Introduction
Multiple primary malignant neoplasms (MPMNs) may
occur in a single organ or involve multiple organ systems and can
be synchronous or metachronous. The current criteria for the
diagnosis of MPMNs, which were established by Warren and Gates
(1), are as follows: i) Each of the
lesions must be malignant; ii) each of the lesions must exhibit
distinctively different pathology; iii) and metastases from the
prior malignancies must be excluded. Among patients with multiple
primary malignancies, double cancers are commonly observed, triple
cancers occur in 0.5% of these patients, and quadruple or quintuple
cancers occur in <0.1% (2). The
present study reports a rare case of a patient exhibiting eight
MPMNs. Written informed consent was obtained from the patient.
Case report
Personal and family history
The present study describes the case of a
61-year-old female who attended the Third Affiliated Hospital of
Suzhou University (Changzhou, China). The patient denied tobacco
use or alcohol consumption when they first came to our hospital in
1979; however, the patient had been diagnosed with type two
diabetes mellitus ~20 years ago and injects insulin to control
blood glucose levels. One year prior to presentation, the patient’s
older brother was diagnosed with brain glioma and two years prior;
the patient’s nephew was diagnosed seminoma of the testis. In
addition, the patient had a healthy 33-year-old daughter.
Medical history
First tumor
The first tumor identified was colon cancer, the
initial symptoms of which were abdominal distension and diarrhoea.
The patient visited our hospital and received a gastrointestinal
barium meal and colonoscopy examination. The tumor was curatively
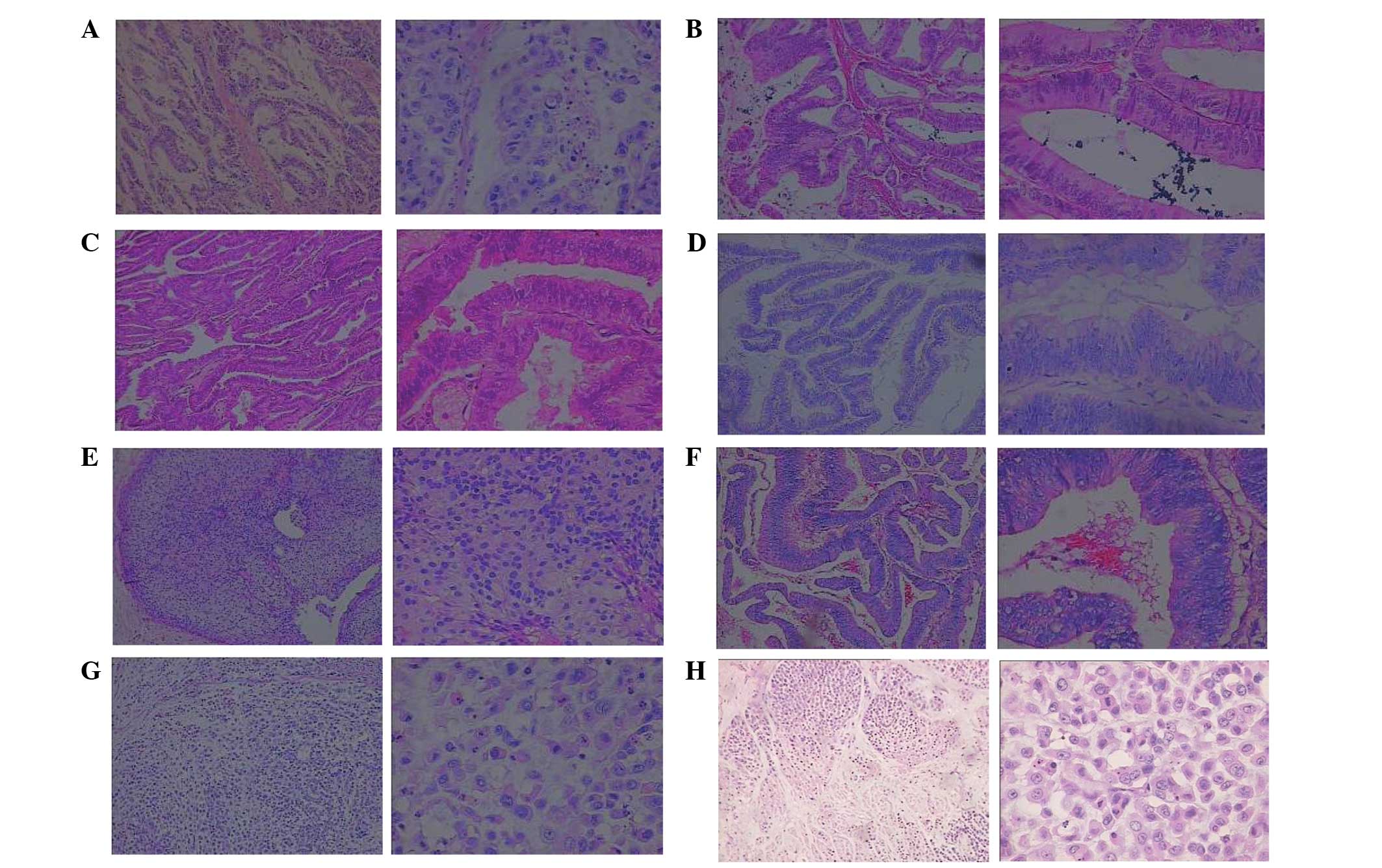
resected in September 1979. Subsequent histopathological analysis
identified a grade III (poorly differentiated) Dukes’ B2
adenocarcinoma of the ileocecal junction (Fig. 1A) (3), which, according to the tumor, node,
metastasis (TNM) system was classified as T3N0M0, stage II
(4). Following surgery, the patient
underwent five cycles of chemotherapy with 5-fluorouracil [5-FU;
500 mg/m2 by intravenous (i.v.) infusion from day 1 to 5
every 21 days as a cycle], dactinomycin (8 μg/kg by i.v. infusion
from day 1 to 5 every 21 days as a cycle) and thiotepa (0.2 mg/kg
by i.v. infusion from day 1 to 5 every 21 days as a cycle).
Second tumor
In October 1988, an additional colon cancer was
identified in the splenic flexure of the colon by routine
endoscopic follow-up (Fig. 1B). The
patient underwent curative surgery followed by five cycles of
adjuvant chemotherapy with 5-FU (500 mg/m2 by i.v.
infusion from day 1 to 5 every 21 days as a cycle), mitomycin (10
mg by i.v. infusion at day 1 every 21 days as a cycle) and
vincristine (2 mg by i.v. infusion at day 1 every 21 days as a
cycle).
Third tumor
In May 1996, the patient was diagnosed with cancer
of the endometrium that had presented as vaginal hemorrhage. A
hysterectomy was performed and pathological examination identified
a well-differentiated, estrogen receptor (ER)- and progesterone
receptor (PR)-positive adenocarcinoma of the endometrium (Fig. 1C).
Fourth tumor
In May 1998, an additional 2-cm-diameter tumor was
identified in the descending colon by a routine colonoscopy, and
the patient underwent descending colectomy. Subsequent pathological
examination determined that the tumor was a descending colon polyp,
which resembled an adenoma. Certain parts of the glandular
epithelium demonstrated midrange atypical hyperplasia and malignant
cells encroaching into the superficial muscular layer (Fig. 1D). The tumor was classified as
T1N0M0, stage I.
Fifth tumor
In April 2004, a palpable mass was identified in the
right breast and the patient was referred to the Department of
Breast Surgery, the Third Affiliated Hospital of Suzhou University.
Biopsy analysis indicated malignancy and the patient underwent a
modified radical mastectomy with level II lymph node dissection.
Pathological examination of the 1.0×1.0×0.8-cm resected mass
identified canal papillary carcinoma with a clear resection margin
(Fig. 1E). Additionally, the lymph
nodes were negative for cancer; immunohistochemistry demonstrated
that the patient was hadro-positive (+++) for ER, PR and p53, and
negative for human epidermal growth factor receptor 2; and the
tumor was classified as T1N0M0, stage I. This was the patient’s
fifth malignancy. Following surgery, the patient received two
cycles of chemotherapy with 5-FU (500 mg/m2 by i.v.
infusion from day 1 to 5 every 21 days as a cycle), methotrexate (1
g/m2 by i.v. infusion at day 1 every 21 days as a cycle)
and cyclophosphamide (600 mg/m2 by i.v. infusion at day
1 every 21 days as a cycle).
Sixth tumor
In May 2007 it was noted that the patient’s
carcinoembryonic antigen (CEA) concentration was progressively
increasing. The patient attended the hospital and received computed
tomography (CT) and colonoscopy examinations. A 6-cm-diameter tumor
was identified in the colon and palliative colectomy was performed.
Subsequent pathological examination demonstrated a mushroom-like
adenocarcinoma of the colon, the majority of which was mucinous
adenocarcinoma (Fig. 1F) that
encroached on the total depth of the intestinal wall.
Immunohistochemistry was p53- and proliferating cell nuclear
antigen-negative and nm23 -, cox-2- and epidermal growth factor
receptor-positive. Following surgery, the patient underwent 12
cycles of chemotherapy with folinic acid (leucovorin), 5-FU and
oxaliplatin. One cycle included i.v. leucovorin calcium at a dose
of 200 mg/m2, bolus 5-FU at a dose of 400
mg/m2 and continuous i.v. 5-FU at a dose of 600
mg/m2 on day 1, followed by 85 mg/m2
oxaliplatin on day 2, and was repeated every 2 weeks.
Seventh and eighth tumors
In February 2011, the patient’s CEA concentration
was again noted to be progressively increasing. Thus, two novel
tumors were identified by positron emission tomography-CT and
colonoscopy examination; one in the small intestine and one in the
colon. The patient underwent partial small intestine and colon
resection of a small intestinal tumor measuring 5.0×5.0×4.5 cm and
a colonic tumor measuring 4.5×4.0×4.5 cm, respectively. Subsequent
pathological examination demonstrated that the two tumors were
poorly differentiated mucinous adenocarcinomas; however, the lymph
nodes were negative for cancer (Fig.
1G). Following surgery, the patient received 12 cycles of
chemotherapy with folinic acid, 5-FU and irinotecan. One cycle
included i.v. leucovorin calcium at a dose of 200 mg/m2,
bolus 5-FU at a dose of 400 mg/m2 and continuous i.v.
5-FU at a dose of 600 mg/m2 on day 1, followed by 180
mg/m2 irinotecan on day 2, and was repeated every 2
weeks. The last chemotherapy cycle ended in September 2011, and the
patient remained alive and appeared to be tumor-free at the time of
writing.
Discussion
The current study presents the case of a patient
with eight pathologically verified primary tumors originating in
the colon, endometrium, breast and small intestine, including six
of the digestive system. According to Kapsinow’s definitions
(5), the first six tumors were
metachronous carcinomas and the most recent two tumors were
synchronous carcinomas. Cases of multiple primary malignancies have
been increasingly reported in recent years (6–9),
however, it remains rare to encounter a patient with eight primary
malignancies. As six of the tumors were located in the intestinal
tract, endoscopies were performed on direct relatives of the
patient, including the patient’s daughter, nephew and two brothers;
however, no familial adenomatous polyposis or other hereditary
nonpolyposis colorectal cancer were identified.
Pathologists were recruited to aid in determining
whether the colonic tumors of the present patient were primary or
metastatic. The following are crucial characteristics for
differentiating between the two types of tumor: i) The majority of
MPMNs are located in the wall of the colon and rectum, whereas
metastatic carcinomas generally occur adjacent to the colon and
rectum or in the regional lymph nodes; ii) the majority of newly
diagnosed MPMNs are located in a different region to previous
tumors, whereas relapsing carcinomas commonly occur at the site of
the primary tumor; iii) the majority of newly diagnosed MPMNs are
singular, whereas metastatic carcinomas tend to be multiple; iv)
synchronous multiple primary carcinomas of the colon and rectum may
exhibit similar or different pathology to the primary tumor,
whereas metastatic carcinomas exhibit similar pathology to the
primary tumor (9); and v) the
diagnosis of synchronous MPMNs of the colon and rectum requires
that tumors be separated by >5 cm of normal colonic and rectal
wall (10). In addition, according
to a previous report (11),
synchronous and metachronous primary advanced colorectal carcinomas
in the same patient may exhibit variable KRAS, NRAS and BRAF
genotypes, which have diagnostic and therapeutic implications when
metastases occur, and may facilitate the identification of
simultaneous or metachronous distant metastases.
Although the mechanisms responsible for the
development of MPMNs are yet to be fully elucidated, frequently
implicated factors include genetic susceptibility, immune status
and previous intensive exposure to carcinogens, such as chemo-
and/or radio-therapy used to treat tumors (7,12).
Furthermore, a number of hereditary conditions are associated with
multiple primary malignant neoplasms; for example, Li-Fraumeni
syndrome is a rare disorder that greatly increases the risk of
developing various types of cancer. The types of cancer most often
associated with this syndrome are breast cancer, osteosarcoma and
soft tissue sarcomas, as well as brain tumors, leukemias and
adrenocortical carcinoma (13). In
addition, the CHEK2 and TP53 genes are associated with Li-Fraumeni
syndrome, as >50% of families with this syndrome exhibit
inherited TP53 gene mutations (14). The present study used
immunohistochemistry to identify mutations in the TP53 gene in each
of the current patient’s tumors, however, the results were
consistently negative. Considering the large numbers of primary
tumors the patient developed, it was proposed that an unidentified
mutation may exist and, thus, the patient was at a high risk of
developing additional tumors in the future.
Novel technologies are able to identify various
genetic changes, such as punctiform mutations, loss of
heterozygosity or genetic instability. Furthermore, microsatellite
instability reportedly occurs more frequently and has a worse
prognosis in cases of MPMNs compared with in sporadic cancers
(15). Similar epigenomic and
epigenetic events are frequently observed within a pair of
synchronous cancers, indicating the presence of a field defect; for
example, microsatellite instability in sporadic cancer is typically
due to epigenetic silencing of the MLH1 gene (16).
Various studies have demonstrated that chemo- and
radio-therapy are carcinogenic (17,18).
By affecting the function and synthesis of DNA, a variety of
chemotherapeutic agents, particularly alkylating agents, may cause
damage to dividing cells in healthy tissues, such as bone marrow or
gastrointestinal mucosa cells. The patient described in the present
report received chemotherapy numerous times and this may have
contributed to the development of additional MPMNs.
The literature regarding MPMNs recommends that
secondary primary cancers should be resected as early as possible
and concludes that the probability of successful treatment is
similar to that of a single cancer (19). Furthermore, long-term follow-up and
screening strategies appear to be important for patients who have
undergone curative resection of malignancies. Healthcare workers
should consider that the prevalence of multiple primary
malignancies appears to be increasing and, thus, should be prepared
to differentiate secondary primary cancer from metastatic cancer.
The present patient was cooperative and attended the hospital
frequently; therefore, all of the tumors were diagnosed early and
removed.
Koutsopoulos et al (20) reviewed cases with three or more
primary malignancies. The occurrence of three primary malignancies
in one patient is not common, however, neither is it particularly
rare. Therefore, it is important that patients who have been
treated for cancer are provided with adequate follow-up care. Upon
the appearance of the symptoms and signs of a tumor in a patient
who has previously been treated for a primary cancer, metastasis
should not be assumed as the diagnosis. Instead, the possibility of
a localized and curable secondary primary cancer should be
considered and evaluated, and tumor markers or positron emission
tomography and computed tomography may be useful for follow-up.
Although the present patient developed a large number of tumors
over a >32-year period, the patient is alive and has a good
quality of life. Therefore, multiplicity of primary malignancies
itself does not necessarily indicate a poor prognosis provided that
adequate diagnosis and treatment are provided.
In conclusion, it is important for health-care
workers to consider that the appearance of an additional tumor in a
cancer patient may be either a metastatic or novel lesion, and the
possibility of a metachronous or a synchronous malignancy should be
investigated. Furthermore, prolonged follow-up after surgery should
be considered.
References
|
1
|
Warren S and Gates O: Multiple primary
malignant tumors: a survey of the literature and statistical study.
Am J Cancer. 16:1358–1414. 1932.
|
|
2
|
Németh Z, Czigner J, Iván L, Ujpál M,
Barabás J and Szabó G: Quadruple cancer, including triple cancers
in the head and neck region. Neoplasma. 49:412–414. 2002.
|
|
3
|
Rahman GA and Mungadi IA: Surgical
trainees’ understanding of Dukes’ staging in rectal cancer. Niger J
Med. 18:75–78. 2009.PubMed/NCBI
|
|
4
|
Edge S, Byrd DR, Compton CC, Fritz AG,
Greene FL and Trotti A: Colon and rectum. AJCC Cancer Staging
Manual. 7th edition. Springer; New York: 2010
|
|
5
|
Kapsinow R: Multiple primary cancer. A
classification with report of cases. J La State Med Soc.
114:194–200. 1962.PubMed/NCBI
|
|
6
|
Hu NC, Hsieh SC, Chen TJ and Chang JY:
Multiple primary malignancies including colon, stomach, lung,
breast, and liver cancer: a case report and literature review. Chin
Med J (Engl). 122:3091–3093. 2009.
|
|
7
|
Irimie A, Achimas-Cadariu P, Burz C and
Puscas E: Multiple primary malignancies - epidemiological analysis
at a single tertiary institution. J Gastrointestin Liver Dis.
19:69–73. 2010.PubMed/NCBI
|
|
8
|
Pastore AL, Palleschi G, Autieri D, Leto
A, Ripoli A, Maggioni C, Moschese D, Al Salhi Y, Porta N, Di
Cristofano C, et al; Sapienza University of Rome, Faculty of
Pharmancy and Medicine. Synchronous primary neoplasms of the
bladder, skin and breast in a male patient: a case report. World J
Surg Oncol. 11:2822013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
He JJ: Meta analysis of 2025 cases with
multiple primary colorectal carcinoma. Zhonghua Wei Chang Wai Ke Za
Zhi. 9:225–229. 2006.(In Chinese). PubMed/NCBI
|
|
10
|
Papadopoulos V, Michalopoulos A, Basdanis
G, Pappolychroniadis K, Paramythiotis D, Fotiadis P, Berovalis P
and Harlaftis N: Synchronous and metachronous colorectal carcinoma.
Tech Coloproctol. 8(Suppl 1): s97–s100. 2004. View Article : Google Scholar
|
|
11
|
Balschun K, Haag J, Wenke AK, von
Schönfels W, Schwarz NT and Röcken C: KRAS, NRAS, PIK3CA exon 20,
and BRAF genotypes in synchronous and metachronous primary
colorectal cancers diagnostic and therapeutic implications. J Mol
Diagn. 13:436–445. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chaturvedi AK, Engels EA, Gilbert ES, Chen
BE, Storm H, Lynch CF, Hall P, Langmark F, Pukkala E, Kaijser M, et
al: Second cancers among 104,760 survivors of cervical cancer:
evaluation of long-term risk. J Natl Cancer Inst. 99:1634–1643.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hisada M, Garber JE, Fung CY, Fraumeni JF
Jr and Li FP: Multiple primary cancers in families with Li-Fraumeni
syndrome. J Nat Cancer Inst. 90:606–611. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Choong SS, Latiff ZA, Mohamed M, Lim LL,
Chen KS, Vengidasan L, Razali H, Abdul Rahman EJ and Ariffin H;
Malaysion Society of Paediatric Hameatology-Oncology. Childhood
adrenal cortical carcinoma as a sentinel cancer for detecting
families with germline TP53 mutations. Clin Genet. 82:564–568.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Nosho K, Kure S, Irahara N, Shima K, Baba
Y, Spiegelman D, Meyerhardt JA, Giovannucci EL, Fuchs CS and Ogino
S: A prospective cohort study shows unique epigenetic, genetic, and
prognostic features of synchronous colorectal cancers.
Gastroenterology. 137:1609–1620. e1–e3. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Söreide K, Janssen EA, Söiland H, Körner H
and Baak JP: Microsatellite instability in colorectal cancer. Br J
Surg. 93:395–406. 2006. View
Article : Google Scholar : PubMed/NCBI
|
|
17
|
Brumback RA, Gerber JE, Hicks DG and
Strauchen JA: Adenocarcinoma of the stomach following irradiation
and chemotherapy for lymphoma in young patients. Cancer.
54:994–998. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Escobar PA, Smith MT, Vasishta A, Hubbard
AE and Zhang L: Leukaemia-specific chromosome damage detected by
comet with fluorescence in situ hybridization (comet-FISH).
Mutagenesis. 22:321–327. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Agnelli L, Storti P, Todoerti K,
Sammarelli G, Dalla Palma B, Bolzoni M, Rocci A, Piazza F,
Semenzato G, Palumbo A, et al: Overexpression of HOXB7 and homeobox
genes characterizes multiple myeloma patients lacking the major
primary immunoglobulin heavy chain locus translocations. Am J
Hematol. 86:E64–E66. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Koutsopoulos AV, Dambaki KI, Datseris G,
Giannikaki E, Froudarakis M and Stathopoulos E: A novel combination
of multiple primary carcinomas: urinary bladder transitional cell
carcinoma, prostate adenocarcinoma and small cell lung carcinoma -
report of a case and review of the literature. World J Surg Oncol.
3:51–57. 2005. View Article : Google Scholar
|