Introduction
Chronic myeloid leukemia (CML) is a
myeloproliferative disorder that is associated with a unique
translocation of chromosomes 9 and 22, resulting in the so-called
Philadelphia chromosome (Ph). This in turn results in the formation
of a fusion protein product, BCR-ABL, which plays a key role in the
pathogenesis of CML. Imatinib is the first-generation tyrosine
kinase inhibitor (TKI) of BCR-ABL and is approved to treat
Ph-positive (Ph+) leukemia (1). Although the drug is highly active, it
is noteworthy that 30–35% of patients do not have an optimal
response due to treatment interruptions resulting from intolerance
to the adverse effects (2).
Up to 20% of patients who have imatinib-treated CML
in blast crisis (BC) or Ph+ acute leukemia experience a
relapse in the central nervous system (CNS) (3,4). This
is a challenging issue in the imatinib era, and is due to the poor
penetration of the drug by the blood-brain barrier (BBB) (4–10).
Dasatinib and nilotinib, the second-generation TKIs, lead to a
complete cytogenetic response (CyR) in ~50% of imatinib-resistant
patients and to major molecular remission in 20–30% (11,12).
Furthermore, the two TKIs have demonstrated hematological and
molecular responses higher than those of imatinib, and are approved
for first-line treatment of newly diagnosed CML in the chronic
phase (CP) (13,14). At least one previous study has
suggested that dasatinib crosses the BBB and is effective for CNS
Ph+ leukemia (15).
However, other studies have reported conflicting findings (16–21).
The present study reports a successful experience of using
dasatinib-based combination therapy to treat CNS involvement in a
22-year-old female with CML in BC. Written informed consent was
obtained from the patient’s family.
Case report
A 22-year-old female was diagnosed with CML in CP at
Tri-Service General Hospital (Taipei, Taiwan) in November 2008 and
was treated with imatinib 400 mg daily. The patient showed poor
compliance with frequent drug interruptions, and the best response
during treatment was a major CyR. In October 2012, approximately
four years after the initiation of therapy, the patient experienced
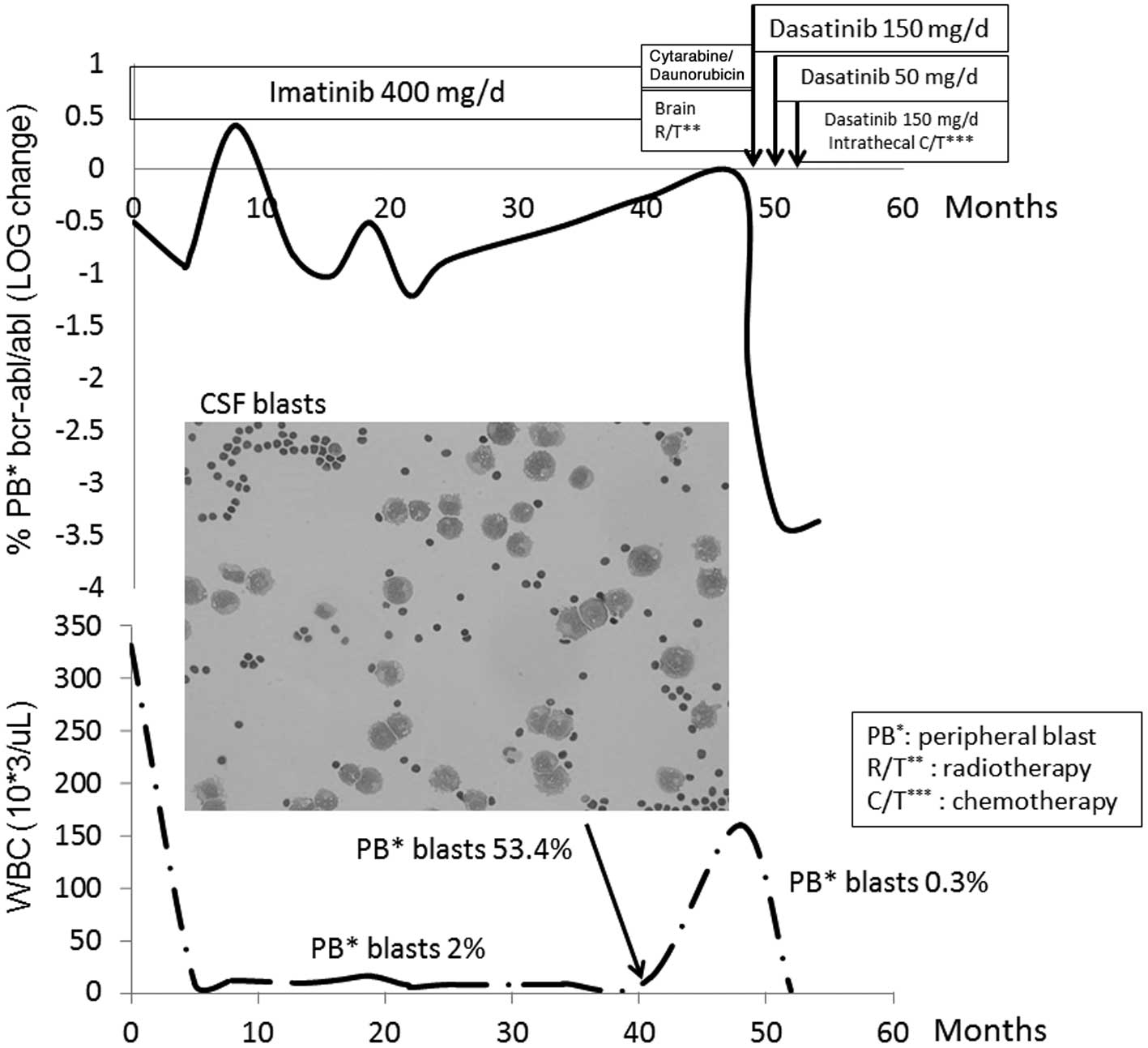
a new onset of intermittent fever and easy bruising. Laboratory
testing revealed marked leukocytosis, with a white blood cell (WBC)
count of 330,000 μl (normal range, 4,500–11,000 μl) and excessive
peripheral myeloblasts (53.4%; normal range, 0–1%). A subsequent
bone marrow (BM) biopsy revealed 60% myeloblasts (normal range,
0.3–5%), and a diagnosis of CML in BC was made. No mutation was
detected in the leukemic BCR-ABL transcripts. The patient received
induction chemotherapy with seven days of 160 mg cytarabine (100
mg/m2) and three days of 100 mg daunorubicin (60
mg/m2). A repeat BM examination revealed partial
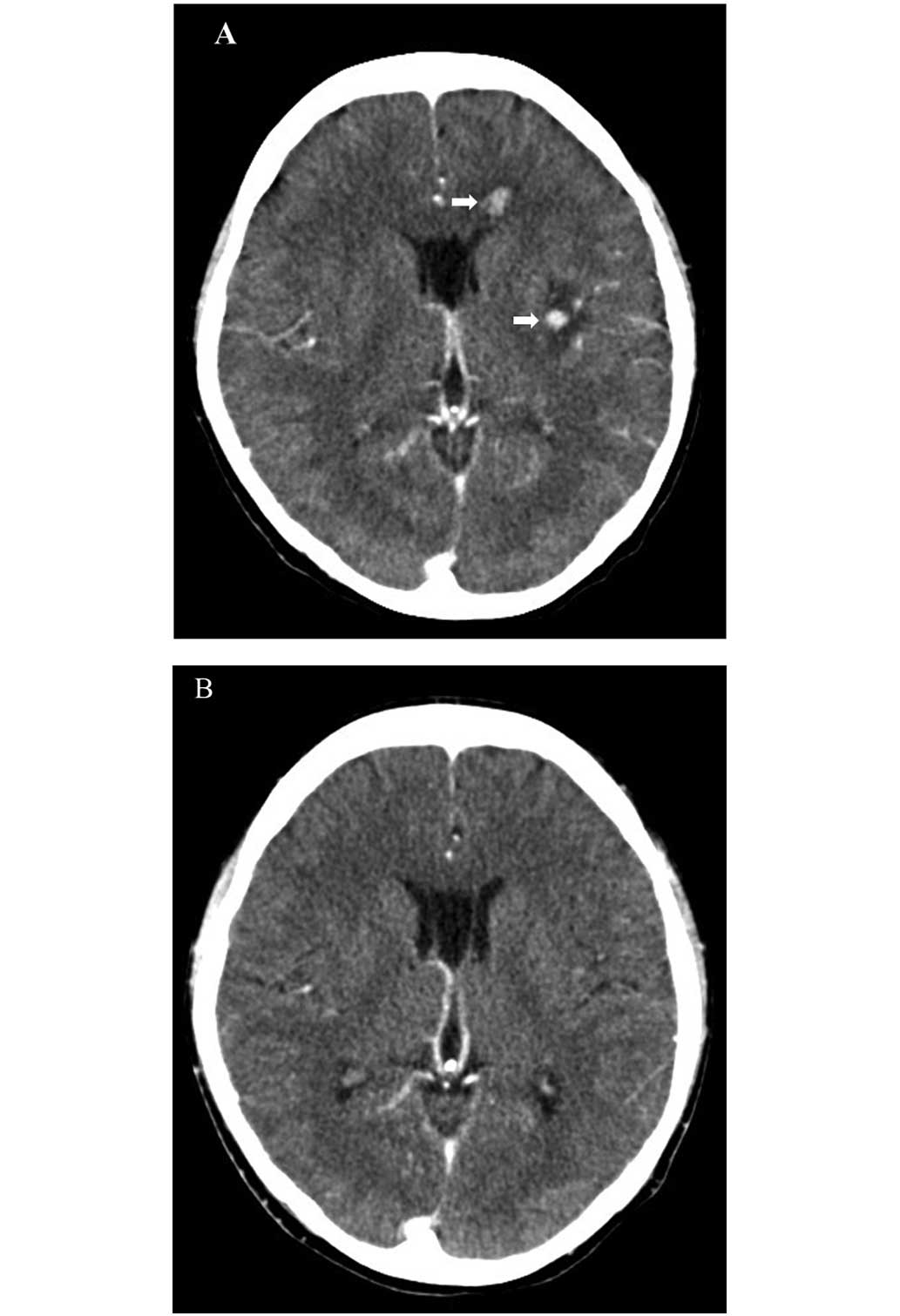
remission after two weeks. Due to a new onset of left facial
numbness, the patient underwent a computed tomography (CT) scan of
the brain, which revealed multiple small enhancing nodules
(Fig. 1A). Cerebrospinal fluid
(CSF) examination revealed myeloperoxidase-positive blasts.
Due to a poor Eastern Cooperative Oncology Group
performance status of 3, it was decided not to treat the patient
with aggressive systemic or intrathecal therapy at that time.
Instead, the patient was treated with 50 mg dasatinib three times a
day in combination with whole brain radiotherapy (total, 3,000
cGy). A repeat CT scan revealed near-complete resolution of the
brain lesions (Fig. 1B). A repeat
BM examination also revealed complete remission. During the
treatment, only grade 1 hematological toxicities were noted. The
patient was subsequently discharged and kept on the same dose of
dasatinib.
One month later, the patient developed intermittent
vomiting and a fever. Laboratory testing revealed pancytopenia,
with a WBC count of 2,590 μl (normal range, 4,500–11,000 μl), a
hemoglobin concentration of 8.4 g/dl (normal range, 11.3–15.3 g/dl)
and a platelet count of 109,000 μl (normal range, 150,000–400,000
μl). Since subsequent investigation did not reveal any notable
cause, this was suspected to be due to the dasatinib treatment and
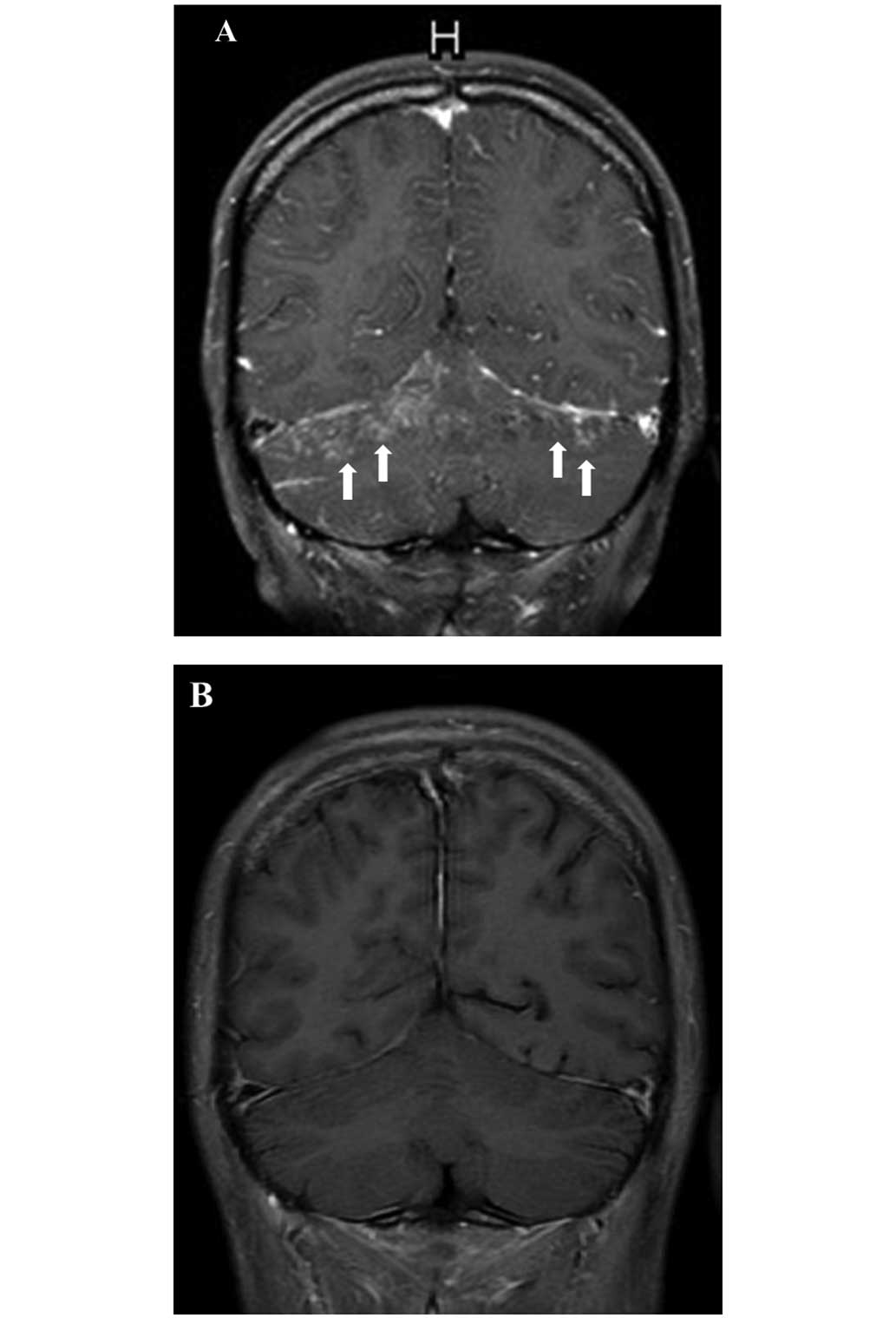
so the dose was reduced. The next week, three days after the dose
reduction of dasatinib, the patient experienced a generalized
tonic-clonic seizure. Magnetic resonance imaging (MRI) of the brain
revealed diffuse leptomeningeal enhancement (Fig. 2A). The patient became rapidly
obtunded and required intubation for ventilator support. Following
weekly intrathecal chemotherapy [methotrexate (12 mg), cytarabine
(100 mg) and hydrocortisone (50 mg)] for five courses, in
combination with 50 mg dasatinib three times daily, the patient’s
clinical condition gradually improved. Subsequently, the patient
was successfully weaned off the ventilator and discharged.
Furthermore, a repeat brain MRI revealed significant regression of
the brain lesions (Fig. 2B). Grade
3 hematological toxicities were noted during the treatment. Two
weeks after being discharged, the patient experienced confusion and
generalized weakness. A brain MRI revealed diffuse
leukoencephalopathy, but there was no evidence of CNS relapse on a
repeat CSF examination. The patient was admitted to the hospital,
but succumbed to pneumonia with profound sepsis two weeks after
admission. The entire treatment course in correlation with BCR-ABL
transcript levels is shown in Fig.
3.
Discussion
Acute leukemia with CNS involvement is not uncommon
in clinical practice. Intrathecal chemotherapy, high-dose
chemotherapy and radiotherapy are conventional treatments for CNS
leukemia. However, a poor quality of life, significant systemic or
CNS toxicity, a short response duration and ultimately mortality
associated with refractory leukemia are common outcomes in a number
of patients (22).
Imatinib is a substrate for the drug-eluting
P-glycoprotein, which results in suboptimal penetration into the
CNS, and the CSF levels of imatinib are 100-fold less than those
achieved in plasma (6–8). This may explain why patients have CNS
relapse in spite of achieving a complete response in the peripheral
blood and BM. Dasatinib has greater potency (325-fold) than
imatinib and can be therapeutically effective at a low or even
subnanomolar concentration (23,24). A
study by Porkka et al demonstrated that dasatinib is
associated with substantial clinical responses in patients with CNS
leukemia and could significantly increase survival and control
intracranial tumors in vivo (15). In addition to the present study,
four separate case reports in Table
I further support the potential benefit of dasatinib in
Ph+ CNS leukemia (16–19).
In these four cases, the majority of patients received dasatinib
combination therapies and all patients were administered ≥140 mg
dasatinib, daily (16–19). Nishimoto et al reported that
dasatinib maintenance following allogeneic hematopoietic stem cell
transplantation has the potential to prevent CNS relapse (18). In spite of these encouraging
studies, it is sobering that several patients have progressive
disease within months of starting therapy. Notably, Papageorgiou
et al reported one case of Ph+ acute
megakaryoblastic leukemia who received 140 mg dasatinib daily and
maintained stable disease for 16 months, however, the patient
experienced CNS relapse following treatment with a de-escalated
daily dose of 70 mg daily due to pleural effusion (20). Frigeri et al also presented a
case of Ph+ CNS leukemia in which dasatinib failed to
prevent CNS progression. However, this patient was administered
<100 mg dasatinib daily during the treatment course (21).
 | Table IDA combination therapies for
PH+ CNS leukemia. |
Table I
DA combination therapies for
PH+ CNS leukemia.
| Ref. | Patient | BCR/ABL mutation | Prior HSCT | Combination
therapies | DA dosage,
mg/day | DA duration after CNS
leukemia | Best CNS
response | Alive | Treatment and
outcome |
|---|
| 16 | Ph+
ALa | T315I | Yes | IT | 140 | 52 days | PR | No | 200 mg/day since day
37; succumbed to disease progression. |
| 17 | BC-CML | T315Ib | No | IT | 140 | 4 months | CR | Yes | Awaiting HSCT |
| 18 | BC-CML | NR | No | RT, IT | 140 | 38+ months | CR | Yes | Post-HSCT DA
maintenance; leukoencephalopathy |
| 19 | Ph+
ALL | NR | Yes | RT, IT | 140 | 12 months | CR | Yes | |
| 20 | Ph+
AML | No | No | No | 70 | 7 months | PD | No | Initially 140 mg/day,
16 months, then 70 mg/day, 7 months, due to pleural effusion;
succumbed to CNS relapse |
| 21 | BC-CML | No | Yes | IT | 100 | 4 months | PD | No | Succumbed to CNS
relapse |
| Present case | BC-CML | No | No | RT, IT | 150 | 6 months | CR | No | Leukoencephalopathy;
succumbed to pneumonia with sepsis |
While disease biology may play a significant role,
it is vital to investigate whether other factors may be involved.
One possibility may be the loss of CNS disease control with the
lowering of the dasatinib dose. Indeed, it appears that among the
cases reported in the literature, outcomes are poor when the dose
is <140 mg a day (15–21). The most common reasons for
decreasing the dose of dasatinib are adverse events, including
cytopenia or pleural effusion (25). This was also observed in the patient
in the present study, where progressive neurological deterioration
occurred shortly after dasatinib dose reduction and a marked
improvement was noted following re-escalation to 150 mg once daily
(Fig. 2). Although the overall
experience with this issue is limited to the small number of cases
in the literature, we believe that the available anecdotal data
point to a requirement for a sufficient dose intensity of dasatinib
for improved outcomes.
In conclusion, dasatinib may be a viable option for
the management of patients with Ph+ CNS leukemia,
including those who are not medically fit for or are otherwise
unwilling to receive high-dose chemotherapy. It appears that dose
intensity is essential for optimal efficacy and should possibly be
maintained at 150 mg daily as far as possible. A well-designed,
prospective study will aid in further clarifying this issue and
better defining the role of dasatinib in this setting.
Acknowledgements
The authors would like to thank Dr Vivek R. Sharma,
Division of Medical Oncology/Hematology, University of Louisville,
School of Medicine (Louisville, KY, USA), for providing a critical
review and comments on the manuscript.
References
|
1
|
Schiffer CA: BCR-ABl tyrosine kinase
inhibitors for chronic myelogenous leukemia. N Engl J Med.
357:258–265. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Carella AM, Branford S, Deininger M, et
al: What challenges remain in chronic myeloid leukemia research?
Haematologica. 98:1168–1172. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Pfeifer H, Wassmann B, Hofmann WK, et al:
Risk and prognosis of central nervous system leukemia in patients
with Philadelphia chromosome-positive acute leukemias treated with
imatinib mesylate. Clin Cancer Res. 9:4674–4681. 2003.PubMed/NCBI
|
|
4
|
Leis JF, Stepan DE, Curtin PT, et al:
Central nervous system failure in patients with chronic myelogenous
leukemia lymphoid blast crisis and Philadelphia chromosome positive
acute lymphoblastic leukemia treated with imatinib (STI-571). Leuk
Lymphoma. 45:695–698. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wolff NC, Richardson JA, Egorin M and
Ilaria RL Jr: The CNS is a sanctuary for leukemic cells in mice
receiving imatinib mesylate for Bcr/Abl-induced leukemia. Blood.
101:5010–5013. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Petzer AL, Gunsilius E, Hayes M, et al:
Low concentrations of STI571 in the cerebrospinal fluid: a case
report. Br J Haematol. 117:623–625. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bornhauser M, Jenke A, Freiberg-Richter J,
et al: CNS blast crisis of chronic myelogenous leukemia in a
patient with a major cytogenetic response in bone marrow associated
with low levels of imatinib mesylate and its N-desmethylated
metabolite in cerebral spinal fluid. Ann Hematol. 83:401–402. 2004.
View Article : Google Scholar
|
|
8
|
Dai H, Marbach P, Lemaire M, Hayes M and
Elmquist WF: Distribution of STI-571 to the brain is limited by
p-glycoprotein-mediated efflux. J Pharmacol Exp Ther.
304:1085–1092. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bujassoum S, Rifkind J and Lipton JH:
Isolated central nervous system relapse in lymphoid blast crisis
chronic myeloid leukemia and acute lymphoblastic leukemia in
patients on imatinib therapy. Leuk Lymphoma. 45:401–403. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Isobe Y, Sugimoto K, Masuda A, Hamano Y
and Oshimi K: Central nervous system is a sanctuary site for
chronic myelogenous leukaemia treated with imatinib mesylate.
Intern Med J. 39:408–411. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hochhaus A, Kantarjian HM, Baccarani M, et
al: Dasatinib induces notable hematologic and cytogenetic responses
in chronic-phase chronic myeloid leukemia after failure of imatinib
therapy. Blood. 109:2303–2309. 2007. View Article : Google Scholar
|
|
12
|
Kantarjian HM, Giles F, Gattermann N, et
al: Nilotinib (formerly AMN107), a highly selective BCR-ABL
tyrosine kinase inhibitor, is effective in patients with
Philadelphia chromosome-positive chronic myelogenous leukemia in
chronic phase following imatinib resistance and intolerance. Blood.
110:3540–3546. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kantarjian H, Shah NP, Hochhaus A, et al:
Dasatinib versus imatinib in newly diagnosed chronic-phase chronic
myeloid leukemia. N Engl J Med. 362:2260–2270. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Saglio G, Kim DW, Issaragrisil S, et al:
Nilotinib versus imatinib for newly diagnosed chronic myeloid
leukemia. N Engl J Med. 362:2251–2259. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Porkka K, Koskenvesa P, Lundan T, et al:
Dasatinib crosses the blood-brain barrier and is an efficient
therapy for central nervous system Philadelphia chromosome-positive
leukemia. Blood. 112:1005–1012. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Abdelhalim A, Barcos M, Block AW, et al:
Remission of Philadelphia chromosome-positive central nervous
system leukemia after dasatinib therapy. Leuk Lymphoma.
48:1053–1056. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Alimena G, Breccia M, Latagliata R, et al:
Dasatinib in the management of lymphoid blast crisis of
Philadelphia-positive chronic myeloid leukemia with multiple
extra-medullary and intracranial localizations. Leuk Res.
33:e134–e136. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Nishimoto M, Nakamae H, Koh KR, et al:
Dasatinib maintenance therapy after allogeneic hematopoietic stem
cell transplantation for an isolated central nervous system blast
crisis in chronic myelogenous leukemia. Acta Haematol. 130:111–114.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Gutierrez-Aguirre H, Garcia-Rodriguez F,
Cantu-Rodriguez O, Gonzalez-Llano O, Jaime-Perez J and
Gomez-Almaguer D: Effectiveness of dasatinib in relapsed CNS, Ph+
ALL that is refractory to radiochemotherapy plus imatinib: a case
report. Clin Adv Hematol Oncol. 9:875–878. 2011.
|
|
20
|
Papageorgiou SG, Pappa V, Economopoulou C,
et al: Dasatinib induces long-term remission in imatinib-resistant
Philadelphia chromosome-positive acute megakaryoblastic leukemia
but fails to prevent development of central nervous system
progression. Leuk Res. 34:e254–e256. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Frigeri F, Arcamone M, Luciano L, Di
Francia R, Pane F and Pinto A: Systemic dasatinib fails to prevent
development of central nervous system progression in a patient with
BCR-ABL unmutated Philadelphia chromosome-positive leukemia. Blood.
113:5028–5029. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Cortes J: Central nervous system
involvement in adult acute lymphocytic leukemia. Hematol Oncol Clin
North Am. 15:145–162. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
O’Hare T, Walters DK, Stoffregen EP, et
al: In vitro activity of Bcr-Abl inhibitors AMN107 and BMS-354825
against clinically relevant imatinib-resistant Abl kinase domain
mutants. Cancer Res. 65:4500–4505. 2005. View Article : Google Scholar
|
|
24
|
Shah NP, Tran C, Lee FY, Chen P, Norris D
and Sawyers CL: Overriding imatinib resistance with a novel ABL
kinase inhibitor. Science. 305:399–401. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
McCormack PL and Keam SJ: Dasatinib: a
review of its use in the treatment of chronic myeloid leukaemia and
Philadelphia chromosome-positive acute lymphoblastic leukaemia.
Drugs. 71:1771–1795. 2011. View Article : Google Scholar : PubMed/NCBI
|