Introduction
Epithelioid hemangioendothelioma (EH) is a rare
vasoformative tumor of intermediate-grade malignancy with a
clinical course between hemangioma and angiosarcoma in terms of
frequent local recurrences and metastatic potential (1). The tumor may occur in the soft tissues,
liver, lungs and bone, as well as numerous other locations
(2–5).
EH occurs less commonly in bone, accounting for
<1% of all primary bone tumors. Mainly located in the long
tubular bones of the lower extremities and pelvis, the tumor is
rarely found in the upper extremities and flat bones (5–9).
Therefore, the formation of a definitive diagnosis of EH is
difficult and the tumor is easily misdiagnosed. Furthermore, the
prognosis and treatment of EH remains controversial. The current
study presents a rare case of multicentric EH of the right head of
the humerus, scapula, ipsilateral distal femur and proximal tibia
with visceral involvement of the lung, which was previously
misdiagnosed as multiple chondroblastoma of the right distal femur
and proximal tibia with low malignant potential. However, the
diagnosis of EH was confirmed post-operatively by radiological and
histopathological examination. Written informed consent was
obtained from the patient.
Case report
In December 2012, a 20-year-old male patient
presented to the orthopedics clinic at the Second Affiliated
Hospital, School of Medicine, Zhejiang University (Zhejiang, China)
with an increasing degree of pain in the right knee that had been
apparent for eight months, predominantly whilst walking. The
patient had no history of trauma or infection. Physical examination
was normal, with the exception of the right knee, which was
slightly enlarged, however, no soft-tissue swelling was
identified.
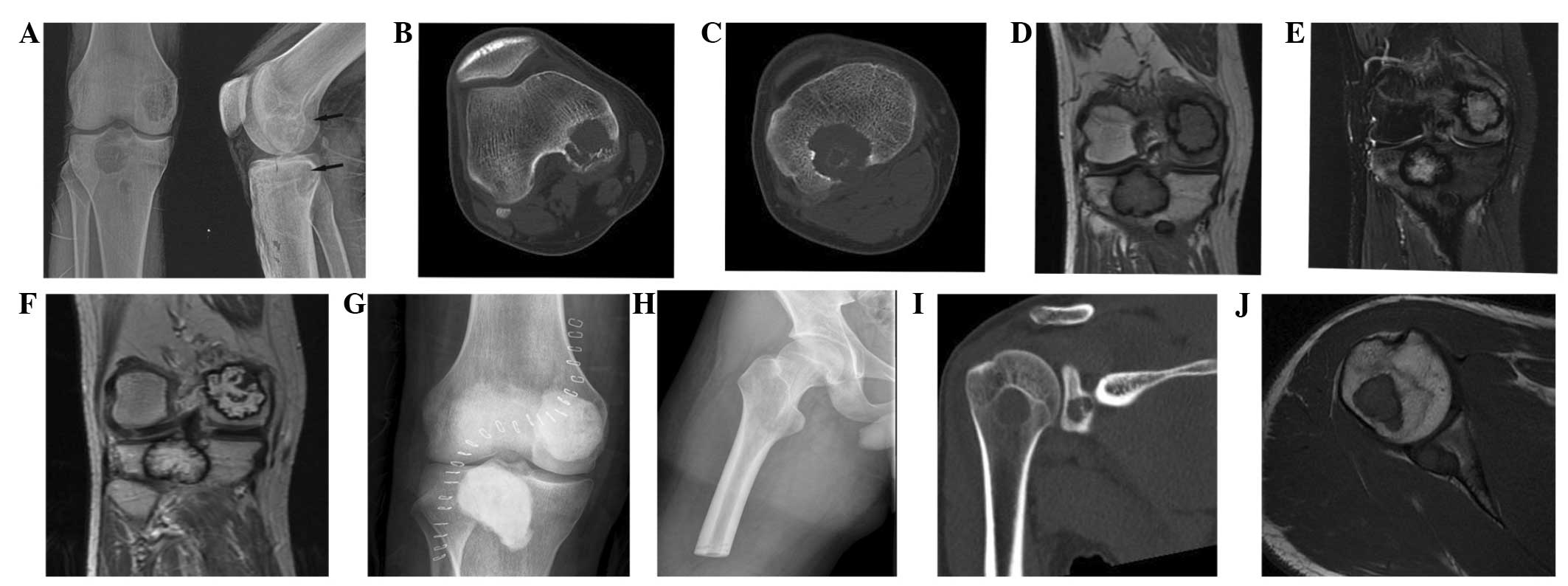
As shown in Fig. 1A,
plain radiography of the right knee revealed multiple large, lytic
lesions with ill-defined margins in the medial femoral condyle and
proximal tibia. Cortical destruction without periosteal reaction
was also identified. However, no lesions of the chest were
indicated on plain radiography.
Bone scintigraphy showed increased radionuclide
uptake in the right medial femoral condyle and proximal tibia
(Fig. 2). Slightly increased uptake
in the right head of the humerus was also identified. However, no
clinical symptoms, such as pain or swelling, were observed.
Non-enhanced computed tomography (CT) revealed
multifocal eccentric lytic lesions in the medial femoral condyle
and proximal tibia, with involvement of the medullar cavity and
cortex (Fig. 1B and C).
Magnetic resonance imaging (MRI) of the right knee
revealed multiple, large, irregular, nodular masses with
intermediate intensity on T1-weighted images (Fig. 1D) and high signal intensity on
T2-weighted images (Fig. 1E). The
injection of gadolinium contrast material resulted in a high
contrast enhancement and peripheral low signal intensity in all
pulse sequences (Fig. 1F). The
largest lesion in the proximal tibia was similar in size to that
identified in the medial femoral condyle, which was ~3.5 cm in
diameter. The masses were considered to arise from the medullary
cavity, with destruction of the proximal cortex and extension into
the adjacent soft tissue. The large lesions in the proximal tibia
and medial femoral condyle were in close proximity to the articular
surface, with a thin residual line of cortex. Furthermore, an
edematous bone reaction was observed, which surrounded the
lesions.
Initially, based on the radiological examination,
the patient was diagnosed with multiple chondroblastoma of the
right distal femur and proximal tibia, with low malignant
potential. An extra-articular curettage of the lesions in the
proximal tibia was performed and the medial femoral condyle was
filled with bone cement (Fig.
1G).
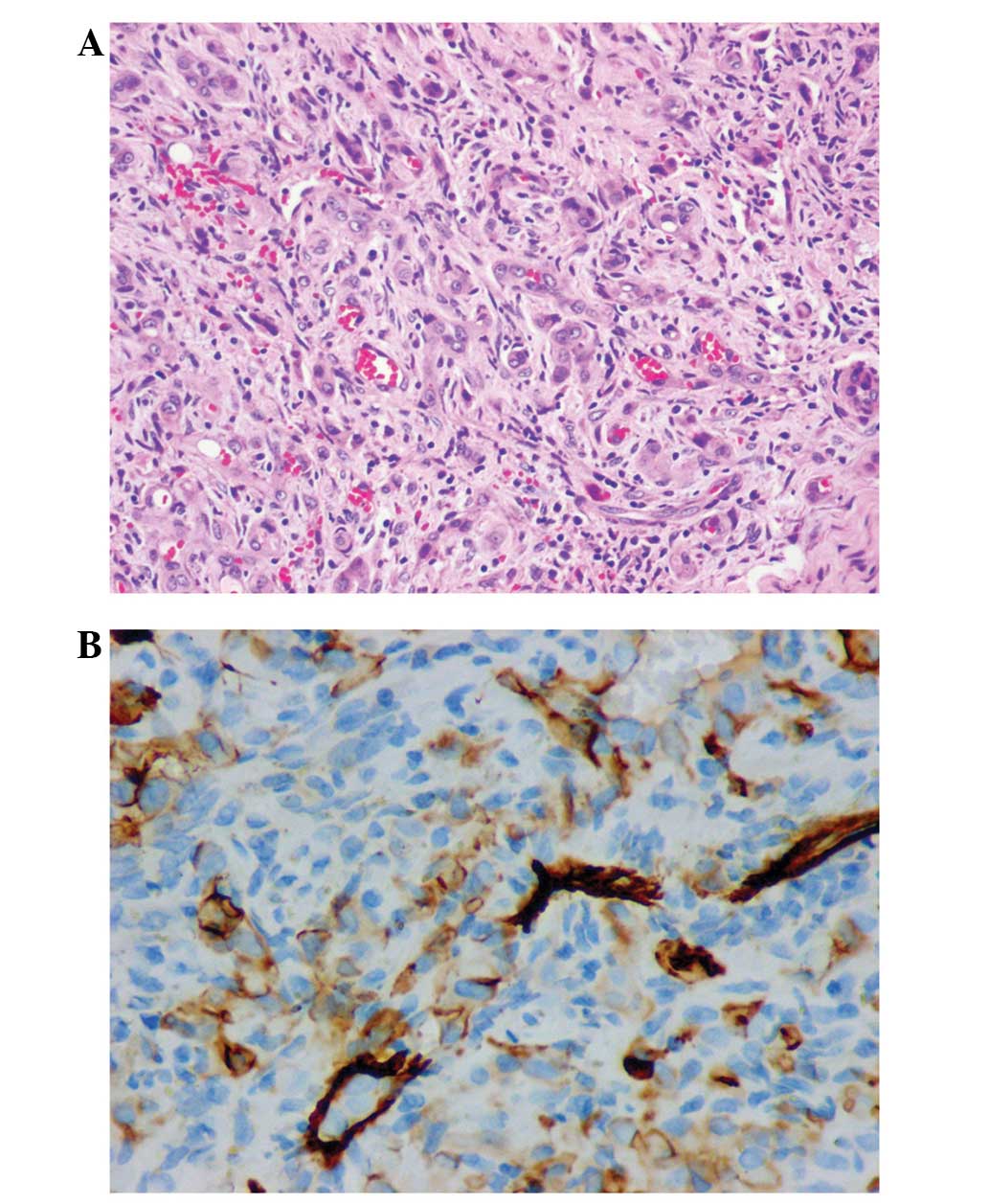
However, following pathological examination, the
tumor was diagnosed as an EH. Histopathological examination
revealed that the tumor tissue was composed of solid nests and
anastomosing cords of epithelioid cells with a moderate quantity of
eosinophilic cytoplasm. The cells were variably spindle-shaped and
epithelioid, with a number of intracytoplasmic vacuoles (Fig. 3A). The presence of intracytoplasmic
vacuoles containing erythrocytes was considered as evidence of
primitive vascular differentiation. In addition, rare mitotic
figures and mild pleomorphism were identified. Immunohistochemistry
revealed that the tumor cells were positive for vascular and
stromal markers [cluster of differentiation (CD)34 (Fig. 3B), CD31 and vimentin] and negative for
epithelial cytokeratin markers [epithelial membrane antigen (EMA)
and AE1/AE3]. Following the diagnosis of EH based on the results of
curettage, the patient underwent an amputation of the right leg at
thigh level (Fig. 1H).
Following this second surgical procedure, whole-body
MRI and CT scans were performed. As shown in Figs. 1I and J, multiple lytic lesions were
identified in the right head of the humerus and scapula.
Furthermore, CT scans of the chest and abdomen revealed pulmonary
metastases. After consultation with orthopedic surgeons and
radiotherapists, the patient underwent radiotherapy of the right
head of the humerus and scapula, but refused chemotherapy. After
the completion of radiotherapy treatment, monthly follow-up
clinical examinations were performed for one year. Subsequently,
follow-up telephone examinations were conducted every two months,
which are ongoing. At the time of writing this manuscript, at 15
months post-surgery, the patient remains alive.
Discussion
EH is an intermediate-grade malignant vascular
neoplasm, with a clinical course between those of epithelioid
hemangioma and angiosarcoma (1). The
first case of EH in the soft tissues was reported by Weiss and
Enzinger in 1982 (10). Since then, a
number of cases of EH have been reported in other locations,
including the liver, lungs and bone. EH most commonly occurs in
individuals between 20 and 30 years of age. EH of the bone is rare,
with lesions distributed throughout the skeleton. Bone EH has a
predilection for involvement of the axial skeleton and long tubular
bones. Osseous EH may be observed as multifocal or multicentric
lesions in a single bone or multiple bones; it predominantly occurs
in the lower extremities and the pelvis, affecting the upper
extremities, vertebrae and other flat bones less frequently.
Simultaneous occurrence in the upper and lower extremities, as
observed in the present case, is extremely rare (5–9,11). An extensive literature search of
PubMed using the search terms, ‘epithelioid hemangioendothelioma’
‘bone’, ‘multicentric’ and ‘multifocal’ revealed only one report of
bone EH occurrence in the upper and lower extremities
simultaneously. Boutin et al (5) reported a case involving several lesions,
which were identified in the proximal and distal phalanges of the
great toe, first metatarsal, medial cuneiform, tarsal navicular, C2
and C3 vertebral body, clavicle, scapulae and ilium. Due to the
lack of literature regarding the simultaneous occurrence of bone EH
in the upper and lower extremities, in the present case, the
lesions identified on bone scintigraphy in the upper extremities
were ignored until whole body MRI and CT scans were performed, even
after the diagnosis with EH was verified post-operatively by
histopathological examination.
Radiography and CT of EH usually reveals a lytic
lesion without matrix mineralization that is localized in the
medullary to cortical bone. Cortical disruption and joint invasion
are also common features of EH. However, the signal characteristics
on MRI are non-specific. Low to intermediate signal intensity on
T1-weighted images and high signal intensity on T2-weighted images,
with homogeneous enhancement, are identified following the
injection of gadolinium-based contrast material (6,7,9). Detection of this tumor is difficult due
to its rarity and uncharacteristic radiographic appearance
(6,7).
The differential diagnoses of multiple contiguous EH of the bone
must include multifocal chondroblastoma, angiosarcoma and
metastatic tumors. Chondroblastoma is a rare, benign tumor of the
bone, which most frequently involves the epiphysis of the long
bones, particularly the femur and tibia. Radiographs, on which
chondroblastoma is difficult to differentiate from EH, show lytic
expansile lesion with cortical disruption, and frequent
encroachment of the articular cartilage. On MRI, the tumor exhibits
a low signal on T1-weighted images, while T2-weighted images
demonstrate high signal density components (12). Gadolinium-enhanced T1-weighted images
exhibit strong contrast enhancement of the tumor (12). There have been several reported cases
of multifocal chondroblastoma, which were considered as multiple
primary lesions (12,13). Aggressive chondroblastoma with
pulmonary metastasis is considered to be ‘malignant’
chondroblastoma (14). The term
‘aggressive’ chondroblastoma has been applied from a clinical point
of view rather than as a histopathological entity. The present case
was initially misdiagnosed as multiple chondroblastoma of the right
distal femur and proximal tibia, based on the uncharacteristic
radiographic appearance observed, and curettage of the lesions in
the proximal tibia and medial femoral condyle was therefore
performed.
A complete skeletal survey with bone scintigraphy is
recommended prior to radiological diagnosis, as it may show
undetected synchronous foci in completely separate anatomically
sites. In the present report, bone scintigraphy showed slight
increased radionuclide uptake in the right head of the humerus, but
not in the right scapula. However, initially, the lesions in the
right shoulder joint were ignored due to the lack of clinical
symptoms. In addition to plain radiography and scintigraphy, MRI
was performed in the present case, which revealed previously
undetected lytic lesions in the right scapula. Notably, Camarero
et al (15) identified no
clear correlation between the radionuclide uptake and signal
intensity on MRI for multicentric EH of the bone. Thus, CT may be
the modality of choice for the evaluation of the thorax and
exclusion of pulmonary metastases. In the present case, CT scans
revealed pulmonary metastases of the tumor, which were initially
missed on plain radiography of the chest.
Even with these specific radiological findings, the
formation of a definitive diagnosis of EH is difficult when based
on radiological findings alone. Therefore, the final diagnosis of
EH requires histopathological analysis. EH exhibits diffuse and
strong immunopositivity for vimentin and endothelial markers, such
as CD31 and CD34, with no reactivity for epithelial markers. In the
present case, the tumor cells were stained diffusely and intensely
with antibodies to vimentin, and showed immunoreactivity for CD31
and CD34. No staining was observed with the AE1/AE3 and EMA
epithelial markers.
Bone EH is a locally destructive tumor and its
clinical course is unpredictable on the basis of histological
features alone. Previous studies have indicated that multifocal EH
may exhibit a better prognosis than unifocal EH, however, the
pathogenesis remains controversial and the number of cases reported
is limited (8,16). Various mechanisms have been described,
including metastatic spread, malignant transformation and
multifocal formation. It is difficult to identify whether a
multicentric disease is primarily multicentric or whether it is a
result of metastases from a primary unicentric tumor (16,17).
Visceral involvement was reported to be the most important
criterion in predicting a poor prognosis. Kleer et al
(18) reported that 87.5% of EH
patients with visceral involvement succumbed to the disease.
At present, no standard treatment for EH has been
established. Although the majority of studies recommend radical
wide surgical resection or amputation as the optimal treatment of
multiple contiguous EH of the bone, (6,9) curettage
is also an option (7,8). We believe that hemangioendothelioma has
the potential to act aggressively and metastasize and thus
recommend a wide surgical resection. At present, treatment plans
should be tailored to the individual patient, according to the
extent and location of the disease. In the present case, as
curettage was initially performed for the treatment of
chondroblastoma of the right distal femur and proximal tibia, an
endoprosthetic replacement was not available and subsequently, an
amputation of the right leg at thigh level had to be performed. In
the present study, it was difficult to select an optimal treatment
for the tumors in the right head of the humerus and scapula, as
well as the lung, due to the widespread nature of the disease,
which was identified by radiological examination. Radiation therapy
may be administered alone or in combination with surgery,
particularly for widespread metastatic tumors or unresectable
lesions, as it has been shown to prevent local tumor progression
(6). At present, the efficacy of
chemotherapy has not been reported. Boutin et al (5) reported the case of one patient who
experienced no tumor regression after chemotherapy treatment for a
multicentric lesion. As a result, the patient in the present study
selected radiotherapy treatment for the right head of humerus and
scapula, but refused chemotherapy.
Bone multicentric EH is rare and must be
distinguished from multifocal chondroblastoma, angiosarcoma and
metastatic tumors. This report presents an extremely rare case of
bone multicentric EH, involving the upper and lower extremities
simultaneously. The results of this study may improve our
understanding with regard to the clinical features of EH, as well
as provide valuable insights for the accurate diagnosis, treatment
and improved prognosis of patients with this disease.
Acknowledgements
This study was supported by the National Natural
Science Foundation of China (grant no. 81301670) and the
Specialized Research Fund for the Doctoral Program of Higher
Education (grant no. 20110101120122).
References
|
1
|
Fletcher CDM, Unni KK and Merfens F: World
Health Organization Classification of Tumors: Pathology and
Genetics of Tumor of Soft Tissue and Bone. IARC Press; Lyon,
France: pp. 173–175. 2002
|
|
2
|
Bruegel M, Muenzel D, Waldt S, Specht K
and Rummeny EJ: Hepatic epithelioid hemangioendothelioma: findings
at CT and MRI including preliminary observations at
diffusion-weighted echo-planar imaging. Abdom Imaging. 36:415–424.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Jinghong X and Lirong C: Pulmonary
epithelioid hemangioendothelioma accompanied by bilateral multiple
calcified nodules in lung. Diagn Pathol. 6:212011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Deyrup AT, Tighiouart M, Montag AG and
Weiss SW: Epithelioid hemangioendothelioma of soft tissue: a
proposal for risk stratification based on 49 cases. Am J Surg
Pathol. 32:924–927. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Boutin RD, Spaeth HJ, Mangalik A and Sell
JJ: Epithelioid hemangioendothelioma of bone. Skeletal Radiol.
25:391–395. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Larochelle O, Périgny M, Lagacé R, Dion N
and Giguère C: Best cases from the AFIP: epithelioid
hemangioendothelioma of bone. Radiographics. 26:265–270. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ignacio EA, Palmer KM, Mathur SC, Schwartz
AM and Olan WJ: Epithelioid hemangioendothelioma of the lower
extremity. Radiographics. 19:531–537. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Liu Q, Miao J, Lian K, Huang L and Ding Z:
Multicentric epithelioid hemangioendothelioma involving the same
lower extremity: a case report and review of literature. Int J Med
Sci. 8:558–563. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gosheger G, Hardes J, Ozaki T, Horst E,
Bürger H and Winkelmann W: The multicentric epithelioid
hemangioendothelioma of bone: a case example and review of the
literature. J Cancer Res Clin Oncol. 128:11–18. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Weiss SW and Enzinger FM: Epithelioid
hemangioendothelioma: a vascular tumor often mistaken for a
carcinoma. Cancer. 50:970–981. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gómez-Arellano LI, Ferrari-Carballo T and
Domínguez-Malagón HR: Multicentric epithelioid hemangioendothelioma
of bone. Report of a case with radiologic-pathologic correlation.
Ann Diagn Pathol. 16:43–47. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Fukunaga M, Asanuma K and Irie T: Peculiar
chondroblastoma involving multiple tarsal bones. Skeletal Radiol.
39:709–714. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Robetis PF and Talor JG: Multifocal benign
chondroblastomas: report of a case. Hum Pathol. 11:296–298. 1980.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Elek EM, Grimer RJ, Mangham DC, Davies AM,
Carter SR and Tillman RM: Malignant chondroblastoma of the os
calcis. Sarcoma. 2:45–48. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Camarero A, Delgado M, Lorente R, Rayo JI
and Ramos JL: Multicentric epithelioid hemangioendothelioma of
bone: diagnostic imaging. Clin Nucl Med. 24:1002–1004. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Theurillat JP, Vavricka SR, Went P,
Weishaupt D, Perren A, Leonard-Meier C and Bachli EB: Morphologic
changes and altered gene expression in an epithelioid
hemangioendothelioma during a ten-year course of disease. Pathol
Res Pract. 199:165–170. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Evans HL, Raymond AK and Ayala AG:
Vascular tumors of bone: A study of 17 cases other than ordinary
hemangioma, with an evaluation of the relationship of
hemangioendothelioma of bone to epithelioid hemangioma, epithelioid
hemangioendothelioma and high-grade angiosarcoma. Hum Pathol.
34:680–689. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kleer CG, Unni KK and McLeod RA:
Epithelioid hemangioendothelioma of bone. Am J Surg Pathol.
20:1301–1311. 1996. View Article : Google Scholar : PubMed/NCBI
|