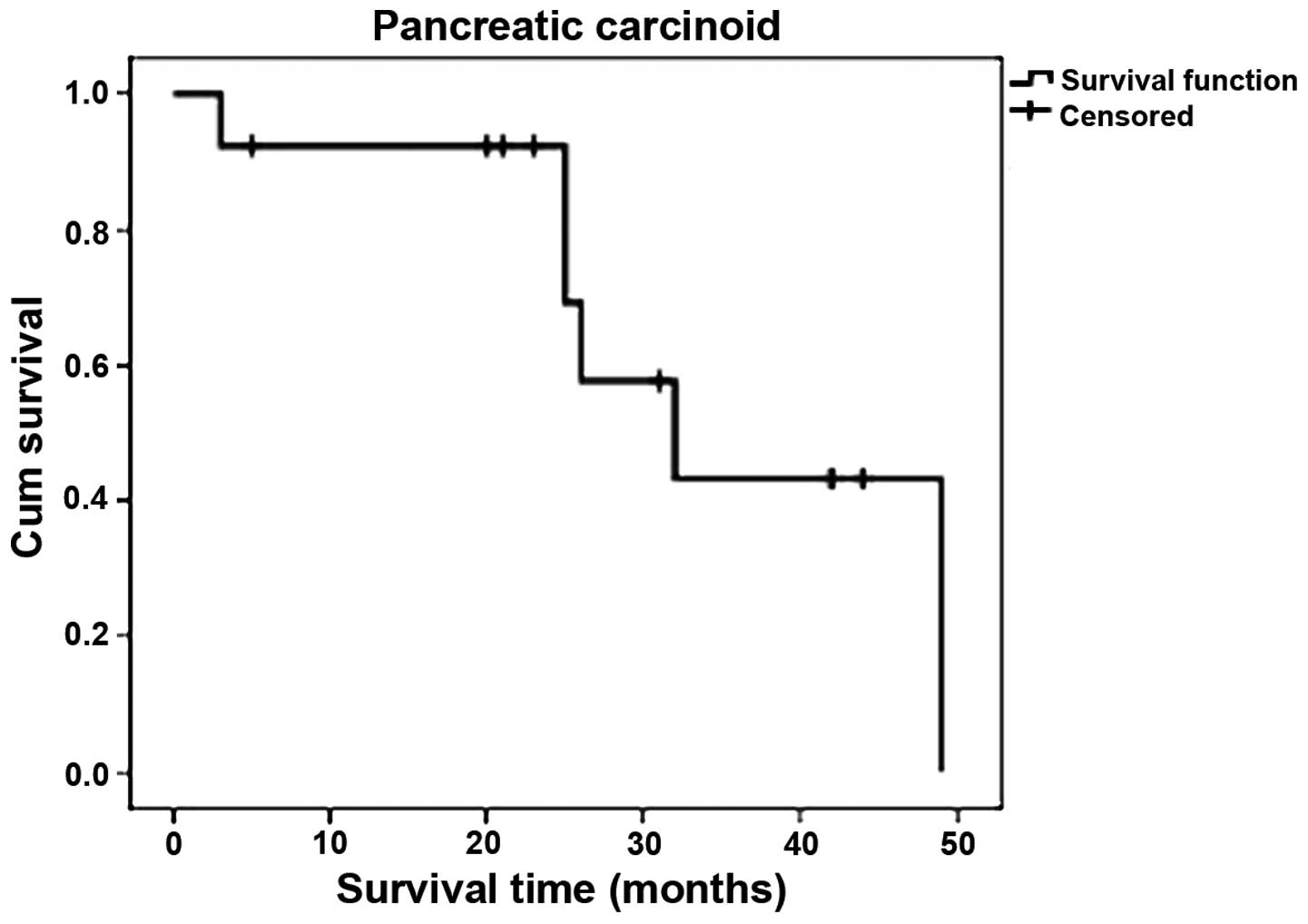
Median survival
The survival time of the 13 cases was calculated,
and the median survival time was 26.6 months. Seven patients had
been followed up until August 2011 (Fig. 3).
Discussion
Carcinoid tumors are extremely rare malignancies
that are derived from enterochromaffin cells, which come from the
embryonic neural crest and are widely distributed in the digestive
tract. These cells produce a large amount of polyaminoamide
hormones. Carcinoid tumors originate from argentaffin cells,
accounting for 0.05–0.2% of the total number of malignancies.
Carcinoid tumors have the characteristics of
inhomogeneous organ distribution and mostly occur in the
gastrointestinal tract; among which the appendix, small intestine
and colorectum accounts for 50, 20–30 and 15%, respectively
(2,3). In Tianjin Medical University Cancer
Institute and Hospital, 414 patients with carcinoid tumors were
treated between 1954 and May 2010, of which, 13 cases (3.14%) were
pancreatic carcinoid tumors.
The occurrence of carcinoid tumors is associated
with living habits, including smoking and drinking, as well as with
family history, diabetes and gender (4). The tumors occur more in female than in
male (5). However, in this study,
there was equal incidence between female and male. Typical
carcinoid syndrome presents with symptoms such as skin flushes,
diarrhea, stomachaches, asthma, right-sided valvulopathy lesions
and hepatomegaly. Laboratory examination show increased 5-HT
content in the serum and elevated amounts of 5-HIAA in the urine.
Generally, carcinoid tumors located in mid-gut secrete higher
levels of 5-TH, which easily induces carcinoid syndrome. Pancreatic
carcinoid tumors derived from the foregut are not typical of the
syndrome. In addition, it has been reported that normal
gastrointestinal tumor markers are not detected in carcinoid tumors
(6). This is consistent with the
present study results. Radiographic results show no specific
characteristics, but heterogeneous enhancement of the arterial
phase can be found on CT as a characteristic of neuroendocrine
tumors. The tumors can be differentiated from pancreatic ductal
adenocarcinomas. Therefore, there is cause to reject the
possibility of pancreatic ductal adenocarcinoma (7). As a result, it is difficult to
diagnose pancreatic carcinoid tumors prior to surgery or
biopsy.
At present, the diagnosis of a pancreatic carcinoid
tumor depends mainly on the pathological examination. The mucosal
surface appears mostly intact and the incisal surface appeared as
yellow or gray (8). Occasionally,
the surface of the tumors appeared ulcerated or with hemorrhage.
This appearance is similar to that of an adenocarcinoma. The tumor
usually invades into the muscular layer and serosa (9). Numerous patients develop polyphyletic
carcinoid tumors. Pancreatic carcinoid tumors have similar
characteristics. Typically, the cancer cells appear to be
consistent in terms of morphology, i.e., they have a regular
arrangement, abundant cytoplasm and a small oval nucleus located in
the center. Thin and uniform chromatin, and bare karyokinesis are
also their common characteristics. However, the atypical
characteristics of the cells can include a polygonal or spindle
shape, marked nuclear atypia, extensive chromatin and marked
karyokinesis. NSE, CK, CgA and Syn can be detected by
immunohistochemical staining (10)
and this method can be used as an adjunct to confirm the presence
of a carcinoid tumor.
Surgical resection is potentially a curative therapy
for carcinoid tumors. The choice of surgical methods depends on
tumor size, position, infiltration and lymph node metastasis, with
tumor size and infiltration being the major contributing factors
(11). However, owing to the unique
position of the pancreas and the lack of typical clinical
characteristics, 66–81% patients present with a large tumor size
and a number with distant metastasis (12). Therefore, radical surgery cannot be
performed.
Moreover, there is disagreement over the
administration of somatostatin analogs to medically inoperable
patients. A previous study revealed that carcinoid cells express a
large number of somatostatin receptors, therefore, somatostatin
analogs could be used as first-line therapy drugs for patients
(13). Contrary to this, there is
no evidence to confirm that somatostatin can prolong median
survival time following surgery or palliative treatment. At
present, surgery is the only effective treatment for carcinoid
tumors due to the uncertainty on the availability of chemotherapy.
Reoperation can improve the prognosis following tumor recurrence or
metastasis. Therefore, an early diagnosis and surgical resection
are considered as the most effective treatments for pancreatic
carcinoid tumors (14,15).
Pancreatic carcinoid tumors are considered to be a
low-grade malignancy that grows slowly, similar to other carcinoid
tumors. The condition has a good prognosis compared to pancreatic
ductal adenocarcinoma, but a worse prognosis compared with that
carcinoid tumors of other organs. Previous studies have shown that
the five-year survival rate of patients with pancreatic carcinoid
tumors may be increased to ~35% (16,17).
Patients who undergo radical surgery eventually succumb due to
hepatic or intra-abdominal metastasis. In the present study,
metastasis was found in three cases at the time of the primary
diagnosis; these patients succumbed after 26, 32 and 49 months,
respectively. Seven patients remained alive at the time of the
latest follow-up in August 2011.
This present study has certain limitations. Bias may
have been introduced as the follow-up was not short and due to the
relatively small number of patients included in the study. A larger
study group is required to confirm these findings. The follow-up of
the remaining patients will be continued.
In conclusion, pancreatic carcinoid has no typical
syndrome and only the pathological results are able to confirm the
diagnosis. Chemotherapy may not have a significant effect on the
treatment of pancreatic carcinoid tumors, while surgery is the most
effective treatment. Surgery for the reduction of the primary tumor
and metastasis result in a appreciable improvement in the survival
time and quality of life.
Acknowledgements
This study was supported by grants from the National
Natural Science Foundation of China (no. 81341068), the Natural
Science Foundation of Tianjin Health Bureau (no. 2013KZ089), the
Doctor Foundation of Tianjin Cancer Institute and Hospital (no.
B24) and the Youth Program of Tianjin Nature Science Foundation
(no. 13JCQNJC10700).
References
|
1
|
Modlin IM, Shapiro MD and Kidd M: An
analysis of rare carcinoid tumors: clarifying these clinical
conundrums. World J Surg. 29:92–101. 2005. View Article : Google Scholar
|
|
2
|
No authors listed. Plastic insulin
syringes. Br Med J (Clin Res Ed). 296:11951988. View Article : Google Scholar
|
|
3
|
Tamm EP, Kim EE and Ng CS: Imaging of
neuroendocrine tumors. Hematol Oncol Clin North Am. 21:409–432.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Soga J: Carcinoids and their variant
endocrinomas. An analysis of 11842 reported cases. J Exp Clin
Cancer Res. 22:517–530. 2003.
|
|
5
|
Hassan MM, Phan A, Li D, Dagohoy CG, Leary
C and Yao JC: Risk factors associated with neuroendocrine tumors: A
U.S.-based case-control study. Int J Cancer. 123:867–873. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Capurso G, Falconi M, Panzuto F,
Rinzivillo M, Boninsegna L, Bettini R, Corleto V, Borgia P,
Pederzoli P, Scarpa A and Delle Fave G: Risk factors for sporadic
pancreatic endocrine tumors: a case-control study of prospectively
evaluated patients. Am J Gastroenterol. 104:3034–3041. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Chu P, Wu E and Weiss LM: Cytokeratin 7
and cytokeratin 20 expression in epithelial neoplasms: a survey of
435 cases. Mod Pathol. 13:962–972. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Varas-Lorenzo MJ: Long-standing malignant
pancreatic carcinoid treated with octreotide. Rev Esp Enferm Dig.
102:662–666. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Torske KR and Thompson LD: Adenoma versus
carcinoid tumor of the middle ear: a study of 48 cases and review
of the literature. Mod Pathol. 15:543–555. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cernaianu G, Tannapfel A, Nounla J,
Gonzalez-Vasquez R, Wiesel T and Tröbs RB: Appendiceal carcinoid
tumor with lymph node metastasis in a child: case report and review
of the literature. J Pediatr Surg. 45:e1–e5. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
He XW, Wu XJ, He XS, Zou YF, Ke J, Wang JP
and Lan P: Clinicopathologic analysis of eight cases of pancreatic
carcinoid tumors. Chin Med J (Engl). 122:1591–1594. 2009.
|
|
12
|
Zuetenhorst JM and Taal BG: Metastatic
carcinoid tumors: a clinical review. Oncologist. 10:123–131. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kaltsas GA, Besser GM and Grossman AB: The
diagnosis and medical management of advanced neuroendocrine tumors.
Endocr Rev. 25:458–511. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Chowsanitphon J: Carcinoid tumor. Oncol
Nurs Forum. 37:677–679. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Bajetta E, Ferrari L, Martinetti A, Celio
L, Procopio G, Artale S, Zilembo N, Di Bartolomeo M, Seregni E and
Bombardieri E: Chromogranin A, neuron specific enolase,
carcinoembryonic antigen, and hydroxyindole acetic acid evaluation
in patients with neuroendocrine tumors. Cancer. 86:858–865. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Pavel M, Kidd M and Modlin I: Systemic
therapeutic options for carcinoid. Semin Oncol. 40:84–99. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Zarina AL, Hamidah A, Zulkifli SZ,
Zulfiqar MA and Jamal R: Malignant pancreatic carcinoid tumour.
Singapore Med J. 48:e320–e322. 2007.PubMed/NCBI
|