Introduction
Skin cancer is one of the most common malignancies
in the USA, where >2,000,000 cases are diagnosed annually
(1). There are several types of
skin cancers, including basal cell carcinoma (BCC), squamous cell
carcinoma (SCC), and malignant melanoma (MM). BCC and SCC are
collectively termed non-melanoma skin cancer (NMSC). BCC usually
presents as a painless raised area of skin with an ulcer, which may
damage surrounding tissues, however, it is unlikley to metastasize
to distant organs. SCC may also form an ulcer, and often presents
as a hard red lump with a flat scaly surface. SCC is more likely to
metastasize to distant organs. Melanomas are the most aggressive
type of skin cancer, which present as a large, uneven mole that has
changed in color (2). The incidence
of skin cancer, particularly MM, is increasing, with an annual
growth rate of 3–5% in the USA, and appropriate preventive
approaches are urgently required (3,4).
Currently, known risk factors for the development of skin cancers
include fair skin, blue or green eyes, blond or red hair, multiple
moles, excess ultraviolet (UV) radiation from sun exposure, and a
history of severe sunburn and skin cancer (5). Primary strategies to prevent the
development and occurrence of skin cancers include reducing skin
cancer-related risk behaviors by avoidance of UV over-exposure, and
by the regular use of sunscreen creams (6,7).
Inflammation is associated with the development of
malignant tumors, particularly for epithelial cell tumors,
including skin cancers (8,9). Cyclooxygenase-2 (COX-2) controls
prostaglandin synthesis, regulating inflammation and the
development and progression of malignant tumors. Furthermore, COX-2
can positively regulate antiapoptotic, proangiogenic and other
tumorigenic processes, and is upregulated in human skin cancers
(10,11). Accordingly, chemotherapies with
COX-2 inhibitors and non-steroidal anti-inflammatory drugs (NSAIDs)
have been tested for the prevention of tumors in humans (12). Epidemiologically, treatment with
aspirin/NSAIDs benefits patients with various solid cancers, such
as colon cancer, esophageal cancer, and breast cancer (13). However, a previous meta-analysis
revealed no significant protective effect of non-aspirin NSAIDs in
preventing the development of skin cancers in humans (14).
Aspirin, also known as acetylsalicylic acid, is a
salicylate drug with analgesic, antipyretic and anti-inflammatory
activity. Aspirin is an inhibitor of COX-1 and COX-2, predominantly
affecting COX-1 (15). The efficacy
of treatment with aspirin for the prevention of tumor development
remains controversial. While several epidemiological studies have
demonstrated that treatment with aspirin may reduce the incidence
of skin cancers, other studies have yielded conflicting results
(16–26). Therefore, in the present study, a
meta-analysis was performed to evaluate the effect of aspirin on
the primary chemoprevention of skin cancer according to the
available clinical observational studies.
Materials and methods
Search strategy
A systematic literature search of MEDLINE (Pubmed),
BIOSIS, EMBASE, Cochrane Library, and China National Knowledge
Infrastructure was conducted to identify cohort and case-control
studies on aspirin intake and skin cancer development, published
between January 1980 and March 2013. The following medical subject
headings or keywords were used, without language restriction: i)
‘Aspirin’, ‘non-steroidal anti-inflammatory drugs’ or
‘acetylsalicylic acid’; ii) ‘skin cancer’, ‘skin tumor’, ‘melanoma
skin cancer’, ‘non-melanoma skin cancer’, ‘squamous cell
carcinoma’, or ‘basal cell carcinoma’. The cited references in
retrieved articles were also screened to identify any additional
relevant studies.
Study selection
The titles and abstracts of individual publications
were screened, and the nature of each study was evaluated
independently by two reviewers (Zhu and Cheng). The studies were
included if they met all of the following criteria: i) Had a
case-control or cohort design, ii) evaluated exposure to aspirin,
iii) reported occurrence of skin cancer diagnosis, and iv) reported
the adjusted relative risks (RRs), hazard ratios (HRs), or odds
ratios (ORs), as well as the corresponding 95% CI. If publications
were duplicated or if articles came from the same study population,
the study with the largest sample size was included.
Data extraction and quality
assessment
Data were extracted from individual publications by
two reviewers (Zhu and Cheng), independently and in a blinded
manner (without prior knowledge of the year of publication, author
and journal). The extracted data included authors, publication
year, population, sample size, medication type and frequency of
use, information source for measurement of aspirin exposure and for
identification of skin cancer cases (e.g. questionnaire, interview,
pharmacy database), ORs or RRs with and without adjustment for
potential confounders, potential confounders used for adjustment
(e.g. age, skin color) and the study design (cohort vs.
case-control). If there was a disagreement, the data were further
discussed by two reviewers until a consensus was reached.
The methodological quality of each study was
assessed using the Newcastle-Ottawa Scale (NOS) (27), by evaluation of the following three
areas: The selection of study groups, comparability of groups, and
ascertainment of either the exposure or outcome of interest for
case-control or cohort studies, respectively. If a study had a
score ≥5 out of a maximum score of 9, the study was considered to
be of high-quality.
Data analysis and risk of bias
All aspirin-related chemopreventive studies of skin
cancer were analyzed simultaneously and further stratified,
according to study design (cohort vs. case-control), method for
determining exposure to aspirin (i.e. questionnaire vs. pharmacy
database), method for identifying skin cancer cases (self-reported
vs. medical records and pathology), histological type (SCC vs. BCC
vs. MM), gender (men vs. women), duration of medication use, and
study population (American vs. European).
Potential publication bias was assessed using
qualitative and quantitative methods. Initially, it was evaluated
by funnel plots of the ORs versus their standard errors, and
subsequently by the Begg’s test (rank correlation method) (28) and Egger’s test (linear regression
method) (29). P>0.10 was
considered to indicate no publication bias.
Statistical analysis
OR was used as a common measure across all studies
for determining the degree of a potential association between
aspirin intake and risk of development of skin cancer. The RRs and
HRs were directly considered as ORs. The potential heterogeneity in
the results across the studies was examined by Cochran’s Q and
I2 statistics (30). If
a P value for heterogeneity was <0.10 or I2 was
>50%, substantial heterogeneity was considered and the summary
was estimated on the basis of the random-effect model, as described
by DerSimonian and Laird (31). The
sensitivity was analyzed by excluding each study individually to
evaluate the consistency of our results. All analyses were
performed using STATA version 10.0 (StataCorp LP, College Station,
TX, USA).
Results
Literature search
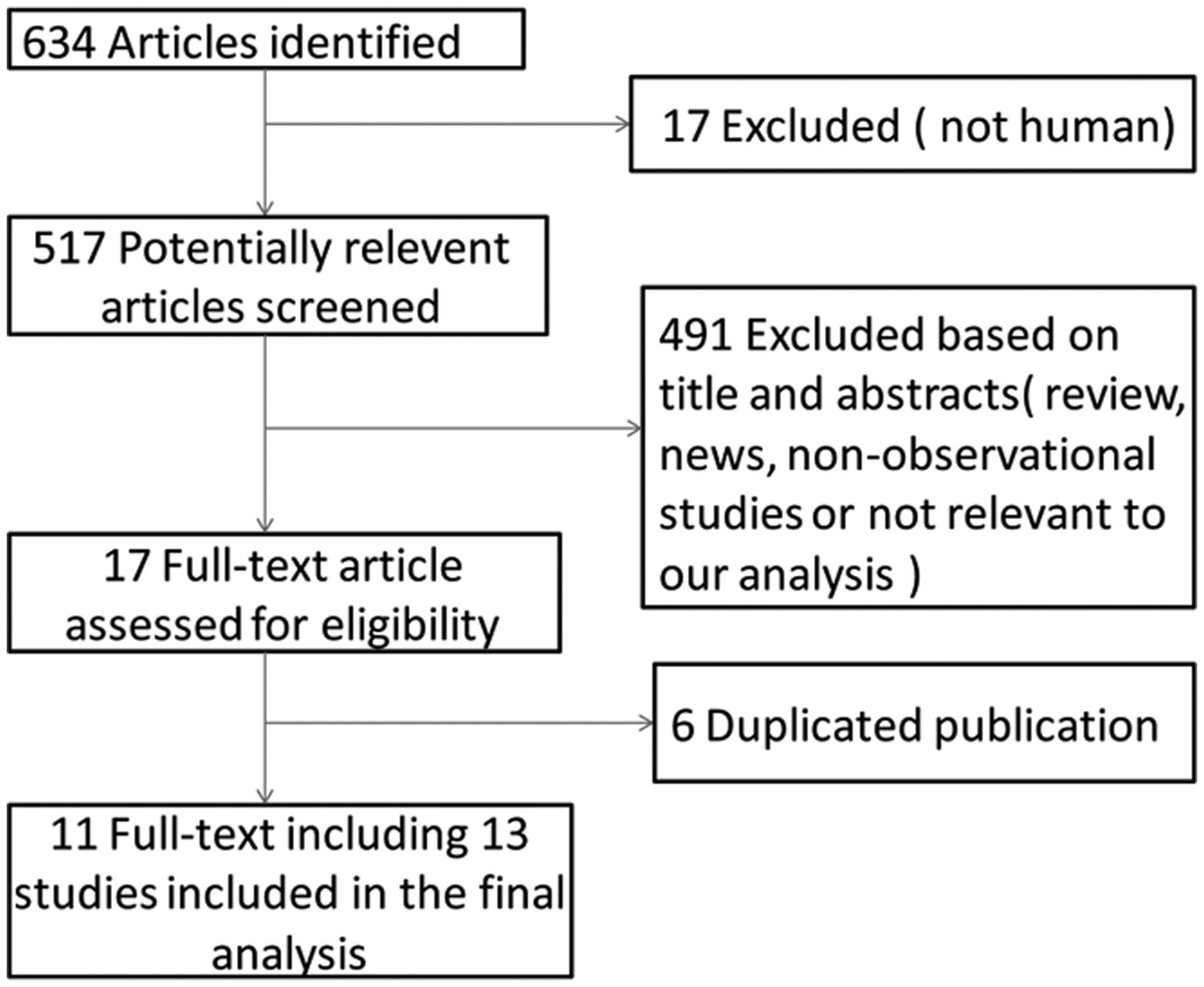
A total of 634 relevant publications were identified
by a systematic literature search, and 623 out of 634 publications
were excluded due to duplications or various other reasons (e.g. if
the publications were review papers or news articles, or related to
randomized controlled studies or animal experiments), according to
the titles and abstracts. Finally, eight case-control studies
(16,19,22,24–26)
and five cohort studies (17,18,20,21,23)
were included in the meta-analysis. A flow chart (Fig. 1) illustrates the process of
selection of relevant studies.
Study characteristics and quality
assessment
According to the inclusion criteria, a total of
eight case-control studies with 21,356 cases and 187,037 controls
and five cohort study incorporating 294,377 participants were
included in the meta-analysis. The main characteristics of these
studies are summarized in Table I.
All research literature was in English; three studies were based in
Denmark (24), one in the
Netherlands (25), and nine in the
USA (16–23). Seven studies (16–19,21,22,24–26)
included both genders and two studies included only females
(20,23). The majority of studies had matched
cases and controls, and had adjusted for a wide range of potential
confounders, including age, gender, ethnicity, skin color, hair
color, amount of sun exposure, history of severe sunburns, number
of moles, family history of skin cancer, smoking status and other
factors.
 | Table ICharacteristics of epidemiological
studies of aspirin intake and skin cancer risk included in the
meta-analysis. |
Table I
Characteristics of epidemiological
studies of aspirin intake and skin cancer risk included in the
meta-analysis.
| Study | Ethnicity | Design | Gender | Cancer type | Participants,
n | Patients, n | Exposure
source | Cancer
confirmed | Confounders
included in adjusted estimates |
|---|
| Gamba 2013
(20) | USA | Cohort | Female only | MM | 59,806 | 548 | Prescription
records | Medical
records |
a1,a2,b,c1,d1,e1,h1,l,m,p1,r1,s1,s2,s3,t1 |
| Jeter 2012
(23) | USA | Cohort | Female only | MM | 92,125 | 658 | Self-reported | Self-reported |
a1,a2,b,f1,h2,n,p1,p2, |
| | | | SCC | | 1,337 | | Self-reported |
q,r1,s1,s3,s4,v1,v2 |
| | | | BCC | | 15,079 | | Medical
records | |
| Johannesdottir
2012[1] (24) | Denmark | Case-control | Female and
male | MM | 196,529 | 3,089 | Prescription
records | Pathology |
a1,c2,d2,g1,g2,t2 |
| Johannesdottir
2012[2] (24) | Denmark | Case-control | Female and
male | SCC | | 1,921 | Prescription
records | Pathology |
a1,c2,d2,g1,g2,t2 |
| Johannesdottir
2012[3] (24) | Denmark | Case-control | Female and
male | BCC | | 12,864 | Prescription
records | Pathology |
a1,c2,d2,g1,g2,t2 |
| Cahoon, 2012
(18) | USA | Cohort | Female and
male | BCC | 58,213 | 2,291 | Self-reported | Medical records and
self-reported | a1,a2,g1,r1 |
| Jeter 2011
(22) | USA | Case-control | Female and
male | MM | 446 | 327 | Self-reported | Medical
records | a1,f1,g1,n,s5 |
| Cruiel 2011
(19) | USA | Case-control | Female and
male | MM | 1,000 | 400 | Self-reported | Self-reported | a1,g1, s4,t2 |
| Torti 2011
(26) | USA | Case-control | Female and
male | SCC | 1,484 | 535 | Self-reported | Medical
records |
a1,c1,g1,s3,s4,s5 |
| | | | BCC | | 487 | | | |
| Asgari 2010
(16) | USA | Case-control | Female and
male | SCC | 830 | 415 | Self-reported and
prescription records | Medical
records | h2, o |
| Joosse 2009
(25) | Netherlands | Case-control | Female and
male | MM | 8,104 | 1,318 | Prescription
records | Medical
records |
a1,d3,g1,g2,s7,t2,y |
| Asgari 2008
(17) | USA | Cohort | Female and
male | MM | 63,809 | 349 | Self-reported | Medical
records | a1,c3,d3,e1,e2,f1,
f2,g1,h1,h3,s4,v3 |
| Jacobs 2007
(21) | USA | Cohort | Female and
male | MM | 18,127 | 1,049 | Self-reported | Medical
records | a1,b,d3,e1,g1,
g2,m,r2,p1,s3 |
The quality scores of these studies are summarized
in Table IIA and IIB. The range of
quality scores was from 6–9. The average scores of case-control
studies and cohort studies were 7.8 and 8.0, respectively. All
studies were considered to be of high-quality.
| Table II
|
Table II
| A, Methodological
quality of case-control studies |
|---|
|
|---|
| Selectiona | | Exposurea |
|---|
|
| |
|
|---|
| Study | Adequate definition
of cases | Representativeness
of cases | Selection of
control subjects | Definition of
control subjects |
Comparabilityb | Exposure
assessment | Same method of
ascertainment for all subjects | Non-response
rate | Total scores |
|---|
| Johannesdottir
2012[1] (24) | * | * | * | * | ** | * | * | - | 8 |
| Johannesdottir
2012[2] (24) | * | * | * | * | ** | * | * | - | 8 |
| Johannesdottir
2012[3] (24) | * | * | * | * | ** | * | * | - | 8 |
| Jeter 2011
(22) | * | * | - | * | * | * | * | - | 6 |
| Cruiel 2011
(19) | * | * | * | * | ** | * | * | - | 8 |
| Torti 2011
(26) | * | * | * | * | ** | * | * | - | 8 |
| Asgari 2010
(16) | * | * | * | * | ** | * | * | - | 8 |
| Joosse 2009
(25) | * | * | * | * | ** | * | * | - | 8 |
|
| B, Methodological
quality of cohort studies |
|
| Selectiona | | Outcomea |
|
| |
|
| Study | Representativeness
of exposed cohort | Representativeness
of nonexposed cohort | Ascertainment of
exposure | Outcome of
interest |
Comparabilityb | Assessment of
outcome | Length of
follow-upc | Adequacy of
follow-upd | Total scores |
|
| Gamba 2013
(20) | * | * | * | * | ** | * | * | * | 9 |
| Jeter 2012
(23) | - | * | * | * | * | * | * | * | 7 |
| Cahoon 2012
(18) | * | * | * | * | ** | * | - | * | 8 |
| Asgari 2008
(17) | * | * | * | * | ** | * | - | * | 8 |
| Jacobs 2007
(21) | * | - | * | * | ** | * | * | * | 8 |
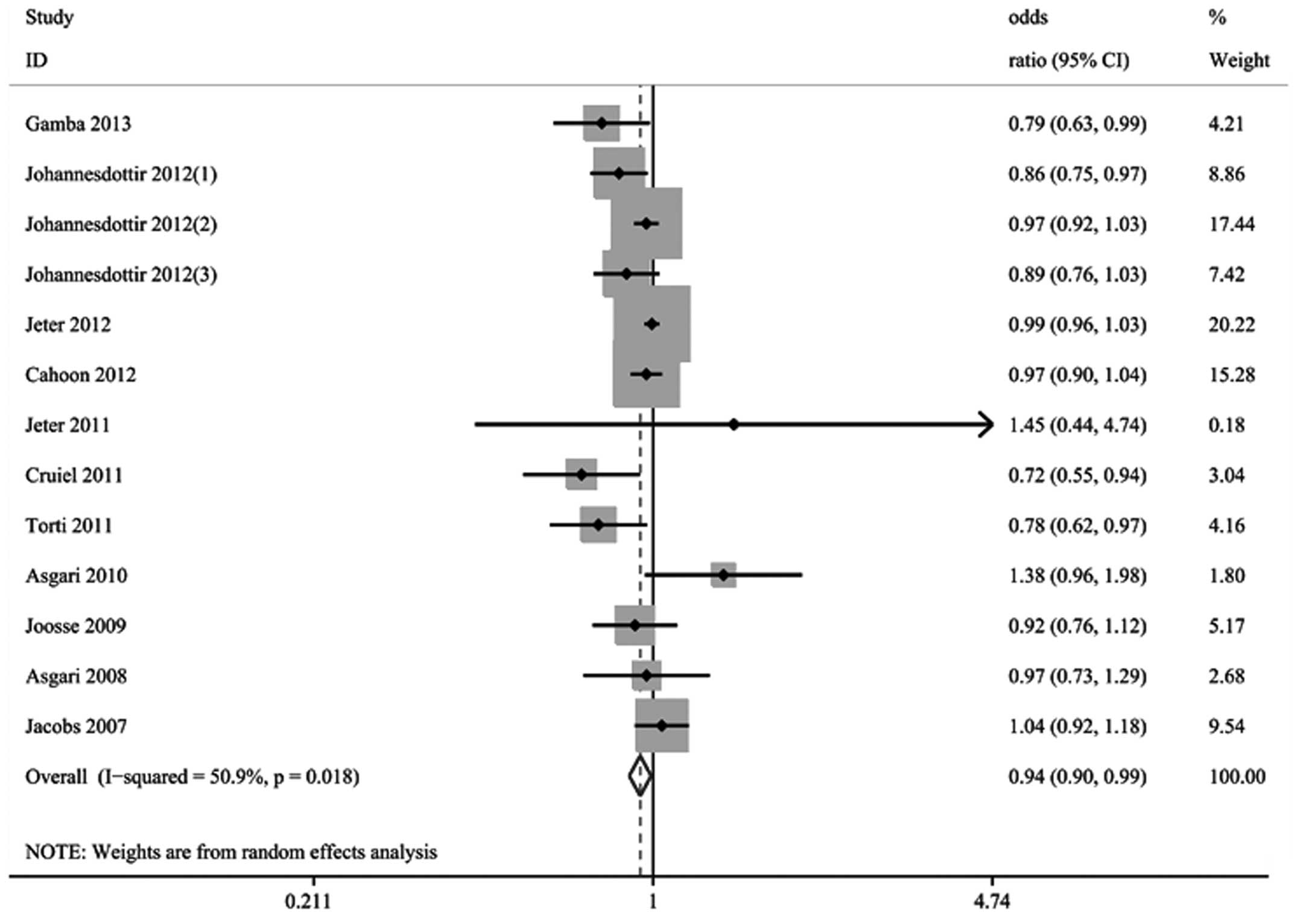
Overall analyses and bias assessment
All studies reported OR and 95% CI for aspirin
exposure and risk of skin cancer after adjusting for confounding
factors. The pooled results indicated that regular aspirin exposure
decreased the risk of developing skin cancers by 6% (OR, 0.94; 95%
CI, 0.90–0.99). Statistical analyses revealed significant
heterogeneity among the studies (P=0.02; I2=50.9%;
Fig. 2). The sensitivity analyses,
by excluding any single study in each step, revealed that only one
[Jeter et al (23)] out of
13 studies included was considered to have a high risk of
differential-verification bias. Exclusion of this study decreased
the heterogeneity, but did not alter the results (OR, 0.95; 95% CI,
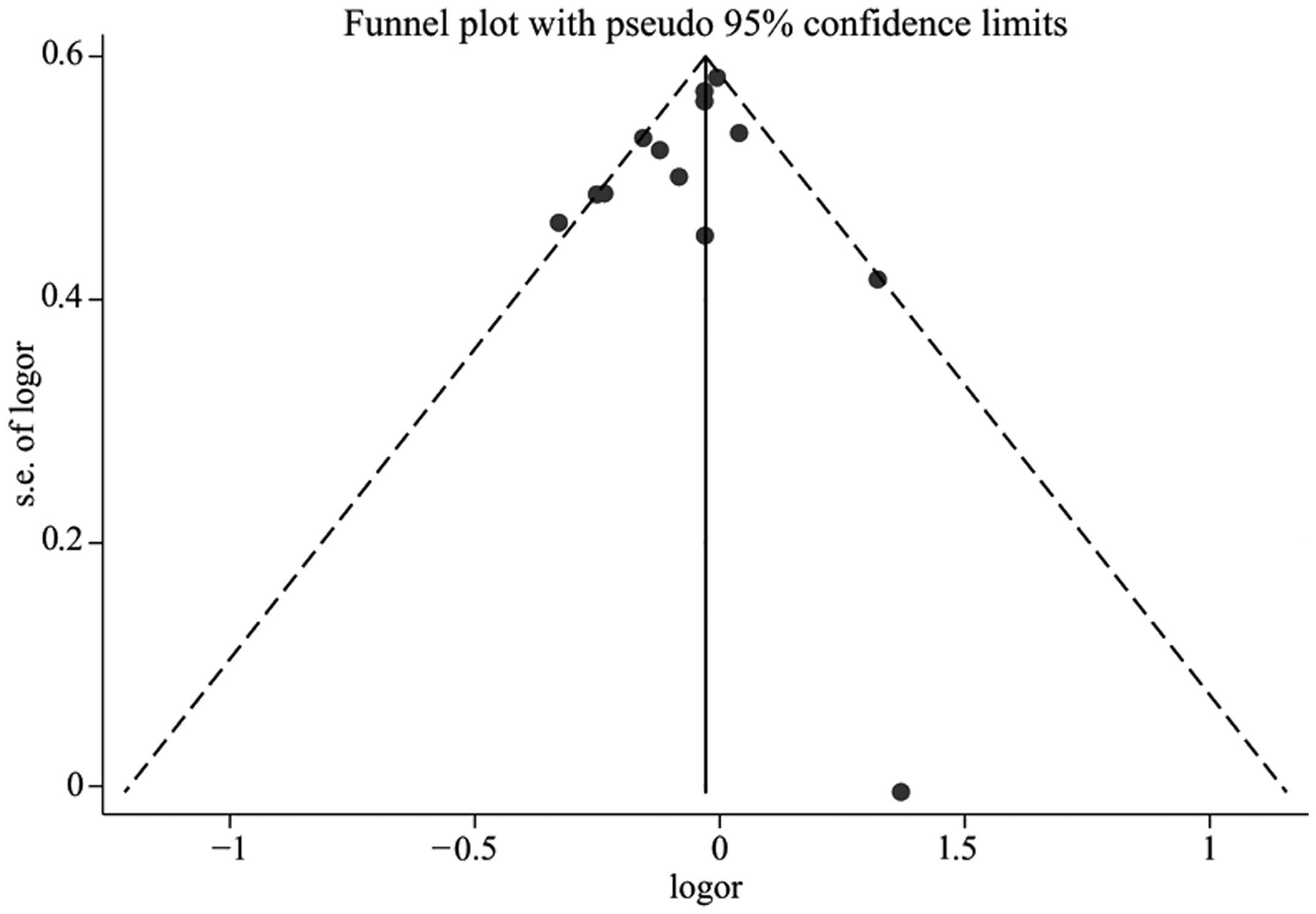
0.91–0.98; P=0.04; I2= 47.1%). No indication of a
publication bias was identified either from the funnel plot
(Fig. 3), or from the Egger’s test
(P=0.17) or Begg’s test (P=0.67).
Subgroup analysis
The effects of aspirin intake on the risk of skin
cancer in subgroup meta-analyses are shown in Table III. Compared with the overall
analysis, the results from individual subgroup analyses were
similar: Case-control studies (OR, 0.90; 95% CI, 0.82–0.99; P=0.03;
I2=53.9%), medical record of skin cancer (OR, 0.95; 95%
CI, 0.92–0.99; P=0.08; I2=40.1%), and continual intake
of low dose aspirin (OR, 0.95; 95% CI, 0.90–0.99; P=0.15;
I2=40.0%). Aspirin intake exerted significant protective
effects against the development of SCC (OR, 0.90; 95% CI,
0.82–0.98; P=0.22; I2=31.7%) and in the non-American
population (OR, 0.94; 95% CI, 0.90–0.99; P=0.29;
I2=20.7%), whilst it had marginal protective effects on
the development of BCC (OR, 0.98; 95% CI, 0.95–1.00; P=0.64;
I2=0%). However, no significant protective effects were
observed in the other relevant strata.
| Table IIISummary odds ratios of the
association between aspirin intake and skin cancer risk. |
Table III
Summary odds ratios of the
association between aspirin intake and skin cancer risk.
| ORa | 95% CIa | I2,
% | P-value for
homogeneity | Studies, n |
|---|
| Study design |
| Case-control | 0.90 | 0.82–0.99 | 53.9 | 0.03 | 8 |
| Cohort | 0.99 | 0.96–1.02 | 20.3 | 0.29 | 5 |
| Histological
type |
| NMSC | 0.97 | 0.95–0.99 | 25.9 | 0.22 | 6 |
| SCC | 0.90 | 0.82–0.98 | 31.7 | 0.22 | 4 |
| BCC | 0.98 | 0.95–1.00 | 0.0 | 0.64 | 4 |
| MM | 0.96 | 0.82–1.12 | 69.3 | 0.00 | 7 |
| Exposure
determination |
| Prescription
records | 0.92 | 0.84–1.01 | 52.6 | 0.06 | 6 |
| Self-reported | 0.98 | 0.96–1.01 | 45.6 | 0.07 | 7 |
| Disease
determination |
| Medical
records | 0.95 | 0.92–0.99 | 40.1 | 0.08 | 11 |
| Self-reported | 0.87 | 0.64–1.19 | 81.7 | 0.02 | 2 |
| Gender |
| Female | 0.88 | 0.74–1.04 | 62.1 | 0.05 | 4 |
| Male | 0.85 | 0.68–1.07 | 0.0 | 0.34 | 2 |
| Duration of aspirin
use |
| Short term | 0.92 | 0.83–1.04 | 66.0 | 0.00 | 8 |
| Long term | 0.90 | 0.78–1.05 | 69.1 | 0.00 | 8 |
| Dose effects |
| High dose | 1.01 | 0.90–1.14 | 0.0 | 5.39 | 7 |
| Low dose | 0.95 | 0.90–0.99 | 40.3 | 0.15 | 5 |
| Study
population |
| American | 0.95 | 0.88–1.02 | 56.5 | 0.02 | 9 |
| Non-American | 0.94 | 0.90–0.99 | 20.7 | 0.29 | 4 |
Sensitivity analysis
In the sensitivity analyses, the combined results
were recalculated by excluding one study per iteration. After
excluding one particular study [Jeter et al (23)], the remaining studies retained
significant heterogeneity, and indicated that aspirin exposure had
significant protective effects on MM. However, exclusion of the
Jeter et al (23) study
reduced the heterogeneity among the remaining studies and indicated
that short term aspirin intake may decrease the risk of skin cancer
in females (data not shown).
Discussion
The results of the current study extend and support
the previous observation that aspirin intake is associated with a
decreased risk of developing skin cancer. However, the results must
be interpreted with caution, due to the substantial heterogeneity
among the studies included in this meta-analysis. This was
anticipated given the difference in the study populations, study
designs, gender and age of the participants, the method of
ascertainment of patients and dosage and duration of medication,
follow-up time and adjustment variables across studies. The
sensitivity analyses indicated that the study conducted by Jeter
et al (23) potentially
caused significant heterogeneity in the pooled data, as this study
was conducted in well-educated nurses with greater awareness of
health concerns.
The current study included high-quality
observational studies on aspirin intake for the primary prevention
of skin cancer. The results from the case-control studies indicated
a significant protective association between aspirin intake and a
reduced risk of primary skin cancers, while the results from the
cohort studies indicated only a borderline significance in the
protective effects of aspirin intake against skin cancer.
Cohort studies are regarded to be the most accurate
observational studies, however, the value of a cohort study depends
on its overall quality. The report by Jeter et al (23) only comprised nurses, whilst Jacobs
et al (21) and Asgari et
al (15) did not confirm skin
reactions to sun exposure, family history, and the number of moles,
which are the main risk factors for skin cancers. Studies have
reported a marked increase in the incidence among the younger
population, particularly in females <40 years of age, which
increased from 28.8 individuals per 100,000 of the population in
1990 to 33.1 individuals per 100,000 of the population in 2000
(32). However, Gamba et al
(20) studied postmenopausal
females only and Asgari et al (17) studied subjects aged between 50 and
76 years, therefore these two cohort studies were not
representative of the whole population. The absence of validated
reports of aspirin use with prescription records should also be
taken into account when interpreting these results.
The results from case-control studies in general
must be interpreted with caution due to the methodological
limitations. Jeter et al (22) studied the spouses of patients as the
controls, and this may cause have potential selection bias in the
control group as a number of spouses of the studied subjects did
not participate in the study. Johannesdottir et al (24), studied cases identified through the
Danish Cancer Registry, in which only ~60% of SCC and BCC cases
were recorded. The incompleteness of tumor records may also cause a
potential bias affecting the results. In addition, a number of the
case-control studies had a moderate sample size, which may
overestimate the treatment effect.
Stratification analyses indicated that aspirin
intake reduced the risk of development of NMSC, but not of MM.
Similarly, aspirin intake had a more significant protective effect
against the development of SCC than BCC. This difference may be
attributed to the differential levels of COX expression in these
different types of skin cancers. Indeed, COX-2 expression is
upregulated in SCC, whilst levels of COX expression in BCC and MM
are controversial (33–35).
In addition, we observed that aspirin intake exerted
borderline statistically significant effects on the development of
skin cancers between females (OR, 0.88; 95% CI, 0.74–1.04) and
males (OR, 0.85; 95% CI, 0.68–1.07). Gamba et al (20) demonstrated that aspirin intake may
be chemopreventive against the development of melanoma in
postmenopausal women, consistent with a previous study that
indicated a similar effect against colorectal cancer (36). However, two studies on aspirin
intake for preventing breast cancer obtained conflicting results in
postmenopausal females (37,38).
Further studies into the potential association of aspirin intake
with protection from skin cancer in postmenopausal females are
required to gain further insight.
Stratification analyses also revealed that low dose
aspirin intake (≤150 mg) exerted a marginal protective effect on
the development of skin cancer, while high dose aspirin intake
(>150 mg) did not show any protective effect. However, the
categories of aspirin dosages varied across the studies, and the
estimated dose in individual studies was based on study-specific
definitions; 150 mg was set as a cut off value. A daily dose of
≤150 mg was considerd to be a ‘low-dose’ while a daily dose of
>150 mg was considerd to be a ‘high-dose’. Thus, the effect of
aspirin intake may be better considered as an inverse dose-risk
correlation.
Additionally, stratification analyses indicated that
aspirin intake for a short (≤5 years) or long (>5 years) time
period was associated with a reduced risk of development of skin
cancers. These results may stem from limited sample sizes in some
groups of subjects, leading to less power to achieve a meaningful
conclusion. Continual intake of aspirin has, however, been
associated with a reduced risk of other types of tumors (39).
Aspirin intake had a marginal protective effect
against the development of skin cancer in Americans, however, the
study also revealed a significant protective effect against skin
cancer in other Caucasian populations. The varying association
levels may be due to the dissimilarities in the baseline risk of
skin cancer between these populations.
There were several potential limitations to the
present meta-analysis. Firstly, the analysis was based solely on
observational studies, which identify only the potential
association between the two factors, and not causality. Secondly,
considerable heterogeneity was present among the included trials,
which may have impacted the results. Thirdly, some patients taking
aspirin may also have taken other NSAIDs, which may confound the
results, yet few studies have adjusted for this factor. Further
large-scale, well-designed randomized controlled trials are needed
to validate the protective effect of aspirin intake on the
development of skin cancer.
In summary, the current meta-analysis of
observational studies indicated that aspirin intake, particularly
with continual small doses, was significantly associated with a
reduced risk for the development of skin cancer, primarily SCC and
BCC, in both females and males. These findings may have important
public health implications. However, the causative protection
against skin cancers by aspirin intake remains to be confirmed.
Acknowledgements
The authors would like to thank Medjaden Bioscience
Limited for assisting in the preparation of this manuscript.
References
|
1
|
D’Orazio J, Jarrett S, Amaro-Ortiz A and
Scott T: UV radiation and the skin. Int J Mol Sci. 14:12222–12248.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Marks R: An overview of skin cancers.
Incidence and causation. Cancer. 75:607–612. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chen ST, Geller AC and Tsao H: Update on
the Epidemiology of Melanoma. Curr Dermatol Rep. 2:24–34. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
MacKie RM, Hauschild A and Eggermont AM:
Epidemiology of invasive cutaneous melanoma. Ann Oncol. 20(Suppl
6): vi1–vi7. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Saladi RN and Persaud AN: The causes of
skin cancer: a comprehensive review. Drugs Today (Barc). 41:37–53.
2005. View Article : Google Scholar
|
|
6
|
Council on Environmental Health, Section
on Dermatology. Balk SJ: Ultraviolet radiation: a hazard to
children and adolescents. Pediatrics. 127:588–597. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kornek T and Augustin M: Skin cancer
prevention. J Dtsch Dermatol Ges. 11:283–296; quiz 297–298.
2013.PubMed/NCBI
|
|
8
|
Buckman SY, Gresham A, Hale P, et al:
COX-2 expression is induced by UVB exposure in human skin:
implications for the development of skin cancer. Carcinogenesis.
19:723–729. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Fosslien E: Molecular pathology of
cyclooxygenase-2 in neoplasia. Ann Clin Lab Sci. 30:3–21.
2000.PubMed/NCBI
|
|
10
|
Denkert C, Köbel M, Berger S, et al:
Expression of cyclooxygenase 2 in human malignant melanoma. Cancer
Res. 61:303–308. 2001.PubMed/NCBI
|
|
11
|
Nijsten T, Colpaert CG, Vermeulen PB, et
al: Cyclooxygenase-2 expression and angiogenesis in squamous cell
carcinoma of the skin and its precursors: a paired
immunohistochemical study of 35 cases. Br J Dermatol. 151:837–845.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Rao CV and Reddy BS: NSAIDs and
chemoprevention. Curr Cancer Drug Targets. 4:29–42. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Harris RE, Beebe-Donk J, Doss H and Burr
Doss D: Aspirin, ibuprofen, and other non-steroidal
anti-inflammatory drugs in cancer prevention: a critical review of
non-selective COX-2 blockade (review). Oncol Rep. 13:559–583.
2005.PubMed/NCBI
|
|
14
|
Silva MT, Galvao TF, Zimmerman IR, Pereira
MG and Lopes LC: Non-aspirin non-steroidal anti-inflammatory drugs
for the primary chemoprevention of non-gastrointestinal cancer:
summary of evidence. Curr Pharm Des. 18:4047–4070. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sneader W: The discovery of aspirin: a
reappraisal. BMJ. 321:1591–1594. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Asgari MM, Chren MM, Warton EM, Friedman
GD and White E: Association between nonsteroidal anti-inflammatory
drug use and cutaneous squamous cell carcinoma. Arch Dermatol.
146:388–395. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Asgari MM, Maruti SS and White E: A large
cohort study of nonsteroidal anti-inflammatory drug use and
melanoma incidence. J Natl Cancer Inst. 100:967–971. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Cahoon EK, Rajaraman P, Alexander BH,
Doody MM, Linet MS and Freedman DM: Use of nonsteroidal
anti-inflammatory drugs and risk of basal cell carcinoma in the
United States Radiologic Technologists study. Int J Cancer.
130:2939–2948. 2012. View Article : Google Scholar
|
|
19
|
Curiel-Lewandrowski C, Nijsten T, Gomez
ML, Hollestein LM, Atkins MB and Stern RS: Long-term use of
nonsteroidal anti-inflammatory drugs decreases the risk of
cutaneous melanoma: results of a United States case-control study.
J Invest Dermatol. 131:1460–1468. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Gamba CA, Swetter SM, Stefanick ML, et al:
Aspirin is associated with lower melanoma risk among postmenopausal
Caucasian women: the Women’s Health Initiative. Cancer.
119:1562–1569. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Jacobs EJ, Thun MJ, Bain EB, Rodriguez C,
Henley SJ and Calle EE: A large cohort study of long-term daily use
of adult-strength aspirin and cancer incidence. J Natl Cancer Inst.
99:608–615. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Jeter JM, Bonner JD, Johnson TM and Gruber
SB: Nonsteroidal anti-inflammatory drugs and risk of melanoma. J
Skin Cancer. 2011:5985712011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Jeter JM, Han J, Martinez ME, Alberts DS,
Qureshi AA and Feskanich D: Non-steroidal anti-inflammatory drugs,
acetaminophen, and risk of skin cancer in the Nurses’ Health Study.
Cancer Causes Control. 23:1451–1461. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Johannesdottir SA, Chang ET, Mehnert F,
Schmidt M, Olesen AB and Sørensen HT: Nonsteroidal
anti-inflammatory drugs and the risk of skin cancer: a
population-based case-control study. Cancer. 118:4768–4776. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Joosse A, Koomen ER, Casparie MK, Herings
RM, Guchelaar HJ and Nijsten T: Non-steroidal anti-inflammatory
drugs and melanoma risk: large Dutch population-based case-control
study. J Invest Dermatol. 129:2620–2627. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Torti DC, Christensen BC, Storm CA, et al:
Analgesic and nonsteroidal anti-inflammatory use in relation to
nonmelanoma skin cancer: a population-based case-control study. J
Am Acad Dermatol. 65:304–312. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Wells GA, Shea B, O’Connell D, et al: The
Newcastle-Ottawa Scale (NOS) for assessing the quality of
nonrandomised studies in meta-analyses. Department of Epidemiology
and Community Medicine, University of Ottawa; Canada: http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm.
Accessed October 12, 2007
|
|
28
|
Begg CB and Mazumdar M: Operating
characteristics of a rank correlation test for publication bias.
Biometrics. 50:1088–1101. 1994. View
Article : Google Scholar : PubMed/NCBI
|
|
29
|
Egger M, Davey Smith G, Schneider M and
Minder C: Bias in meta-analysis detected by a simple, graphical
test. BMJ. 315:629–634. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Higgins JP, Thompson SG, Deeks JJ and
Altman DG: Measuring inconsistency in meta-analyses. BMJ.
327:557–560. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
DerSimonian R and Laird N: Meta-analysis
in clinical trials. Control Clin Trials. 7:177–188. 1986.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Christenson LJ, Borrowman TA, Vachon CM,
et al: Incidence of basal cell and squamous cell carcinomas in a
population younger than 40 years. JAMA. 294:681–690. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
An KP, Athar M, Tang X, et al:
Cyclooxygenase-2 expression in murine and human nonmelanoma skin
cancers: implications for therapeutic approaches. Photochem
Photobiol. 76:73–80. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Asgari M, White E and Chren MM:
Nonsteroidal anti-inflammatory drug use in the prevention and
treatment of squamous cell carcinoma. Dermatol Surg. 30:1335–1342.
2004.PubMed/NCBI
|
|
35
|
Fürstenberger G, Marks F and Müller-Decker
K: Cyclooxygenase-2 and skin carcinogenesis. Prog Exp Tumor Res.
37:72–89. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Cole BF, Logan RF, Halabi S, et al:
Aspirin for the chemoprevention of colorectal adenomas:
meta-analysis of the randomized trials. J Natl Cancer Inst.
101:256–266. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Bardia A, Olson JE, Vachon CM, et al:
Effect of aspirin and other NSAIDs on postmenopausal breast cancer
incidence by hormone receptor status: results from a prospective
cohort study. Breast Cancer Res Treat. 126:149–155. 2011.
View Article : Google Scholar
|
|
38
|
Zhang X, Smith-Warner SA, Collins LC,
Rosner B, Willett WC and Hankinson SE: Use of aspirin, other
nonsteroidal anti-inflammatory drugs, and acetaminophen and
postmenopausal breast cancer incidence. J Clin Oncol. 30:3468–3477.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Burn J, Gerdes AM, Macrae F, et al: CAPP2
Investigators: Long-term effect of aspirin on cancer risk in
carriers of hereditary colorectal cancer: an analysis from the
CAPP2 randomised controlled trial. Lancet. 378:2081–2087. 2011.
View Article : Google Scholar : PubMed/NCBI
|