Introduction
The concept of global burden of disease (GBD)
emerged when it was perceived that the use of mortality as a
measure of disease burden reflects only a section of population
health and this metric does not incorporate the impact of
disability (1–4). A key measure for GBD is the number of
disability adjusted life years (DALYs), which is calculated from
the sum of two other measures, consisting of the years of life lost
(YLLs) and years lived with disability (YLDs) (5). These composite measures incorporate and
synthesize estimates of the incidence, prevalence and duration of a
particular condition, and the outcome, either disability or
premature death. The measures were developed for the objective
assessment of the burden of disease within the population of one
country, at a national or subnational level, and within populations
of regions and continents (2,6,7).
Four factors determined the conception and design of
this study. The first was that malignancies have not been
previously ranked by national burden of disease (NBD) in Lithuania
with reference to the composite single indicators. The second was
that there is no data on the national burden of colorectal cancer
in the population of Lithuania at present. The third reason was
that there is no comparative assessment between the performance of
Lithuania for colorectal cancer and other European nations based on
ranking. The fourth was that objective assessment of NBD is
required prior to the complete implementation of a national
colorectal cancer screening and prevention programme in
Lithuania.
The analysis that follows, therefore, elaborates on
the national burden of all malignancies and colorectal cancer in
Lithuania. The performance of Lithuania in terms of colorectal
cancer is assessed by comparison with 45 European nations by their
ranking. The present study aimed to produce trends for the
incidence of colorectal cancer, and also for the mortality, DALYs,
YLLs and YLDs due to colorectal cancer. The percentage change of
the aforementioned measures was assessed for countries and regions
between 1990 and 2010. The ranking of Lithuania was also assessed
to determine whether the country was above or below the average of
the currently named or historic European regions. An additional
reason for the production of the present study was to encourage the
adoption of the composite metrics of GBD as a health policy so that
estimates of NBD may be produced for Lithuania and its regions on a
regular basis (8).
Materials and methods
Seven sources of data and information were used for
the creation and analysis of the present figures and tables. These
sources were the WHO Department of Measurement and Health
Information (8), International Agency
for Research on Cancer, GLOBOCAN (9),
Lithuanian Health Information Centre (10), WHO European Detailed Mortality
Database (11), Global Burden of
Disease Study, Institute for Health Metrics and Evaluation
(12), Statistics Lithuania (13) and Lithuanian Cancer Registry (14). The majority of the data on disease
burden are reported in the present study by gender as
age-standardised DALYs, YLLs and YLDs per 100,000 individuals per
year. The WHO population age standard for each gender was used for
the expression of age-standardised rates (8,9,11,12). Other
metrics, including the crude incidence rate and mortality,
age-standardised and age-specific mortality rates for colorectal
cancer were also used in the present study for the clarification of
anomalies in the NBD of Lithuania. The International Statistical
Classification of Diseases and Related Health Problems (10th
revision), codes C18-21 for malignant neoplasms of the colon,
rectosigmoid junction, rectum, anal canal and anus (http://apps.who.int/classifications/icd10/browse/2015/en)
were used to search for incidence and mortality data within the
Health Indicators of the Lithuania database and the European
Detailed Mortality Database (10,11).
The comparative analysis of the burden of colorectal
cancer incorporated the data from 45 European nations. The present
study aimed to produce trends for the incidence and mortality of
colorectal cancer, and the DALYs, YLLs and YLDs due to this
disease. The percentage change of these measures in countries and
regions between 1990 and 2000 was also determined.
The data from Lithuania were assessed to determine
if the country was above or below the average of the currently
named or historic European regions. The Northern, Southern,
Western, and Central and Eastern regions of Europe were defined by
GLOBOCAN 2008 (9). The original EU-15
consisted of the following countries: Denmark, Germany, the UK,
Belgium, Luxembourg, Austria, Italy, Netherlands, Ireland, France,
Sweden, Portugal, Spain, Finland and Greece. The terms ‘communist
countries in 1990′ and ‘democratic countries in 1990′ are historic.
The first term includes all the communist countries of Europe in
1990, with the exception of the German Democratic Republic.
Results
Leading causes of NBD
The fourth leading cause of NBD is malignancies,
with the preceding three causes being injuries, neuropsychiatric
conditions and cardiovascular conditions in Lithuania. Malignancies
account for 9.8% of the disease burden resulting from males, with
2098 DALYs per 100,000 males in 2004, and 11.2% of the disease
burden that arises from females, with 1369 DALYs per 100,000
females in 2004. Malignancies are the fourth leading cause of the
NBD accounted for by males, preceded by injuries (26.6%),
cardiovascular diseases (21.1%) and neuropsychiatric conditions
(18%). In females, malignancies rank third, being preceded by
neuropsychiatric conditions (25.7%) and cardiovascular diseases
(15.2%).
Ranking of malignancies by DALYs and
YLDs
The national burden of 10 malignant oncological
diseases is reported and ranked in Table
I. Colorectal cancer was the third (8.6%) leading cause of
DALYs in males in Lithuania in 2008, preceded by lung (23.8%) and
stomach (9.9%) cancers. In the female population, colorectal cancer
was also the third leading cause of DALYs, preceded by breast
(21.3%) and uterine cervix (11.8%) cancers. The burden of malignant
disease was 37.3% higher in males than females in Lithuania in
2008.
 | Table I.Ten causes of the national burden of
malignancies ranked by DALYs and YLDs in 100,000 men and 100,000
women in 2008, Lithuania. |
Table I.
Ten causes of the national burden of
malignancies ranked by DALYs and YLDs in 100,000 men and 100,000
women in 2008, Lithuania.
| A, Male patients
(n=100,000) |
|---|
|
|---|
|
| DALYs | YLDs |
|---|
|
|
|
|
|---|
| Rank | Cancer | n | % | Cancer | n | % |
|---|
| 1 | Lung | 886 | 23.8 | Prostate | 78 | 28.1 |
| 2 | Stomach | 368 | 9.9 | Colorectum | 48 | 17.3 |
| 3 | Colorectum | 321 | 8.6 | Lung | 28 | 10.1 |
| 4 | Prostate | 306 | 8.2 | Stomach | 21 | 7.6 |
| 5 | Leukaemia | 182 | 4.9 | Bladder | 14 | 5.0 |
| 6 | Pancreas | 177 | 4.8 | Lip, oral cavity | 12 | 4.3 |
| 7 | Kidney | 152 | 4.1 | Kidney | 10 | 3.6 |
| 8 | Oesophagus | 152 | 4.1 | Other pharynx | 10 | 3.6 |
| 9 | Nervous system | 152 | 4.1 | Larynx | 9 | 3.2 |
| 10 | Larynx | 135 | 3.6 | Non-Hodgkin's
lymphoma | 6 | 2.2 |
|
| All
cancersa | 3721 | 100.0 | All
cancersa | 278 | 100.0 |
|
| B, Female patients
(n=100,000) |
|
|
| DALYs | YLDs |
|
|
|
|
| Rank | Cancer | n | % | Cancer | n | % |
|
| 1 | Breast | 577 | 21.3 | Breast | 125 | 39.3 |
| 2 | Uterine cervix | 319 | 11.8 | Uterine cervix | 52 | 16.4 |
| 3 | Colorectum | 240 | 8.9 | Uterine corpus | 37 | 11.6 |
| 4 | Ovary | 208 | 7.7 | Colorectum | 30 | 9.4 |
| 5 | Stomach | 190 | 7.0 | Ovary | 19 | 6.0 |
| 6 | Brain, nervous
system | 151 | 5.6 | Stomach | 9 | 2.8 |
| 7 | Lung | 128 | 4.7 | Non-Hodgkin's
lymphoma | 5 | 1.6 |
| 8 | Leukaemia | 118 | 4.4 | Kidney | 5 | 1.6 |
| 9 | Uterine corpus | 99 | 3.7 | Melanoma of skin | 4 | 1.3 |
| 10 | Pancreas | 96 | 3.5 | Thyroid | 4 | 1.3 |
|
| All
cancersa | 2711 | 100.0 | All
cancersa | 318 | 100.0 |
Table I also reveals
the contribution of the YLDs accounted for by the 10 leading
malignant diseases to the total disability-associated burden of
malignant diseases for Lithuania. The disability burden of
malignant disease was revealed to be 14.4% higher in females than
males. Prostate and colorectal cancers were the leading
contributors, accounting for almost 45.8% of the disease burden due
to disability in the male population. In females, colorectal cancer
was the fourth leading cause (9.4%), preceded by breast (39.3%) and
uterine cancers of either the cervix or corpus (28%).
Incidence of colorectal cancer and the
ranking of Lithuania
Overall, the crude incidence of colorectal cancer in
Lithuania per 100,000 individuals was 35 in 2001 and 51 in 2011.
The overall incidence varied between the ten counties and five
cities of Lithuania. In 2011, the incidence was 68 and 42 cases per
100,000 individuals in the cities Vilnius and Kaunas, and 62 and 35
cases per 100,000 individuals in the counties Panevėžys and
Tauragė. The incidence of colorectal cancer increased in all
Lithuanian regions, with the exception of Western Lithuania. The
incidence decreased in Western Lithuania over the 11 years. The
overall age-standardised incidence of colorectal cancer for the two
genders was 25 cases per 100,000 individuals in Lithuania,
resulting in Lithuania being ranked as the 27th country out of the
comparative nations in 2008. The overall age-standardised incidence
of colorectal cancer for the two genders was highest in the Central
European countries of Slovakia, Hungary and the Czech Republic in
2008, with 42, 41 and 39 cases per 100,000 individuals,
respectively.
With the age-standardised incidence of 33 colorectal
cancer cases per 100,000 males, Lithuania was ranked 22nd out of
the 45 European countries. The same incidence was estimated in
Poland. The incidence of colorectal cancer in males was highest in
Slovakia, Hungary and the Czech Republic, with 61, 56 and 54 cases
per 100,000 males, respectively. In females, the incidence of
colorectal cancer was highest in Israel, Norway, and Denmark, with
36, 34 and 34 cases per 100,000 females, respectively. Lithuania,
with the age-standardised incidence rate of 20 cases per 100,000
females, was ranked as 29th in 2008, the same ranking as the
Republic of Moldova, Austria and Latvia.
Mortality due to colorectal
cancer
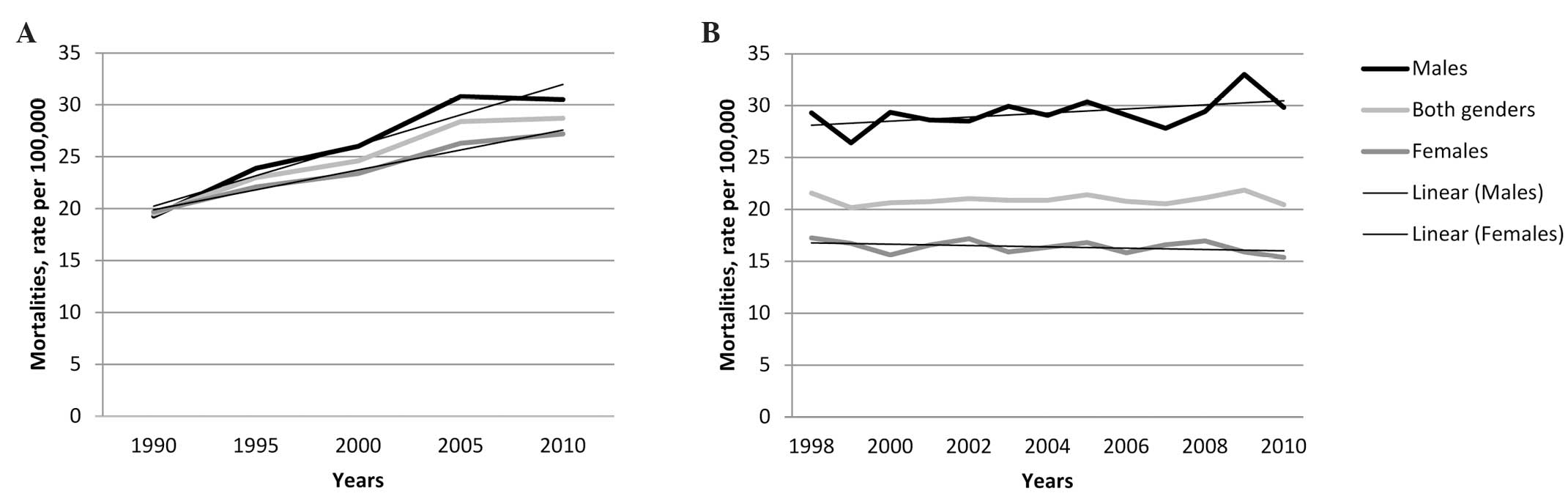
There were 719 mortalities associated with
colorectal cancer in Lithuania in 1990, out of a total population
of 3.67 million individuals (12).
Despite the decrease in population size of 16% in 2010, 958
mortalities were registered as associated with colorectal cancer in
2010, resulting in a 24.9% increase in colorectal cancer-associated
mortalities between 1990 and 2010. This resulted in a sharp 36.7%
increase in the male mortality rate, 27.6% increase in the female
mortality rate, and 32.1% increase in the overall mortality rate
associated with colorectal cancer in the two genders between 1990
and 2010. It is important to note that the trends based on
different sources of information vary slightly (11,12), as
demonstrated by Fig. 1.
Mortality pattern by age and
gender
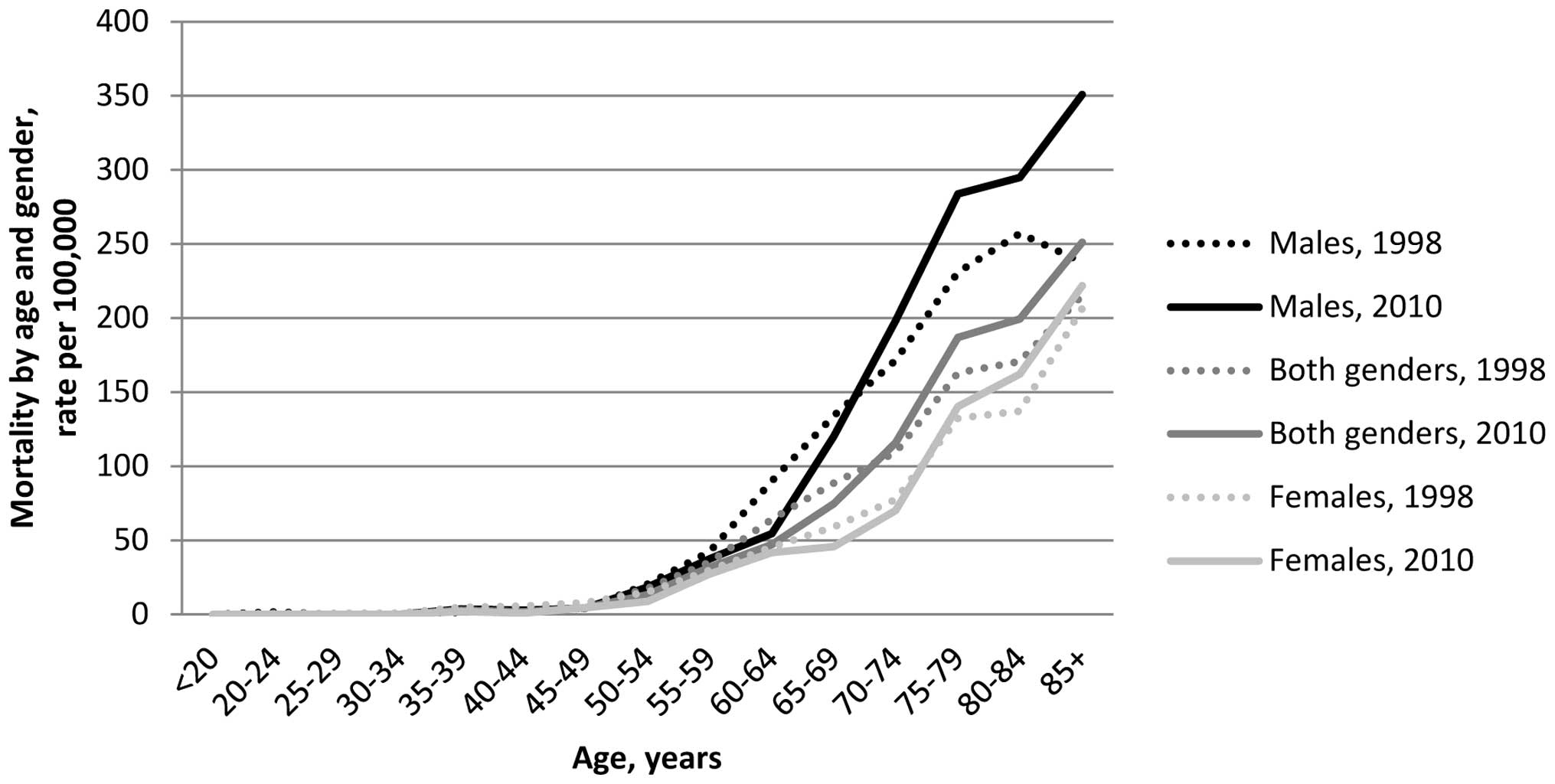
Fig. 2 depicts a
pattern based on the crude age-specific mortality rates of
colorectal cancer by age, gender and the two genders combined in
1998 and 2010 in Lithuania. All six mortality curves in the
Fig. 2 began to increase in the age
group of 45–49 years. The mortality rate was 4–5 times higher in
males aged 50–54 years than in males aged 45–49 years. The
mortality rate was two times higher in females aged 50–54 years
than in females aged 45–49 years. The mortality rates were markedly
increased in males aged ≥65 compared with females of the same age
group. The highest crude mortality rate occurred in males aged ≥85,
with 351 mortalities per 100,000 males in 2010. In the same year,
the mortality rate in females aged ≥85 was 222 mortalities per
100,000 females.
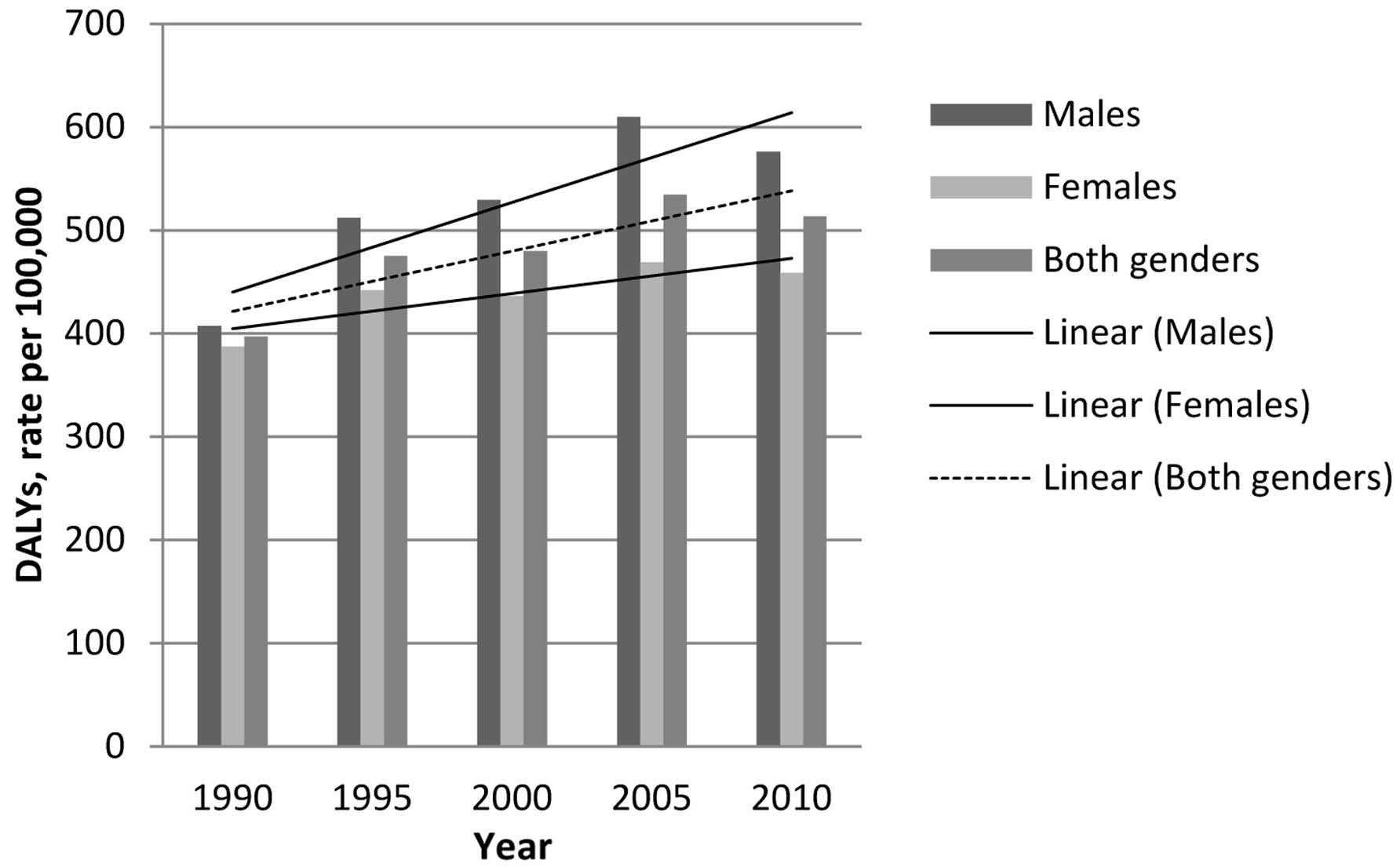
DALYs due to colorectal cancer
Fig. 3 reveals the
number of DALYs per 100,000 individuals per year in Lithuania due
to colorectal cancer between 1990 and 2010 in males, females and
the two genders combined for all ages. The national burden of
colorectal cancer was highest in 2005. In males, females and the
two genders combined, the number of DALYs was decreased in 2010
compared with 2005. The burden of colorectal cancer was greater in
males than females.
YLDs caused by colorectal cancer
The number of YLDs caused by colorectal cancer
increased by 42.6% in the age-standardised population of 100,000
males, by 35.6% in the age-standardised female population and by
38.9% in the age-standardised overall population between 1990 and
2010. The number of YLDs increased between 11 and 19 years in
males, between 12 and 18 years in females, and between 11 and 18.5
years overall in the two genders between 1990 and 2010.
Distribution of YLLs and YLDs due to
colorectal cancer
In total, 97% of DALYs arising from colorectal
cancer were from YLLs and 3% of DALYs were from YLDs in 1990, 1995,
2000, 2005 and 2010. However, there is a slight non-significant
trend towards a decrease in the number of YLLs and increase in the
number of YLDs between 1990 and 2010. This trend is more evident in
females than in males, as 3.0% of female DALYs were comprised by
YLDs in 1990 and 3.9% were comprised by YLDs in 2010.
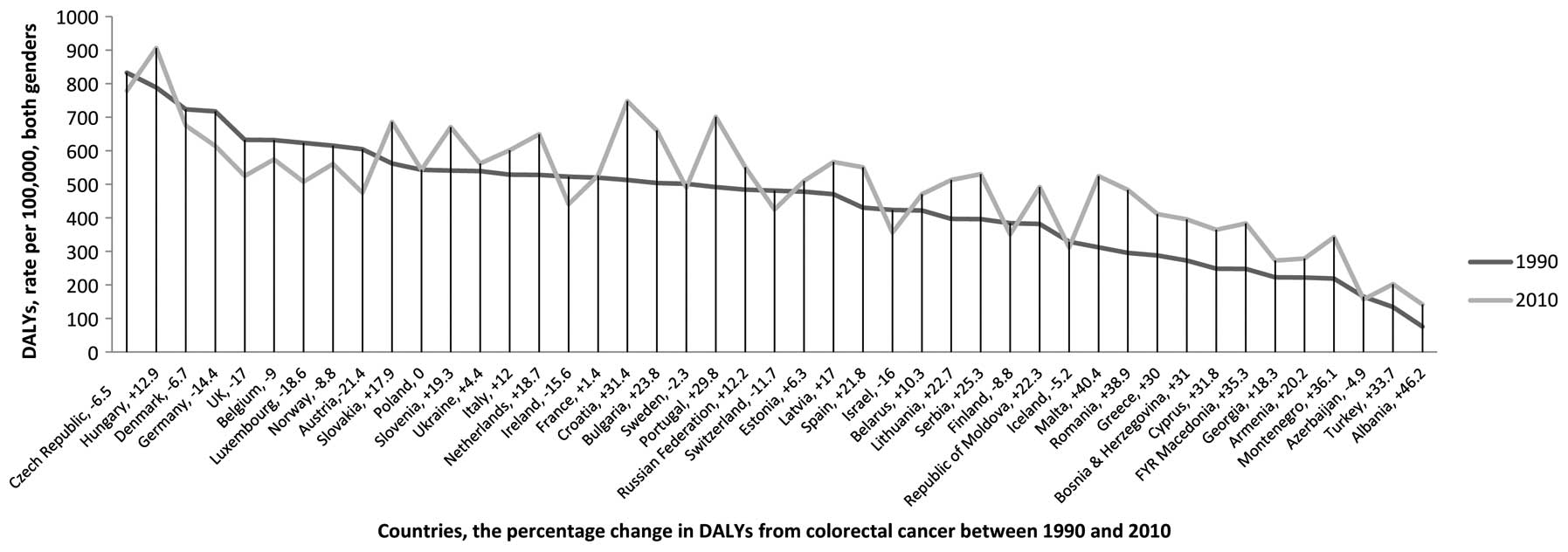
Ranking of DALYs due to colorectal
cancer across 45 European nations
Lithuania was in the group of 14 European countries
with the highest percentage increase in DALYs in males,
demonstrating an increase of 29.3% (Fig.
4). This group of 14 countries includes Serbia, the Republic of
Moldova, Bosnia and Herzegovina, Montenegro, Turkey, Cyprus,
Portugal, Greece, Croatia, FYR Macedonia, Albania, Romania and
Malta. Only 11 of the 45 European countries reduced the burden of
colorectal cancer in males in terms of DALYs between 1990 and 2010.
They are as follows, in descending order: Luxembourg; Finland;
Israel; the UK; Austria; Switzerland; Azerbaijan; Ireland; Norway;
Belgium; and Germany.
In females, Lithuania demonstrated one of the
highest increases, with an increase of 15.5% in the burden of
colorectal cancer from DALYs. In total, 17 countries reduced the
burden of colorectal cancer in terms of DALYs between 1990 and
2010. These countries were as follows: Austria, which demonstrated
the largest reduction of 32.4%; Germany; Ireland; the UK;
Luxembourg; Iceland; Belgium; the Czech Republic; Israel; Denmark;
Switzerland; Belarus; Norway; Estonia; Sweden; Ukraine; and
France.
The overall percentage increase in the national
burden of colorectal cancer for males and females over 20 years in
the Lithuanian population was 22.7%.
Ranking of YLDs due to colorectal
cancer across 45 European nations
In terms of male YLDs, Lithuania was ranked as 30th
in 1990 and 29th in 2010 out of the 45 European countries. For
female YLDs, Lithuania ranked slightly higher as 28th in 1990 and
27th in 2010. Over a 20-year period, every country, including
Lithuania demonstrated an increase in YLDs. Lithuania was ranked as
the 21st country in males in terms of this increase, and as the
18th country in females. For males and females combined, Lithuania
was ranked as the 20th country.
Ranking of YLDs across 12 European regions. The
number of YLDs per 100,000 individuals per year in Lithuania
increased by 22.4% between 1990 and 2010. However, Lithuania was
below the average of the Central and Eastern, Southern, Northern
and Western regions of Europe in 2010. It was also below the
average of Europe-45, EU-25, the original EU-15, the Nordic
countries, the Baltic countries, the UK and the block of countries
classified as democratic in 1990. In terms of YLLs per 100,000
individuals in 2010, Lithuania was above the average of the Central
and Eastern European countries, Western Europe, EU-25, EU-15, the
UK and the Baltic countries.
Discussion
The 30.6% increase in the overall crude incidence of
colorectal cancer in Lithuania between 2001 and 2011 indicates that
the incidence of colorectal cancer is likely to increase as the
proportion of elderly individuals within the population of the
Republic in Lithuania rises. Statistics taken in Lithuania reveal
that the life expectancy at birth in Lithuania was 68.53 years in
1994, the lowest expectancy within the last 50 years, and 73.62
years in 2011 (13).
In the present study, the varying incidence of
colorectal cancer between the regions of Lithuania was a notable
finding for such a small country with a population size of 2.986
million in 2012 and an area of 62,302 km2 (13). The incidence varied twofold between
certain counties and cities in Eastern and Western Lithuania. As
the changing age structure of the population is similar in all
Lithuanian regions, it was assumed that there are most likely
numerous factors contributing to this discrepancy in the overall
incidence rate of colorectal cancer in Lithuania at a particular
time point or over time. In terms of the ranking of
age-standardised incidence rates across European nations, the
age-standardised incidence of colorectal cancer was revealed to be
low in Lithuania compared with Western and Central European
countries.
The mortality rates due to colon cancer varied
considerably between the regions of Lithuania. Western Lithuania
was revealed to be possibly the most challenging region in
Lithuania as it demonstrates the lowest incidence of colorectal
cancer as well as the highest mortality rates.
In general, it was found that the overall
age-standardised mortality rate from colorectal cancer has
increased in Lithuania since 1990. A number of points are
noteworthy. First, the age-standardised mortality rate is higher in
males than females. Secondly, there is a marked difference in the
age-standardised mortality rates in males and females. Thirdly,
different data sources report different values for the
age-standardised mortality rates. This suggests that there are
several areas for improvement in the retrieval of oncological data
and statistics within Lithuania.
The assessment of DALYs presented a different
interpretation to that provided by conventional mortality
statistics, in which lung, prostate and stomach cancers are the
three leading causes of mortality from malignant diseases in the
Lithuanian male population (14). In
the present study, it appeared that colorectal cancer was the third
leading cause of the national burden of malignant disease in males
and females. Furthermore, when the top 10 causes of the global and
national burden of malignancies in Lithuania were compared and
ranked by gender and YLDs, it was revealed that colorectal cancer
is the second leading cause of disability (17.3%) preceded by
prostate cancer (28.1%) in males. In females, colorectal cancer was
ranked as the fourth highest contributor to disability, with 9.4%
of YLDs being due to this cancer.
In order to rank and define the performance of the
Lithuanian health service provision for colorectal cancer, the
geographic criteria were used for comparisons between European
nation and regions, in addition to the GBD traditional metrics.
When percentage change over the time was taken into account, it was
revealed that Lithuania is one of a group of countries with a
percentage increase in DALYs, and therefore YLLs, between 1990 and
2010. The percentage of DALYs rose by 22.7% between 1990 and 2010.
This increase was more pronounced in males than females, with
increases of 29.3 and 15.5%, respectively. This suggests that the
national burden of colorectal cancer in Lithuanian males was one of
the highest in Europe. Only countries in the Southeast region of
Europe, such as the Balkan Peninsula, demonstrated a higher
percentage increase. Each of the five neighbouring countries of
Lithuania, consisting of Poland, Latvia, Estonia, Belarus and the
Russian Federation, demonstrated a larger decrease in DALYS than
Lithuania. Estonia demonstrated a reduction DALYs in 2010, with a
percentage decrease of 7.5% in females.
Lithuania demonstrates a relatively low number of
YLDs due to colorectal cancer in comparison with other European
countries and regions of Europe. This is the most discouraging
finding of the present study, and suggests that novel therapeutic,
surgical and radiological technologies for colorectal cancer
management are not applied effectively in Lithuania (15). In addition, there is a substantial
opportunity to improve colorectal cancer management through
regionalisation, centralization and standardization. Finally, this
finding indicates that a national colorectal cancer prevention
programme is necessary in Lithuania.
This observational study demonstrates a number of
important limitations. The use of multiple sources of data and
estimates of the national burden of colorectal cancer is one
limitation. As the present study assessed primary and secondary
data, in addition to tertiary composite estimates, the
appropriateness of the method applied for the assessment of the
national burden of colorectal cancer may be disputable. In
addition, it was impossible to evaluate the impact of additional
risk factors and comorbid conditions on the mortalities due to
colorectal cancer. Overall, the issues with the provision of
colorectal cancer service in Lithuania may therefore be either
underestimated or overestimated. The ranking of the 45 European
nations may also be questionable due to the validity of the primary
data sources of certain developing European countries remaining
unknown.
In summary, the present study may provide a basis
for the acceleration of the development of the Lithuanian
colorectal cancer service and to implement long-term colorectal
cancer prevention and control programmes.
Acknowledgements
The present study is a part of the ‘Colorectal
cancer in Lithuania: mortality, morbidity and quality of life
study’ project. The project is kindly supported by the National
Research Council of Lithuania (grant no., LIG-01/2011). The authors
also thank the International Agency for Research on Cancer,
GLOBOCAN 2008 and the Global Burden of Diseases, Injuries, and Risk
Factors Study 2013 team.
Abbreviations:
|
GBD
|
global burden of disease
|
|
DALYs
|
disability-adjusted life years
|
|
YLLs
|
years of life lost
|
|
YLDs
|
years lived with a disability
|
|
NBD
|
national burden of disease
|
References
|
1
|
Murray CJL and Lopez AD: The global burden
of disease: a comprehensive assessment of mortality and disability
from diseases, injuries and risk factors in 1990 and projected to
2020. 1. Harvard University Press; Cambridge, MA: 1996
|
|
2
|
Wang H, Dwyer-Lindgren L, Lofgren KT, et
al: Age-specific and gender-specific mortality in 187 countries,
1970–2010: a systematic analysis for the Global Burden of Disease
Study 2010. Lancet. 380:2071–2094. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Murray CJ, Richards MA, Newton JN, Fenton
KA, Anderson HR, Atkinson C, et al: UK health performance: findings
of the Global Burden of Disease Study 2010. Lancet. 381:997–1020.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Highlights on health in Lithuania 2005.
World Health Organization; Geneva: pp. 7–8. 2006
|
|
5
|
Perlman S and Driver C; DALYs Working
Group, : Disability-adjusted life years (DALYs) in New York City.
New York City Department of Health and Mental Hygiene Epi Data
Brief. 11:2011.
|
|
6
|
Mathers CD, Vos T, Lopez AD, Salomon J and
Ezzati M: Planning a National Burden of Disease Study. In: National
Burden of Disease Studies: A Practical Guide. Edition 2.0. World
Health Organization; Geneva: pp. 16–23. 2001
|
|
7
|
Jayatilleke N, Pashayan N and Powles JW:
Burden of disease due to cancer in England and Wales. J Public
Health (Oxf). 34:287–295. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
World Health Organization, . Health
statistics and information systems. Disease and injury country
estimates: Burden of disease. http://www.who.int/healthinfo/global_burden_disease/estimates_country/en/index.htmlAccessed.
21– September. 2013
|
|
9
|
International Agency for Research on
Cancer, . World Health Organization. GLOBOCAN 2008: Cancer
Incidence and Mortality Worldwide. http://www.iarc.fr/en/media-centre/iarcnews/2010/globocan2008.phpAccessed.
24– Sepember. 2013
|
|
10
|
Ministry of Health of Lithuanian Republic,
. Institute of Hygiene Health Information Centre. http://sic.hi.lt/html/en/lhic.htm(In
Lithuanian). Accessed. 21– September. 2013
|
|
11
|
World Health Organization, . European
Detailed Mortality Database. http://datanew.euro.who.int/DMDBPHP5/caparams.phpAccessed.
21– September. 2013
|
|
12
|
Institute for Health Metrics and
Evaluation, University of Washington, . Global Burden of Diseases,
Injuries, and Risk Factors Study 2013. http://vizhub.healthdata.org/gbd-cause-patterns/Accessed.
21– September. 2013
|
|
13
|
Statistics Lithuania, . Official
Statistics Portal. Life Expectancy. http://osp.stat.gov.lt/en/statistiniu-rodikliu-analize?portletFormName=visualization&hash=e6729112-922a-475f-b90c-716dab8a2f26Accessed.
September 24–2013
|
|
14
|
Lithuanian National Cancer Institute, .
Lithuanian Cancer Registry. http://www.nvi.lt/index.php?-1413089819(In
Lithuanian). Accessed. September 24–2013
|
|
15
|
Poškus E, Mikalauskas S, Jotautas V,
Žeromskas P, Poškus T, Strupas K, et al: The pattern of colorectal
cancer surgery in Lithuania in 2005: do results meet expectations?
Medicina (Kaunas). 49:124–131. 2013.PubMed/NCBI
|