Introduction
Merkel cell carcinoma (MCC), also known as
trabecular carcinoma of the skin, is a primary cutaneous
neuroendocrine malignancy with a low incidence rate and a high rate
of aggressive biological behavior. The tumor most commonly occurs
in the sun-exposed areas of Caucasians aged >50 years; primarily
on the head and neck, followed by the extremities, trunk and
buttocks (1,2). The clinical manifestation of MCC is
that of a solitary, firm, glossy, painless cutaneous nodule, with
red- or purple-colored skin, which may exhibit ulcerative
characteristics. Histologically, MCC exhibits sheets of
monomorphous small blue cells, which may be confused with other
closely associated skin neoplasms, such as small cell lung cancer
(SCLC), cutaneous lymphoma, melanoma, Ewing’s sarcoma and rare
basal cell carcinoma (3). The
positive expression of certain antibodies in immunohistochemical
staining is confirmed to be an important diagnostic tool to
distinguish MCC from these tumors.
A retrospective review was previously conducted by
Song et al (4) to describe
the clinical profile of MCC in China. The results indicated that
MCC appeared to be uncommon in mainland China, and that patients
often developed lesions on the head/neck region, as observed in
Western countries, but received surgery alone as treatment. The
present study reports the case of a Chinese male who presented with
an unusual nodule in the left groin, without sun exposure, which
was initially diagnosed as a malignant lymphoma, but was later
proven to be an MCC following immunohistochemical studies. Written
informed consent was obtained from the patient and the patient’s
family.
Case report
A 66-year-old Chinese male presented to the
Deaprtment of Pathology, The Third Affiliated Hospital of Soochow
University (Changzhou, China) in May 2009 with complaints of a 2-cm
asymptomatic, smooth and firm nodule in the left inguinal region.
There was no discoloration or other visible abnormality of the
overlying skin. Surgical excision of the lesion was performed and a
diagnosis of malignant lymphoma was formed at the Changzhou No.2
People’s Hospital (Changzhou, China). The patient’s medical history
revealed a previous resection of a similar painless nodule in the
subcutaneous region of the left knee 6 months previously, but a
pathological examination had not been performed. The nodule in the
left groin was suspected to be a metastatic lesion.
Upon review of 4-μm sections of the lesion by light
microscopy, the entire thickness of the dermis was observed to be
widely infiltrated by small round monomorphic cells, with minimal
cytoplasm, hyperchromatic nuclei and small nucleoli (Fig. 1A). Apparent nuclear atypia and
multiple mitotic figures were observed. These neoplastic cells
showed diffuse distribution and infiltrated into the deep
mesenchyme, where blood vessels were plentiful (Fig. 1B and C). Immunohistochemical
staining was performed on 4-μm thick, formalin-fixed,
paraffin-embedded tissue sections provided by the external
hospital. The results demonstrated that the tumor cells were
strongly positive for neuroendocrine markers, including
chromogranin A (CgA) and synaptophysin (Syn), and epithelial
markers cytokeratin (CK) 20, CK8/18 and epithelial membrane antigen
(EMA) (Fig. 1D–H), but negative for
leukocyte common antigens (LCA), thyroid transcription factor-1
(TTF-1), Melan-A, human melanoma black 45 (HMB45), vimentin (Vim),
S-100, cluster of differentiation (CD)34, CD57 and CD99. These
histopathological and immunohistochemical features were consistent
with a diagnosis of MCC. Therefore, a corrected diagnosis of MCC
was made for this patient.
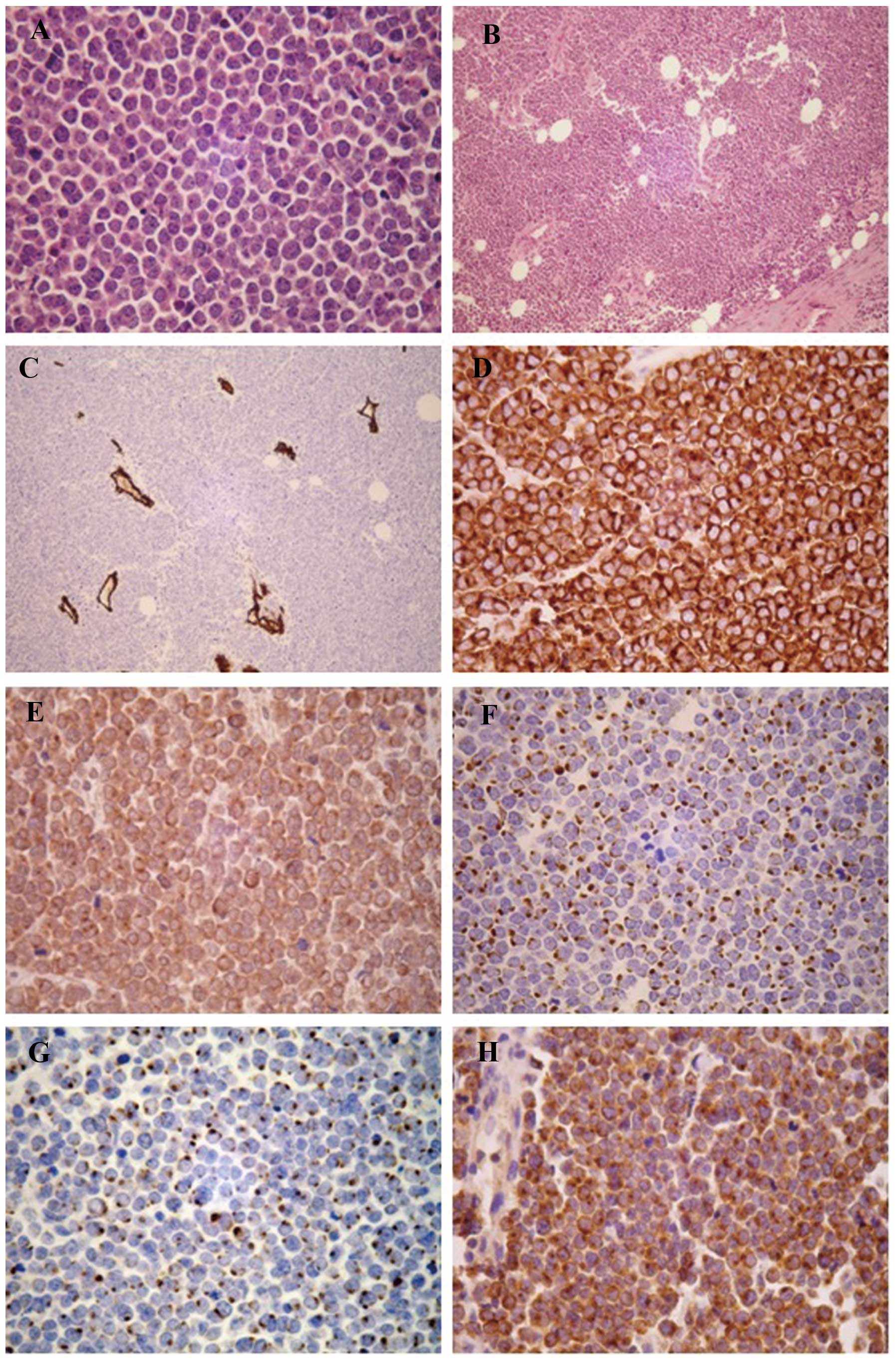 | Figure 1(A) Sheets of round to oval, small,
blue cells with amphophilic sparse cytoplasm and vesicular nuclei
[hematoxylin and eosin (HE); magnification, ×400). (B) Diffuse
distribution of neoplastic cells and deep mesenchyme infiltration
(HE; magnification, ×100). (C) Vascular proliferation in
interstitial substance with staining for cluster of differentiation
34 (magnification, ×100). (D) Merkel cell carcinoma (MCC) with
diffusely-positive staining for synaptophysin (magnification,
×400). (E) MCC with diffusely-positive staining for chromogranin
(magnification, ×400). (F) Positive staining for cytokeratin
(CK)20, with a perinuclear dot-like pattern, supporting the
diagnosis of MCC (magnification, ×400). (G) Positive staining for
CK8/18, with a perinuclear dot-like pattern (magnification, ×400).
(H) MCC with diffusely-positive staining for epithelial membrane
antigen (magnification, ×400). |
Discussion
MCC was first described by Toker (5) in 1972 and is believed to be a rare
skin carcinoma of neuroendocrine origin. Fair skin shows a clear
predilection for MCC, representing nearly 95% of the total number
of cases. MCC is less commonly described in the skin types of
patients of Asian, Native American or African descent (6). Epidemiology and End Results (SEER)
from 1973 to 2006, 94.9 % of patients were Caucasioan,
African-Americans represented only 1% of patients (7). However, the histogenesis of MCC
remains controversial. The most commonly accepted hypothesis is
that the tumor arises from a neural crest-derived cell, which is
considered to be the Merkel cells (8). However, recent observations have
challenged this concept and put forward a pluripotent cutaneous
stem cell origin (9). MCC is a
challenging and aggressive disease, with high mortality and
associations with Merkel cell polyomavirus and immunosuppression.
Even after radical surgery, it easily relapses in situ,
invades the regional lymph nodes and metastasizes to distant skin,
liver, bones and lungs, and more rarely to organs such as the
pancreas (3,10).
Due to the nondescript clinical features of MCC, the
diagnosis in the majority of cases relies upon the pathological
examination. Microscopically, MCCs frequently originate in the
dermis and mostly invade the lymphatic capillaries of subcutaneous
adipose tissue; <10% of cases have a tendency to spread into the
epidermis and may even generate micro-abscesses (11). Histologically, the tumor is composed
of small, round to oval-shaped, basophilic cells that are uniform
in size, with little cytoplasm, vesicular nuclei, finely granular
dispersed chromatin, distinct nuclear membranes and multiple small
nucleoli. Numerous mitotic figures and apoptotic bodies are usually
present. Additionally, certain MCC cases present with increased
vascularity, which is significant as increased vascular
proliferation is associated with a worse prognosis, as are
lymphovascular invasion, a small cell size and a high mitotic
rate.
According to the varying pathological morphology,
MCC can be histologically divided into three subtypes: The
trabecular, intermediate cell and small cell types. There does not
appear to be any prognostic differences associated with these
subtypes. The rare trabecular type displays uniform cells with
characteristic parallel alignment and Zellballen architecture.
Cytology shows vesicular nuclei and inconspicuous nucleoli. The
intermediate cell variant is observed most commonly in MCC and
displays a solid, diffuse growth pattern made up of closely packed
cells that are shaped like lymphocytes. Mitoses and nuclear
fragmentation are noted frequently in tumor cells in this
particular pattern. The tumor cells of the small cell type are
characterized by deeply stained ‘oat cells’ and possess obvious
nuclei, scant cytoplasm, spotty necrosis and nuclear debris. Mixed
and transitional forms of the three types are often present
(12,13).
Upon immunohistochemical analysis, the tumor cells
of MCC are labeled with neuroendocrine markers (CgA, Syn and NSE)
and epithelial markers such as CK20 and CK8/18, which may show a
characteristic perinuclear-dot pattern. This feature is routinely
used to assist in diagnosing MCC. Indeed, a previous study recorded
that 87% of 191 MCC cases were positive for CK20 (14). Thus, the lack of a characteristic
stain for CK20 does not exclude the diagnosis of MCC. Several
studies have also found CD117 and CD99 positivity in cases of MCC,
and CD44-positive cases may correlate with the high risk of tumor
metastasis (15,16). In order to form a differential
diagnosis in the present study, these tests were combined with
staining for LCA, Vim, TTF-1, HMB45, Malen-A and S-100, which are
usually negative in the majority of MCC.
In the majority of cases, the diagnosis of MCC can
be challenging due the uncharacteristic histomorphological cellular
features of MCC and the extensive list of differential diagnoses.
Immunohistochemical staining plays a crucial role in the
differential diagnosis of these tumors. Characteristic
immunohistochemical staining of MCC and other small, round, blue
cell tumors is compared in Table I.
Lymphoma is a critical differential diagnosis of MCC. The tumor
cells of lymphoma have a diffuse growth pattern with plentiful
cytoplasm, often infiltrating into the epidermis. The presence of
irregular nuclear membranes is usually typical of lymphomas,
whereas the nuclear contours in MCC are usually smooth and rounded.
Specific expression patterns of LCA in malignant lymphoma can aid
in establishing a definitive diagnosis (17). Similar to the small cell type of
MCC, the tumor cells of metastatic SCLC are small with deeply
stained nuclei. It should be noted that neuroendocrine markers are
not specific for MCC, as they can also be positively expressed in
metastatic SCLC. When the distinction is problematic, positive
staining for TTF-1 and CK7 and negative staining for CK20 in
metastatic SCLC offer the greatest sensitivity and specificity,
however, CK20 may be positive in 3% of the SCLC, which should be
taken into consideration (18). The
conventional, reliable, morphological feature of tumor cells being
pleomorphic and often involving the epidermis can be of aid in
distinguishing non-pigmented malignant melanoma from MCC. When in
doubt, the immunohistochemical stains of Malen-A, HMB45 and S-100,
which are expressed in the majority of malignant melanomas, provide
valuable evidence (19). In
primitive neuroectodermal tumors (PNETs), characteristic
rosette-like structures can be observed, and the central lumen are
filled with hyperplastic fibrils. The common expression of CD99 in
PNET and CK20 in MCC suggests these markers may be valuable in the
diagnostic setting (20). Other
small cell cutaneous carcinomas, such as primary
poorly-differentiated squamous carcinoma of the skin, can also be
confused with MCC in terms of the morphological features. Only
epithelial markers, including CEA and EMA, can be used in the
staining of the tumor cytoplasm of squamous carcinoma. Occasionally
squamous carcinoma can occur concurrently with MCC, however, MCC
has a poorer prognosis.
 | Table IImmunohistochemical staining markers
of small, round, blue cells in the skin. |
Table I
Immunohistochemical staining markers
of small, round, blue cells in the skin.
| Cancer type | CK20 | CEA | EMA | CgA | Syn | NSE | TTF-1 | Melan-A | HMB45 | S-100 | CD56 | CD99 | LCA |
|---|
| Merkel cell
carcinoma | +/− | − | + | +/− | +/− | + | − | − | − | − | + | −/+ | − |
| Small cell lung
cancer | −/+ | + | − | +/− | +/− | + | +/− | − | − | − | + | − | − |
| Malignant
melanoma | − | − | − | − | − | − | − | + | + | + | −/+ | −/+ | − |
| Lymphoma | − | − | − | − | − | − | − | − | − | − | − | − | + |
| PNET | − | − | − | + | + | + | − | − | − | +/− | − | + | − |
| Squamous
carcinoma | − | + | + | − | − | − | − | − | − | − | − | − | − |
In conclusion, MCC occurring on sites not exposed to
the sun, such as the inguinal region, is rare. Due to the low
incidence rate and lack of characteristic clinical manifestations,
MCC is often misdiagnosed. The final diagnosis relies on the
analysis of histological findings and immunohistochemical markers
following lesion biopsy or resection.
References
|
1
|
Smith DF, Messina JL, Perrott R, et al:
Clinical approach to neuroendocrine carcinoma of the skin (Merkel
cell carcinoma). Cancer Control. 7:72–83. 2000.PubMed/NCBI
|
|
2
|
Haag ML, Glass LF and Fenske NA: Merkel
cell carcinoma. Diagnosis and treatment. Dermatol Surg. 21:669–683.
1995. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Poulsen M: Merkel-cell carcinoma of the
skin. Lancet Oncol. 5:593–599. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Song PI, Liang H, Wei WQ, Jiang YQ, Smith
JS and Qiao YL: The clinical profile of Merkel cell carcinoma in
mainland China. Int J Dermatol. 51:1054–1059. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Toker C: Trabecular carcinoma of the skin.
Arch Dermatol. 105:107–110. 1972. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Swann MH and Yoon J: Merkel cell
carcinoma. Semin Oncol. 34:51–56. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hughes MP, Hardee ME, Cornelius LA, et al:
Merkel Cell Carcinoma: Epidemiology, Target, and Therapy. Curr
Dermatol Rep. 3:46–53. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bickle K, Glass LF, Messina JL, Fenske NA
and Siegrist K: Merkel cell carcinoma: a clinical, histopathologic,
and immunohistochemical review. Semin Cutan Med Surg. 23:46–53.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Morrison KM, Miesegaes GR, Lumpkin EA and
Maricich SM: Mammalian Merkel cells are descended from the
epidermal lineage. Dev Biol. 336:76–83. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ouellette JR, Woodyard L, Toth L and
Termuhlen PM: Merkel cell carcinoma metastatic to the head of the
pancreas. JOP. 5:92–96. 2004.PubMed/NCBI
|
|
11
|
Smith KJ, Skelton HG III, Holland TT,
Morgan AM and Lupton GP: Neuroendocrine (Merkel cell) carcinoma
with an intraepidermal component. Am J Dermatopathol. 15:528–533.
1993. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Skelton HG, Smith KJ, Hitchcock CL,
McCarthy WF, Lupton GP and Graham JH: Merkel cell carcinoma:
analysis of clinical, histologic, and immunohistologic features of
132 cases with relation to survival. J Am Acad Dermatol.
37:734–739. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Schrama D and Becker JC: Merkel cell
carcinoma - pathogenesis, clinical aspects and treatment. J Eur
Acad Dermatol Venereol. 25:1121–1129. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Bobos M, Hytiroglou P, Kostopoulos I,
Karkavelas G and Papadimitriou CS: Immunohistochemical distinction
between merkel cell carcinoma and small cell carcinoma of the lung.
Am J Dermatopathol. 28:99–104. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Llombart B, Monteagudo C, López-Guerrero
JA, et al: Clinicopathological and immunohistochemical analysis of
20 cases of Merkel cell carcinoma in search of prognostic markers.
Histopathology. 46:622–634. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Penneys NS and Shapiro S: CD44 expression
in Merkel cell carcinoma may correlate with risk of metastasis. J
Cutan Pathol. 21:22–26. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Burke JS, Hoppe RT, Cibull ML and Dorfman
RF: Cutaneous malignant lymphoma: a pathologic study of 50 cases
with clinical analysis of 37. Cancer. 47:300–310. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Byrd-Gloster AL, Khoor A, Glass LF, et al:
Differential expression of thyroid transcription factor 1 in small
cell lung carcinoma and Merkel cell tumor. Hum Pathol. 31:58–62.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kontochristopoulos GJ, Stavropoulos PG,
Krasagakis K, Goerdt S and Zouboulis CC: Differentiation between
merkel cell carcinoma and malignant melanoma: An
immunohistochemical study. Dermatology. 201:123–126. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Nicholson SA, McDermott MB, Swanson PE and
Wick MR: CD99 and cytokeratin-20 in small-cell and basaloid tumors
of the skin. Appl Immunohistochem Mol Morphol. 8:37–41. 2000.
View Article : Google Scholar : PubMed/NCBI
|














