Introduction
A solitary fibrous tumor (SFT) is a type of spindle
cell tumor that was initially described as a tumor of the pleura
and peritoneum; however, it has also been identified in the central
nervous system, head and neck, visceral organs, skin and soft
tissues. For instance, SFTs have been described in the meninges,
paranasal sinuses, oral cavity, throat, orbit, lungs, liver,
thyroid, kidney, bladder and genitals (1–8). SFTs are
uncommon in thoracic and extrathoracic locations, with thoracic
SFTs accounting for <5% of all pleural neoplasms (9). SFTs principally affect middle-aged
adults (mean age, 51 years; range, 5–87 years) and exhibit no
gender predilection (3,8). The majority of thoracic SFTs are
asymptomatic while extrathoracic SFTs are usually symptomatic,
depending on tumor location and the size of the mass. Symptoms of
SFT in the head and neck are nonspecific; headaches often occur in
intracranial lesions and visual disturbances, poor memory, finger
clubbing and hypoglycemia have also been reported (2,6). The
majority of SFTs exhibit benign behavior and have a good outcome;
however, certain cases may have malignant features. In 10–15% of
cases, SFT recurrence and/or metastasis may occur; thus, it is
difficult to predict the postsurgical course of the disease
(10,11).
SFTs rarely occur in the sella turcica, with only
four cases of sellar SFT described in the literature thus far
(6,12–14)
(Table I). SFTs can be easily
misdiagnosed as they rarely occur and share similar radiological
and clinical symptoms with other sella turcica tumors, including
macroadenoma, meningioma and craniopharyngioma (6,12,14). The present study reports two cases of
SFT arising from the sellar region with suprasellar extension. The
clinical, imaging and histopathological findings, as well the
surgical outcomes, were discussed and recommendations for the
treatment of SFTs in the sella turcica were proposed. Written
informed consent was obtained from both patients.
 | Table I.Reported cases of sella turcica
solitary fibrous tumor as described in the literature, including
the present two cases. |
Table I.
Reported cases of sella turcica
solitary fibrous tumor as described in the literature, including
the present two cases.
| Patient | Author (year) | Gender | Age, years | Symptoms | Neuroimaging
examination results | Extent of
invasion | Surgery | Status at last
follow-up |
|---|
| 1 | Cassarino (2003) | F | 54 | Headaches and visual
impairment | Solid enhancing
intrasellar mass | Encased the carotid
artery and involved the sphenoid and cavernous sinuses | STR | NA |
| 2 | Pakasa (2005) | F | 66 | Headaches and visual
impairment | Solid enhancing
intrasellar mass | Extension to the
optic chiasm cavernous sinus and carotid arteries | STR | 14, 26 and 62 months
Rec, 78 months deceased |
| 3 | Furlanetto
(2009) | M | 28 | Visual
impairment | Solid enhancing
intrasellar mass | Compressed the optic
chiasm | GTR | 10 months NED |
| 4 | Yin (2010) | M | 32 | Headache,
ophthalmalgia and visual impairment | Solid enhancing
intrasellar mass | Compressed the left
optical nerve and chiasma | STR | 44 months NED |
| 5 | Present case | F | 20 | Headaches and visual
impairment | Solid enhancing
intrasellar mass | Compressed the optic
chiasm, invaded the left cavernous sinus and encased the carotid
artery | STR | 4 years NED |
| 6 | Present case | M | 22 | Visual
impairment | Solid enhancing
intrasellar mass | Compressed the optic
chiasm, and encased the anterior cerebral artery | GTR | 2 years NED |
Case report
Case one
In March 2011, a 20-year-old female presented with a
one-year history of menstrual disorder and five months of
deteriorating vision and was admitted to the Jinan Military General
Hospital (Jinan, China). Physical examination revealed
left-temporal hemianopsia and decreased visual acuity of the right
eye, while the prolactin levels were marginally elevated (591.7
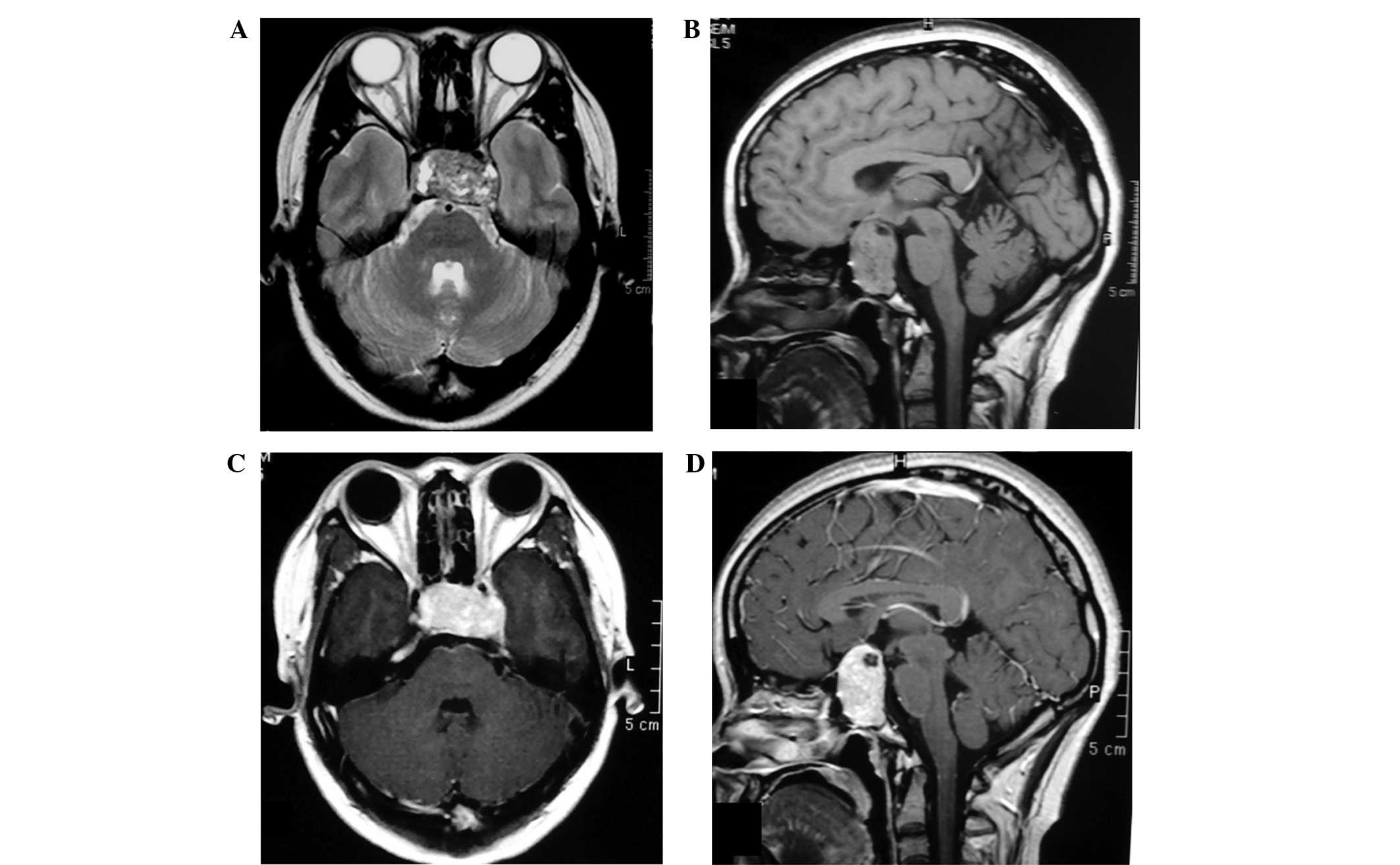
µlU/ml; normal range, 102–496 µlU/ml). Magnetic resonance imaging
(MRI) identified a well-marginated mass centered within the sellar
and suprasellar region. The mass extended into the sphenoid sinus,
compressed and elevated the optic chiasm, invaded the left
cavernous sinus and encased the cavernous internal carotid artery.
Furthermore, the lesion demonstrated low and high signal
intensities on T2-weighted images (T2-WIs) and an isointense signal
on T1-WIs (Fig. 1A and B), as well as
acute heterogeneous enhancement on post-contrast T1-WIs (Fig. 1C and D). Dural enhancement was
identified in the anterior cranial fossa (Fig. 1D). The initial diagnosis was a
pituitary macroadenoma; therefore, endoscopic transnasal
transsphenoidal microsurgery was performed. The microsurgery
identified a firm, highly vascular, brick red-colored tumor in the
sellar that bled easily during surgery. The surgery was prematurely
terminated due of excessive bleeding; therefore, only a small
section of the tumor was resected. Microscopic examination revealed
that the tumor was composed of highly atypical spindle cells with
varying degrees of fibrosis and interspersed with a branching
vascular component. Areas of cellular pleomorphism and increased
cellularity were present; however, mitosis was not identified
(Fig. 3A). Furthermore, Ki-67
expression exhibited scattered positivity (2% of tumor cells),
indicating a low level of active proliferation (Fig. 3B). Immunohistochemical staining
identified that the tumor cells were diffusely positive for
vimentin (Fig. 3C), cluster of
differentiation (CD) 34 (Fig. 3D) and
CD99. By contrast, the tumor cells were negative for epithelial
membrane antigen (EMA) and S-100 protein. These findings confirmed
the diagnosis of SFT. In April 2011, the patient underwent a second
craniotomy at Peking Union Medical College Hospital (Beijing,
China). Again, complete resection was not achieved due to excessive
hemorrhage. The patient is currently undergoing follow-up MRI
examination every 6 months and at the time of writing was well with
no evidence of residual tumor progression.
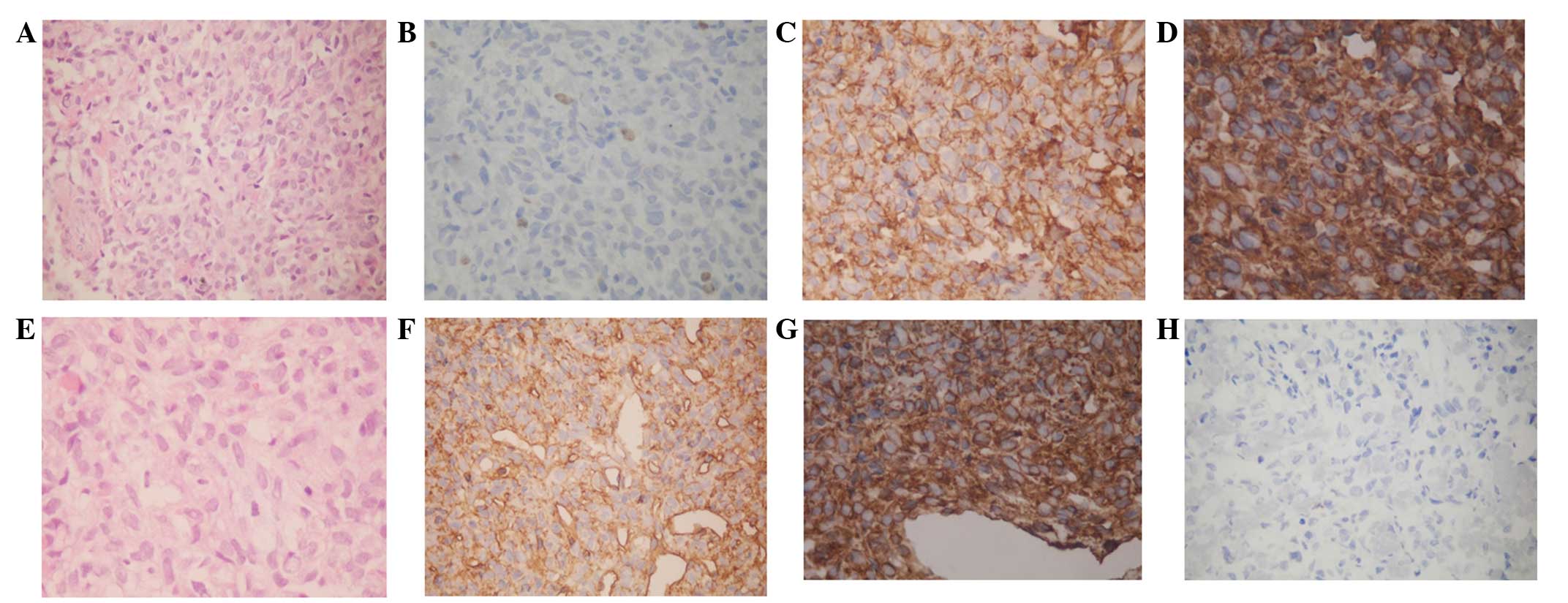 | Figure 3.Immunohistochemical staining in the
resected tumors of case one and two. Case one. (A) The tumor
consisted of highly spindle cells in a dense hyalinized collagenous
stroma, which consisted of alternating hypercellular and
hypocellular areas, while thin-walled staghorn branching vessels
were identified (hematoxylin and eosin staining; magnification,
×200). (B) Ki-67 demonstrated scattered positivity (2% of tumor
cells) (magnification, ×200). Immunohistochemically, the tumor
cells exhibited strong positive staining for (C) vimentin
(magnification, ×400) and (D) CD34 (magnification, ×400). Case two.
(E) The tumor was composed of spindle cells interspersed between
dense collagen bundles and vascular channels, without atypia
(hematoxylin and eosin staining; magnification, ×200).
Immunohistochemically, the tumor cells exhibited positive staining
for (F) CD34 (magnification, ×400) and (G) vimentin (magnification,
×400) and negative staining for (H) epithelial membrane antigen
(magnification, ×200). CD, cluster of differentiation. |
Case two
In February 2013, a 22-year-old male presented with
a five-month history of progressive reduced visual acuity and
visual field impairment and was admitted to the Jinan Military
General Hospital (Jinan, China). Laboratory examinations, including
endocrine investigations, revealed no abnormalities. General
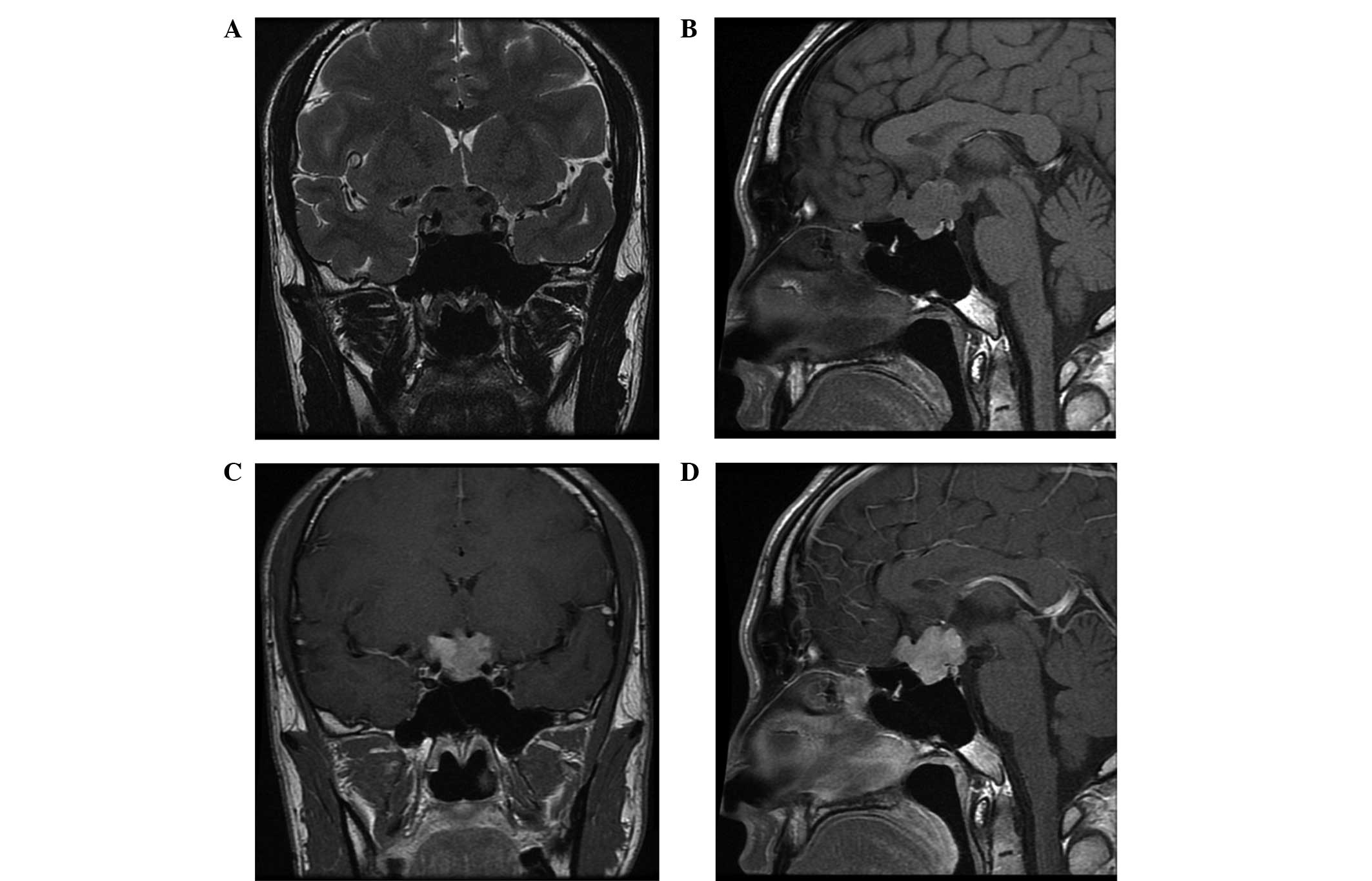
examination of the patient was also normal. However, an MRI scan
identified a 1.7×2.4-cm2 irregular, well-marginated mass
located in the sella and suprasellar region. The mass compressed
and elevated the optic chiasm and encased the anterior cerebral
artery. However, the cavernous sinus was not invaded. Furthermore,
healthy pituitary tissue was detected, although the edge was
unclear. On T1-WIs, the lesion exhibited isointense signals
relative to grey matter. Additionally, the mass was inhomogeneous
on T2-WIs and demonstrated homogeneous enhancement following
intravenous administration of 15 ml gadolinium (Fig. 2A-D). Based on the aforementioned
findings, the initial diagnosis was nonfunctional pituitary
macroadenoma; therefore, a craniotomy was performed.
Intraoperatively, a firm, fibrous and well-circumscribed mass was
observed in the sellar region, with cerebral dural matter
infiltrating, but not invading, the pituitary gland. The tumor was
completely removed; however, blindness in the left eye occurred
following surgery, possibly due to damage to the blood vessel of
the optic chiasm. Microscopically, the tumor was composed of
clusters of spindle-shaped cells interspersed between dense
collagen bundles and vascular channels, without atypia (Figure. 3E). Ki-67 expression exhibited
scattered positivity (2–5% of tumor cells), indicating a low level
of active proliferation. Immunohistochemical staining identified
that the tumor cells were positive for CD34 (Fig. 3F) and vimentin (Fig. 3G) but negative for EMA (Fig. 3H) and S-100 protein. Histological and
immunohistochemical analysis of the resected tumor identified
determined results similar to case one, thus, resulting in a
diagnosis of SFT. Follow-up MRI examinations every 6 months were
planned and at the time of writing the patient was asymptomatic
with no evidence of disease or recurrence.
Discussion
Numerous SFT cases have been identified in the
central nervous system (CNS). However, a literature search of the
PubMed database (http://www.ncbi.nlm.nih.gov/pubmed), using the search
term ‘sella turcica solitary fibrous tumor’ revealed that only four
cases involving the sella turcica have been published in the
English literature to date (6,12–14) (Table I);
thus, the sella turcica is a relatively uncommon site of SFT. In
light of its rarity and considering that SFT may mimic other types
of tumor located in the sellar and suprasellar area, SFT of the
sella turcica is easily misdiagnosed prior to surgery. The six
known SFT cases, including the four cases reported in the
literature (6,12–14) and
the two cases reported in the present study, were initially
diagnosed as pituitary macroadenomas. Among the six cases, three
were male and three were female patients, with an age range of
20–66 years and an average age of 37 years.
Clinically, SFTs are slow-growing and their symptoms
depend on the tumor size (maximum length along the sagittal plane,
2–3 cm) (14). The four
previously-described cases presented with reduced visual acuity and
visual field impairment. Endocrine investigations were normal, with
the exception of case one in the present study, in which prolactin
levels were mildly elevated; this is described as the stalk section
effect, where the pituitary stalk may become compressed due to
suprasellar tumors, resulting in subsequent hyperprolactinemia
(15). However, these clinical
features are non-specific.
Radiological investigation identified a
heterogeneous mass inside and above the pituitary fossa in six
cases (images not provided in two cases). The pituitary gland was
located in case two of the present study; however, it was not
clearly identifiable in all other cases. Comparing the six known
cases of sellar SFT, including the two cases of the present study,
the following were determined as common features of sellar SFTs:
Well-marginated mass, inhomogeneous on T2-WI, homogeneous and
isointense signal on T1-WI, acute enhancement on post-contrast
T1-WI and local invasion. In addition, cavernous sinuses were
invaded in 3/6 cases, the carotid artery was encased in 3/6 cases,
and the sphenoid and temporal bones were infiltrated in 1/6 cases.
No pathognomonic findings were elucidated and sellar SFTs were
demonstrated to share similar imaging characteristics with
pituitary macroadenomas (6,12,13,16).
Therefore, although the occurrence of SFT in the sellar turcica is
rare, it should be considered during differential diagnosis.
The pathological features of an SFT of the sella
turcica resemble those described for SFTs in other regions. For
instance, immunohistochemically, the six sellar SFT cases exhibited
reactivity with CD34 and vimentin, but were negative for S-100
protein, smooth muscle actin and EMA. Five cases were positive for
CD99, while one case was negative. Although CD34 may be negative in
a small number of cases (range, 5–30%), strongly positive CD34
staining is a characteristic immunohistochemical feature of SFTs
(17).
The six reported cases of SFT underwent surgery.
Endoscopic transnasal transsphenoidal microsurgery was performed in
three cases (12,13), with the tumor being completely
resected in one case (12), which
resulted in a cerebrospinal fluid (CSF) fistula. The tumor was
incompletely removed in the other two cases (13,14). In
the other three cases, craniotomy with a fronto-pterional approach
was performed (6), with complete
tumor resection in one case, which resulted in blindness. The tumor
was incompletely removed in the other two cases (6). Generally, the tumors were hard, locally
invasive and highly vascularized, precluding complete resection.
Stereoradiotherapy was performed in two cases (13,14); one
patient succumbed due to uncontrolled disease progression (13) and the other patient was followed up
for 44 months with no indication of progression or distant
metastasis of the residual tumor (14).
In conclusion, it has been previously reported that
stereotactic and external beam radiotherapy are effective treatment
strategies for residual or inoperable recurrences of SFT (14,17–19).
Therefore, since complete resection may result in complications
such as CFS fistulas and blindness, while stereotactic radiotherapy
is known to be effective, the present study proposes that a
subtotal resection should be considered as an acceptable surgical
approach for the treatment of recurrent or residual intracranial
SFTs in cases where removal of the sellar tumor is difficult. In
addition, careful follow-up is required in all cases of sellar SFT
as the tumor exhibits long-term malignant potential and an
unpredictable clinical outcome. However, drawing definite
conclusions is difficult due to the limited number of cases
reported in the literature to date.
References
|
1
|
Caroli E, Salvati M, Orlando ER, Lenzi J,
Santoro A and Giangaspero F: Solitary fibrous tumors of the
meninges: report of four cases and literature review. Neurosurg
Rev. 27:246–251. 2004.PubMed/NCBI
|
|
2
|
Metellus P, Bouvier C, Guyotat J, Fuentes
S, Jouvet A, Vasiljevic A, Giorgi R, Dufour H, Grisoli F and
Figarella-Branger D: Solitary fibrous tumors of the central nervous
system: clinicopathological and therapeutic considerations of 18
cases. Neurosurgery. 60:715–722. 2007.PubMed/NCBI
|
|
3
|
Nai GA, Ramalho N and eto GC: Solitary
fibrous tumor of the nasal cavity. Braz J Otorhinolaryngol.
75:7692009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sun K, Lu JJ, Teng XD, Ying LX and Wei JF:
Solitary fibrous tumor of the liver: a case report. World J Surg
Oncol. 9:372011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wignall OJ, Moskovic EC, Thway K and
Thomas JM: Solitary fibrous tumors of the soft tissues: review of
the imaging and clinical features with histopathologic correlation.
AJR Am J Roentgenol. 195:W55–W62. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cassarino DS, Auerbach A and Rushing EJ:
Widely invasive solitary fibrous tumor of the sphenoid sinus,
cavernous sinus, and pituitary fossa. Ann Diagn Pathol. 7:169–173.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kim SA, Hwang JE, Ro JY, Cho KJ, Song C
and Kim MJ: Solitary fibrous tumor of the kidney: A report of two
cases with review of literature. Korean J Pathol. 44:420–425. 2010.
View Article : Google Scholar
|
|
8
|
Talvitie H, Aström K, Larsson O, Ahlén J,
Bergh A and Egevad L: Solitary fibrous tumor of the prostate: a
report of two cases. Pathol Int. 61:536–538. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Cardillo G, Carbone L, Carleo F, Masala N,
Graziano P, Bray A and Martelli M: Solitary fibrous tumors of the
pleura: An analysis of 110 patients treated in a single
institution. Ann Thorac Surg. 88:1632–1637. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ning S, Song X, Xiang L, Chen Y, Cheng Y
and Chen H: Malignant solitary fibrous tumor of the thyroid gland:
report of a case and review of the literature. Diagn Cytopathol.
39:694–699. 2011. View
Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ikeda T, Wada N, Nomura M, Tamiya S and
Ushijima M: A case of solitary fibrous malignant tumor with
multiple metastases. Nihon Kokyuki Gakkai Zasshi. 49:913–916.
2011.(In Japanese). PubMed/NCBI
|
|
12
|
Furlanetto TW, Pinheiro CF, Oppitz PP, de
Alencastro LC and Asa SL: Solitary fibrous tumor of the sella
mimicking pituitary adenoma: an uncommon tumor in a rare location -
a case report. Endocr Pathol. 20:56–61. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Pakasa NM, Pasquier B, Chambonnière ML,
Morrison AL, Khaddage A, Perret AG, Dumollard JM, Barral FG and
Péoc'h M: Atypical presentations of solitary fibrous tumors of the
central nervous system: an analysis of unusual clinicopathological
and outcome patterns in three new cases with a review of the
literature. Virchows Arch. 447:81–86. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Yin W, Ma C, Wu J, Cai B and You C: A
primary atypical solitary fibrous tumor of the sella mimicking
nonfunctional pituitary adenoma: a case report. Acta Neurochir
(Wien). 152:519–522. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Rupp D and Molitch M: Pituitary stalk
lesions. Curr Opin Endocrinol Diabetes Obes. 15:339–345. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Vassal F, Manet R, Forest F, Camdessanche
JP, Péoc'h M and Nuti C: Solitary fibrous tumors of the central
nervous system: report of five cases with unusual
clinicopathological and outcome patterns. Acta Neurochir (Wien).
153:377–384. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Bisceglia M, Galliani C, Giannatempo G,
Lauriola W, Bianco M, D'Angelo V, Pizzolitto S, Vita G, Pasquinelli
G, Magro G and Dor DB: Solitary fibrous tumor of the central
nervous system: a 15-year literature survey of 220 cases (August
1996-July 2011). Adv Anat Pathol. 18:356–392. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Saynak M, Bayir-Angin G, Kocak Z, Oz-Puyan
F, Hayar M, Cosar-Alas R, Karamustafaoglu A, Yurut-Caloglu V,
Caloglu M and Yoruk Y: Recurrent solitary fibrous tumor of the
pleura: significant response to radiotherapy. Med Oncol. 27:45–48.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Reames DL, Mohila CA and Sheehan JP:
Treatment of intracranial solitary fibrous tumors with gamma knife
radiosurgery: report of two cases and review of literature.
Neurosurgery. 69:E1023–E1028. 2011. View Article : Google Scholar : PubMed/NCBI
|