Introduction
Lymphomas are malignant lymphocytes. They may be
classified as Hodgkin's lymphoma and non-Hodgkin's lymphoma
(1). Non-Hodgkin's malignant
lymphomas may be divided into nodal and extranodal lymphoma. The
gastrointestinal tract is the most common site of extranodal
lymphoma (2).
Primary gastrointestinal lymphoma occurs in the
absence of evidence of systemic disease. Dawson et al
(3) established criteria for the
diagnosis of primary colorectal lymphomas in 1961. These are: No
palpable, superficial lymph nodes at presentation; no enlarged
mediastinal lymph nodes on chest X-ray; normal range for white
blood cell count including total and differential; at surgery, only
the regional lymph nodes are involved; and the liver and spleen are
without disease.
Controversy remains with regard to the therapeutic
approaches of treating gastrointestinal lymphomas. The optimal
treatment for primary rectal lymphoma remains unclear, and further
research is still required. In this paper, we present a case of
primary lymphoma of the rectum and focus on the role of
chemotherapy.
Case report
In July 2012, a 51-year-old female attended the
outpatient clinic of Renji Hospital, Shanghai, China, with
complaints of change in bowel habits, rectal bleeding. Rectoscopy
revealed proctitis with erosion, and the histology of biopsy
specimens revealed chronic inflammation of mucous membranes.
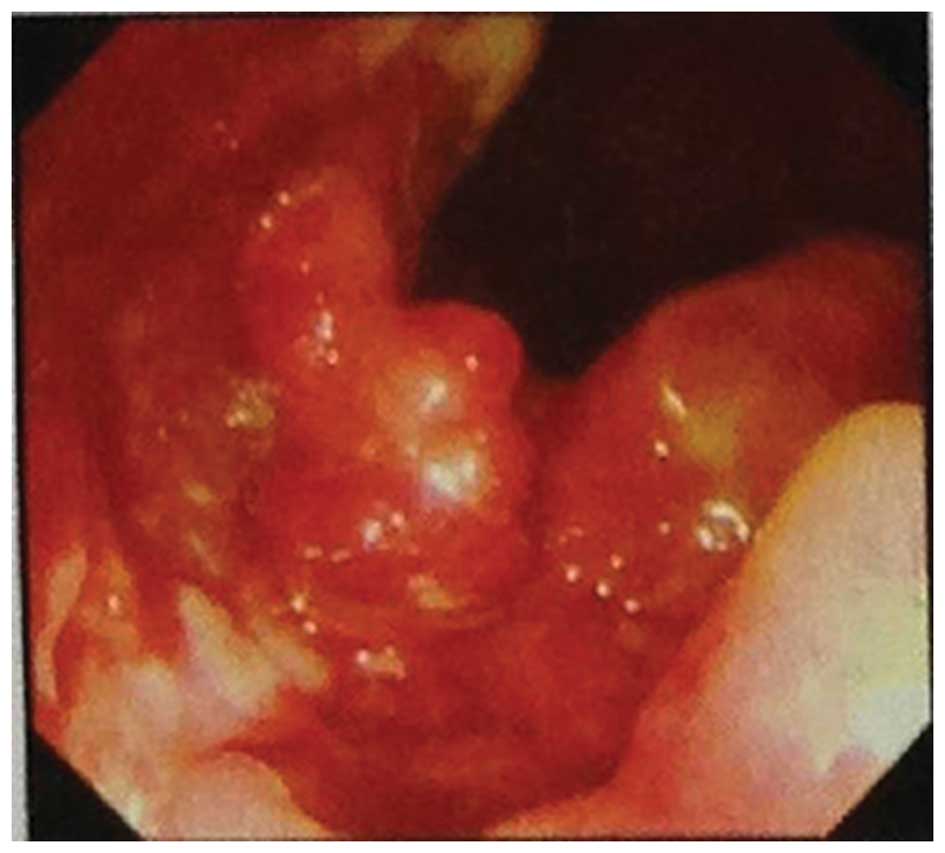
When the patient came to our clinic, her clinical
manifestation was severe rectal bleeding. A palpable mass was
identified on directeral rectal examination. The mass was located
in the dentate line, and fixed to the rectal wall. The superior
border of the tumor could not be reached. A repeat colonoscopy
revealed a three-quarters circumferential lesion approximately 3–8
cm from the anal verge. The ulcer was infiltrating with necrotic
tissue in the central area, and the margins demonstrated nodular
uplift (Fig. 1). By histopathological
diagnosis, the rectal biopsy specimen was diagnosed as
non-Hodgkin's diffuse large B-cell lymphoma (DLBCL). The results of
immunohistochemical staining were CD20(+), CD79a(+), CD30(+),
Bcl-2(–), CD10(–), Mum-1(–), CD21(–), CD23(–), CK(–), Vim(+) and
Ki-67 >40%. Abdominopelvic computed tomography (CT) demonstrated
that the rectal wall had local thickening, and the fat gap
surrounding the colon wall contained small scattered lymph nodes
(Fig. 2). Additional examinations did
not reveal any evidence of infiltration to other organs.
It was finally decided not to resect the rectum
where the lesion located due to the fact that the lesion completely
disappeared after the patient had received four cycles of
cyclophosphamide, hydroxydaunomycin, oncovin and prednisolone
(CHOP) chemotherapy. A complete remission was achieved and
confirmed by abdominal CT scan and colonoscopy with a biopsy of the
diseased region.
Discussion
Primary rectal lymphoma is the rarest disorder of
all primary gastrointestinal lymphomas, accounting for 0.1–0.6% of
all colonic malignancies and 0.05% of all primary rectal
malignancies (4). The majority of
patients with rectal lymphoma present with non-specific symptoms or
negative rectal biopsy, which often leads to delays in diagnosis
and an advanced stage at presentation, where rectal bleeding may be
observed as with primary rectal carcinoma (5). Endoscopy with biopsy and abdominal CT
are the most valuable diagnostic tests.
CT examination for the diagnosis of rectal lymphoma
has not attracted sufficient attention for a long time. Primary
colorectal lymphomas often manifest as discrete masses and tend to
have a greater depth of mural invasion than infiltrative lesions
(6). Research has identified that
when CT reveals concentric wall thickening, involving the full
thickness of the bowel wall without an associated desmoplastic
reaction, lymphoma should be the primary consideration in the
differential diagnosis (7,8). Although the characteristic tumor
morphology and imaging aid in the diagnosis, pathological analysis
of a biopsy remains the gold standard for diagnosis of this
disease. As colorectal lymphoma originates from the submucosa of
the colon, accurately obtaining a biopsy sample may be challenging,
and the pathological positive rate is low (9,10).
Therefore when a biopsy is obtained via colonoscopy, experienced
endoscopists are required. As there is only a low incidence of the
disease, there have been no prospective studies evaluating the
relative benefits of adjuvant chemotherapy, radiotherapy, surgery
or a combination of treatments for primary rectal lymphoma
(11). DLBCL of the colorectum
generally has a uniform method of treatment: chemotherapy followed
by aggressive surgical treatment (12). Due to its varied histological
behaviors and clinical presentations, rectal lymphoma should be
considered as a different clinicopathological type. For this
reason, individualized treatment programs need to be developed
based on specific clinical situations (13). Although it is not possible to make a
reasonable conclusion with a few cases, we emphasize the
significance of chemotherapy in achieving a successful cure for
patients with rectal DLBCL.
References
|
1
|
Jaffe E, Harris NL, Stein H and Vardiman
JW: WHO Classification of Tumours: Pathology and Genetics of
Tumours of Hematopoietic and Lymphoid Tissues. IARC Press; Lyon:
2001
|
|
2
|
Muller-Hermelink HK, Chott A, Gascoyne RD
and Wotherspoon A: B-cell lymphoma of the colon and rectumWHO
Classification of Tumours. Pathology and Genetics of Tumours of the
Digestive System. Hamilton SR and Aaltonen LA: IARC Press; Lyon:
pp. 139–141. 2000
|
|
3
|
Dawson IM, Cornes JS and Morson BC:
Primary malignant lymphoid tumours of the intestinal tract. Report
of 37 cases with a study of factors influencing prognosis. Br J
Surg. 49:80–89. 1961. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Dodd GD: Lymphoma of the hollow abdominal
viscera. Radiol Clin North Am. 28:771–783. 1990.PubMed/NCBI
|
|
5
|
Quayle FJ and Lowney JK: Colorectal
lymphoma. Clin Colon Rectal Surg. 19:49–53. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wyatt SH, Fishman EK, Hruban RH and
Siegelman SS: CT of primary colonic lymphoma. Clin Imaging.
18:131–141. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Degeorges S, Mesnil A, Marion-Audibert AM,
et al: Ano-rectal symptoms, related to Epstein-Barr
Virus-Associated Burkitts lymphoma in an immunocompetent patient.
Gastronterol Clin Biol. 31:442–444. 2007.(In French).
|
|
8
|
Stanojevic GZ, Nestorovic MD, Brankovic
BR, et al: Primary colorectal lymphoma: An overview. World J
Gastrointest Oncol. 3:14–18. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Zhang RP, Qiang L, Tao S, et al: 68 cases
of primary colorectal non-Hodgkin's lymphoma clinical analysis.
Zhongguo Zhonghua Weichang Waike Zazhi. 6:49–51. 2004.(In
Chinese).
|
|
10
|
Yang JO, Zhang S, Zhen WJ and Zhen HH:
Diagnosis and treatment of primary malignant lymphoma of the
rectum. Jie Zhichang Gangmen Waike. 18:13–15. 2012.(In
Chinese).
|
|
11
|
Friedlich M, Lamba M and Stern H:
Management of rectal lymphoma. Can J Surg. 47:142–143.
2004.PubMed/NCBI
|
|
12
|
Avilés A, Neri N and Huerta-Guzmán J:
Large bowel lymphoma: an analysis of prognostic factors and therapy
in 53 patients. J Surg Oncol. 80:111–115. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Bilsel Y, Balik E, Yamaner S and Bugra D:
Clinical and therapeutic considerations of rectal lymphoma: a case
report and literature review. World J Gastroenterol. 11:460–461.
2005. View Article : Google Scholar : PubMed/NCBI
|