Introduction
Middle ear effusion is commonly observed in
otorhinolaryngological practice. Causes of middle ear effusion
include viral and bacterial infections, allergies and autoimmune
diseases, adenoid hypertrophy, functional abnormality of the
Eustachian tube, and gastroesophageal reflux syndrome (1,2). The
common symptoms of aneurysm include cochelar nerve damage,
tinnitus, hearing impairment, facial nerve and trigeminal nerve
palsy. Although computed tomography angiography (CTA) is clinically
more commonly utilized and is helpful in the treatment of this
condition, digital subtraction angiography (DSA) is the gold
standard for diagnosis. The therapeutic results of this combined
embolization technique approach have been good, with an 80%
survival rate (3). However, the
pathogenesis of middle ear effusion remains unclear.
The present study reports the rare case of a patient
who experienced recurrent middle ear effusion as a result of
compression of the Eustachian tube by a right-sided intrapetrous
carotid aneurysm. When middle ear effusion is the main presenting
symptom, as in the present case, the diagnosis may be delayed by
the common nature of this complaint. Awareness of this condition is
important in order to direct the clinician to perform angiography,
which is the definitive investigatory procedure. Once the diagnosis
has been established, treatment consists of endovascular coil
embolectomy under radiographic control or other surgical treatments
with, or without, subsequent reconstruction. Written informed
consent was obtained from the patient's family.
Case report
On May 7, 2011, a 13-year-old female presented to
Subei Hospital (Yangzhou, China) with a 6-month history of a
blocked ear sensation together with hearing loss in the right ear.
These symptoms were persistent and marked, but there was no history
of vertigo or otorrhea, and the patient had previously been well,
with no past medical history of ear disease or trauma. There was no
significant personal or family medical history. Upon examination,
the right tympanic membrane was dull and indrawn suggestive of a
middle ear effusion. The oropharynx showed first-degree enlargement
of the tonsils, and electronic nasopharyngoscopy showed adenoid
hypertrophy and oropharyngeal mucosal edema. Acoustic immittance
revealed a C curve in the left ear and a B curve in the right ear,
while pure tone audiometry in the right ear revealed 35-dB
conductive hearing loss, with a normal result in the left ear. The
provisional diagnosis of right-sided secretory otitis media with
adenoid hypertrophy was made on the basis of the previous clinical
findings and auxiliary examination. Next, right tympanostomy tube
placement and an adenoidectomy were performed under general
anaesthesia on the second day of admission to confirm the presence
of an effusion and allow ventilation. The post-operative period was
uneventful with a significant improvement in hearing. The patient
was discharged after three days. The follow-up examinations showed
no any sign of recurrence, therefore, the tube was removed after
six months.
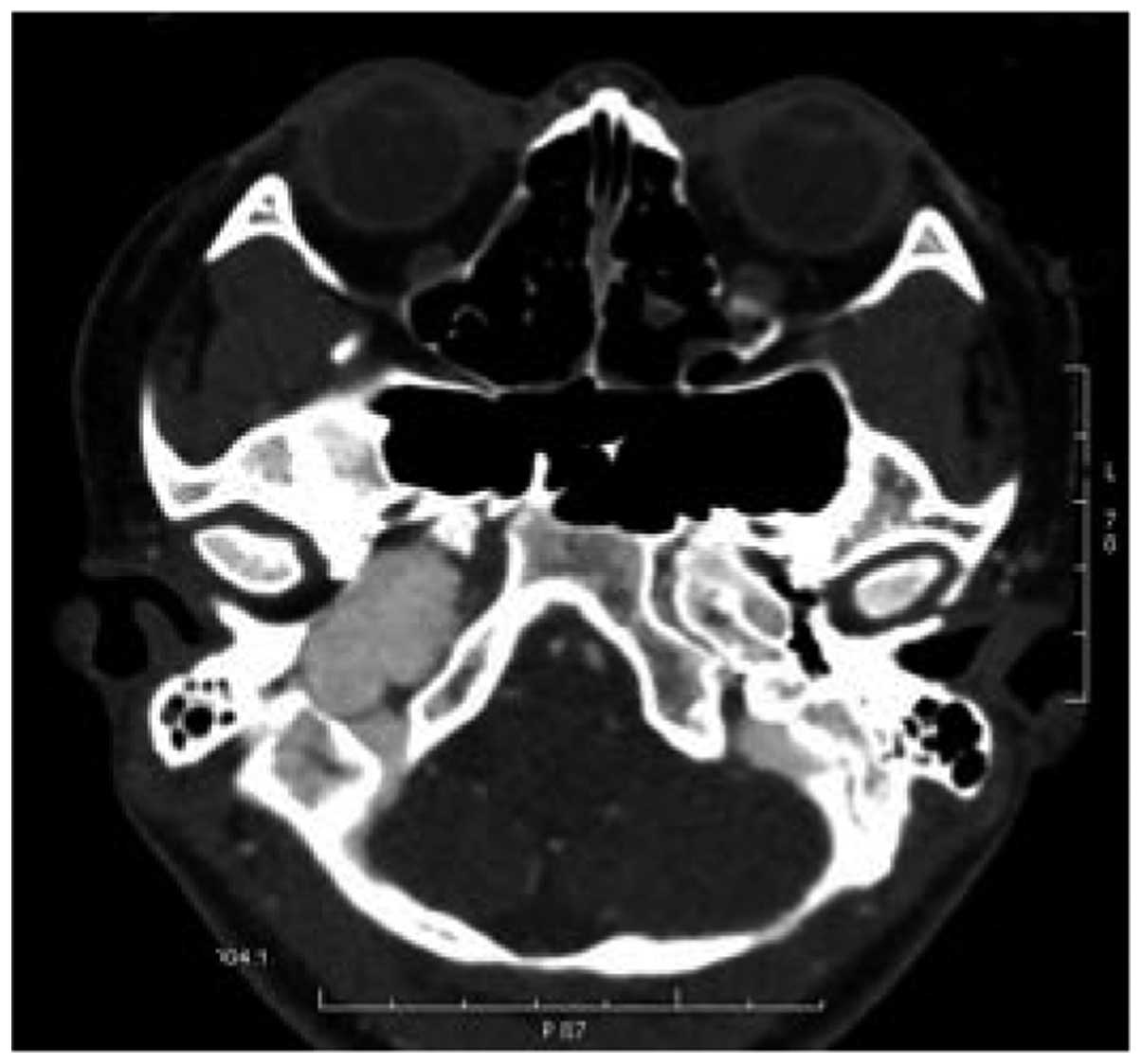
At 15 days post-tube removal, the patient again felt
a sensation of fullness in the right ear and experienced hearing
impairment. Upon examination, right middle ear effusion was
observed. Computed tomography (CT) of the temporal bone again
demonstrated middle ear effusion occupying the right side of the
attic (Fig. 1). Upon the basis of the
clinical findings and the imaging diagnosis, there was a strong
suspicion that a giant aneurysm was present in the region of the
right internal carotid artery. Accordingly, CTAwas performed, which
revealed an aneurysm of the petrous segment of the right internal
carotid artery, internal jugular vein compression with tortuous
dilatation of the tributaries and compression-induced distal
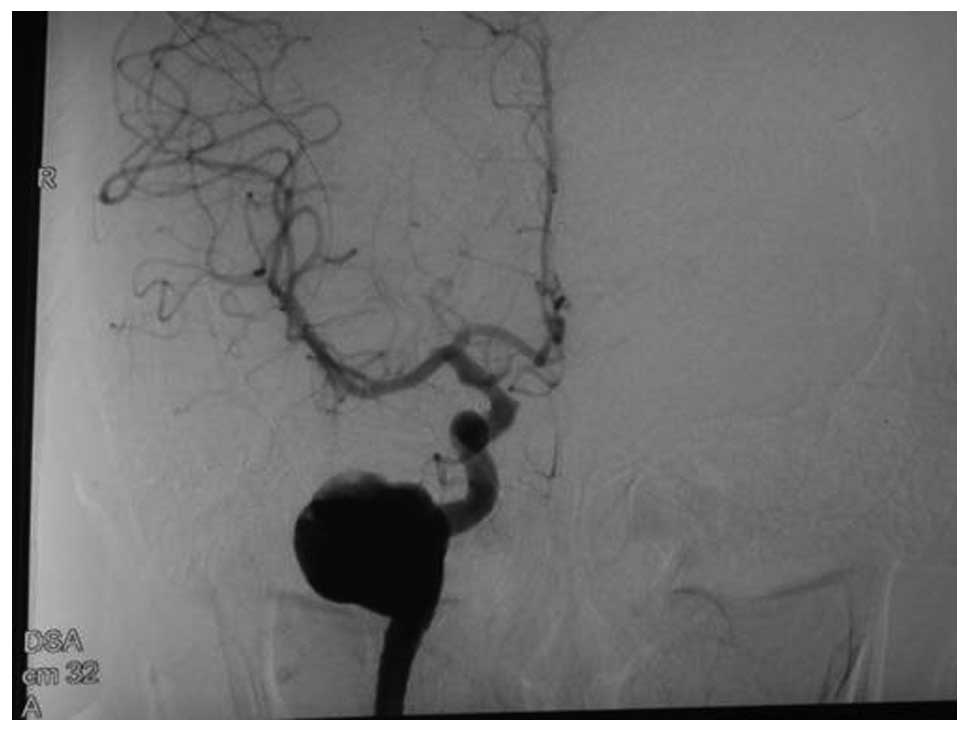
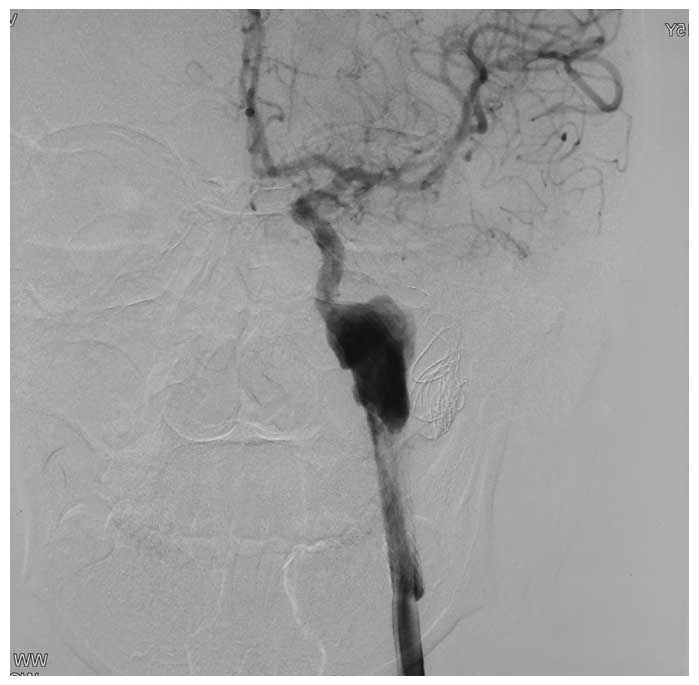
convoluted reflux disorder. The largest diameter of the aneurysm
was 25 mm (Fig. 2). DSA was performed
via a right femoral approach and an aneurysm of the intrapetrous
carotid artery with a size of 25×16 mm was confirmed (Fig. 3). The following therapeutic approaches
were considered on the basis of a consultation with the Department
of Neurosurgery: i) Embolization of the internal carotid artery
aneurysm, performed by placing a coil inside the aneurysm via a
catheter; ii) a right anterior craniotomy, followed by clipping of
the internal carotid artery aneurysm; iii) a craniotomy followed by
trapping of the artery. However, the patient was young and the
aneurysm was large in size. In consideration of these and other
facts, it was concluded that it would be dangerous to attempt
surgery by means of a craniotomy. It was thus decided that the best
approach was to perform a coil embolization using a catheter.
Initially, the patient and the patients family refused the
suggestion of any surgical procedures, including coil embolization,
due to the high risks of brain surgery. However, as a spontaneous
resolution was not likely, surgery was necessary, and the patient
accordingly underwent a successful right internal carotid
endovascular coil embolization (Fig.
4). During the procedure, a 6-French guiding catheter (90cm;
Boston Scientific, Fremont, CA, USA) was inserted into the right
internal carotid artery, a Prowler-14 microcatheter (Cordis
Neurovascular, Miami, FL, USA) was guided into the aneurysm and
seven orbit coils (Cordis Neurovascular) were released. The patient
made a satisfactory post-operative recovery and the aneurysm shrank
considerably (Fig. 5). During one
year of post-operative follow-up, the patient was completely
relieved of the middle ear effusion and the hearing level
demonstrated in the pure tone audiogram was preserved.
Discussion
Aneurysms of the internal carotid artery arising
within the petrous temporal bone are quite uncommon, and are
potentially serious occurrences that are difficult to detect and
treat. The causes of the formation of internal carotid artery
aneurysms include congenital factors, trauma, mastoid surgery,
pharyngeal and tonsillar infection, and corrosion from middle ear
disease. Brill et al (4)
hypothesized that childhood aneurysms can be linked to polycystic
kidney disease, collagen vascular disease, subacute bacterial
endocarditis, fibromuscular dysplasia, sclerosis, coarctation of
the aorta, Marfan's syndrome, syphilis, Ehler's-Danlos syndrome,
Moyamoya syndrome, and tuberous and mycotic disease. Such aneurysms
are generally congenital in nature (5).
Aneurysms of the internal carotid artery account for
all the ~40% of all aneurysms. The most common site of occurrence
is the posterior communicating artery, with other sites consisting
of the intracavernous internal carotid artery, the ophthalmic
artery, the internal carotid artery bifurcation and the anterior
choroidal artery (6). The incidence
of intrapetrous carotid aneurysms is lower than that of
non-traumatic intracranial aneurysms (7,8) Giant
aneurysms are more common in children than adults, comprising 31 to
45% of all childhood aneurysms (9,10). An
aneurysm size of >25 mm is defined as a giant aneurysm; these
occur more commonly in females than in males, and are most commonly
found in the connecting section of the cavernous sinus of the
internal carotid artery, at the end of the main artery bifurcation,
the basilar artery bifurcation and the vertebral basilar artery
(11). Aneurysms of the petrous
segment of the internal carotid are rare, particularly those with a
diameter of >25 mm, and among these, aneurysms with the initial
symptom of middle ear effusion are even more of a rarity. A
fundamental knowledge of the anatomy of the region is required so
that a good understanding of the development of the lesion can be
obtained (12). The carotid artery
passes vertically through the skull base into the periosteum-lined
carotid canal medial to the jugular foramen. The artery lies
anteromedial to the tympanic cavity and is separated anteriorly
from the Eustachian tube by a thin bony plate. The internal
auditory meatus lies posterosuperiorly. The clinical presentation
of intrapetrous aneurysms depends on the direction of extension.
When the aneurysms extend into the cavernous sinus, the symptoms
may include ptosis, diplopia, sixth-nerve paralysis and Horner's
syndrome. The symptoms associated with lateral extension of the
petrous aneurysm into the tympanic cavity include dizziness,
hearing loss, vertigo and pulsatile tinnitus (13). Such aneurysms may remain asymptomatic
until their expansion causes mechanical compression of adjacent
structures. Aneurysms is this section mainly present with the
symptoms of cochlear nerve damage, tinnitus in ~50% of patients,
hearing impairment and occasionally, facial and trigeminal nerve
palsy. The present study reports a case of a 13-year-old patient in
which the history and physical examination did not suggest the
symptoms of auditory nerve damage. Therefore, the cause of the
aneurysm in the present case was probably congenital in nature. The
patient has yet to develop any complications.
Methods for the diagnosis of internal carotid artery
aneurysms vary; a combination of CT, CTA, magnetic resonance
angiography and DSA may be diagnostic (14). Investigations with CT scans may
demonstrate erosion of the petrous temporal bone and effusion may
be observed within the middle ear and mastoid air cell system
following leakage. In the absence of effusion, such investigations
are often unremarkable and clinical judgement must be relied upon
to proceed to further analysis. The gold standard diagnostic
technique, however, remains as conventional selective carotid
angiography prior to therapeutic intervention. Angiography is
essential for establishing a final diagnosis and demonstrating the
shape, extent and origin of these aneurysms. At present, the use of
DSA is becoming more and more common, as it can reveal these
lesions accurately with much less risk of complications compared
with conventional arterial catheter angiography. In the present
case, the patient presented with middle ear effusion as the first
symptom, and examination revealed adenoid hypertrophy. Therefore,
it was originally believed that the middle ear effusion was caused
by adenoid hypertrophy. Thus, tympanostomy tube insertion and an
adenoidectomy were performed. The patient relapsed quickly after
the removal of the tube, which confirmed that the surgery was
ineffective. Next, relevant imaging examinations were performed,
which showed an aneurysm of the petrous segment of the right
internal carotid artery, temporal bone desorption due to
compression and expansive growth to the surrounding, leading to
compression of the Eustachian tube and causing tympanic cavity
effusion. This case suggests that in order to form a correct
diagnosis, diseases with rare etiology should be considered and the
examination should be performed in detail to avoid misdiagnosis and
incorrect treatment. Occasionally, middle ear exploratory surgery
without pre-operative angiography can result in disastrous results
(15). The differential diagnosis of
contrast enhancing parasellar masses mimicking an aneurysm in
children includes optichypothalamic gliomas, histiocytosis,
hamartomas and craniopharyngiomas (16).
Several treatments exist for carotid artery
aneurysms, including the following five (3): i) Suturing or clipping of the aneurysm
stalk; ii) reinforcement of the arterial wall encompassing the
aneurysm by coating it with a synthetic resin adhesive, or by
wrapping the aneurysm in fascia or gelatin; iii) intravascular
surgical therapy by means of coil embolization; iv) trapping and
clipping of the artery on each side of the aneurysm; and v)
suturing of the internal carotid artery in the neck region.
International studies on unruptured aneurysms have highlighted the
fact that the yearly rate of aneurysm rupture is significantly
higher in giant aneurysms than smaller aneurysms (17). Thus early interventions should be
implemented in cases of giant aneurysms. Direct clipping of the
aneurysm is the current gold-standard treatment. If the neck of the
aneurysm is wide and cannot be clipped directly then vascular
bypass grafting could also be considered (18). In the present patient, due to the
broad-based neck and embedding of the aneurysms in the temporal
bone, proximal vascular control was difficult to achieve safely
(bypass was also difficult) and direct clipping was less likely to
be successful. Thus, the best possible treatment approach was
spring coil embolization and internal carotid artery ligation. The
complication induced by these two methods was an insufficient local
cerebral blood supply. Application of internal carotid artery
ligatures is the most common method to be applied since 1990, but
this has been replaced by coil embolization and other techniques in
recent years, placing less burden on the patients (3). Ligation results in thrombosis from the
level of the interruption up to the origin of the ophthalmic
artery, thereby obliterating the aneurysm. It has been reported
that 30–60% of patients treated like this develop neurological
deficits and that approximately half of these will succumb
(19). Consequently, coil
embolization using a catheter was chosen as the method of choice in
the present study.
Intrapetrous carotid artery aneurysms occur rarely,
and should one present as middle ear effusion, delays in diagnosis
may result from the common nature of this complaint. Middle ear
effusion in the presence of a haemotympanum should alert the
clinician to the possibility of this condition. Whilst CT scans may
reveal the lesion, DSA is necessary for a definitive diagnosis and
delineation.
Acknowledgements
This study was supported by a grant from the Project
on Science and Social development of Jiangsu Province (no.
BE2012706).
References
|
1
|
Marshall BJ, Warren JR, Francis GJ,
Langton SR, Goodwin CS and Blincow ED: Rapid urease test in the
management of Campylobacter pyloridis-associated gastritis. Am J
Gastroenterol. 82:200–210. 1987.PubMed/NCBI
|
|
2
|
Cześnikiewicz-Guzik M, Karczewska E,
Bielański W, Guzik TJ, Kapera P, Targosz A, et al: Association of
the presence the Helicobacter pylori in the oral cavity and the
stomach. J Physiol Pharmacol. 55:105–115. 2004.PubMed/NCBI
|
|
3
|
Moro Y, Kojima H, Yashiro T and Moriyama
H: A case of internal carotid artery aneurysm diagnosed on basis of
massive nosebleed. Auris Nasus Larynx. 30:97–102. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Brill CB, Peyster RG, Hoover ED and Keller
MS: Giant intracranial aneurysm in a child with tuberous sclerosis:
CT demonstration. J Comput Assist Tomogr. 9:377–380. 1985.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Waga S and Tochio H: Intracranial aneurysm
associated with moyamoya disease in childhood. Surg Neurol.
23:237–243. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Liu CJ: Intracranial aneurysmCerebral
Vascular Surgery. 1st. Jiangsu Science and Technology Press;
Nanjing: pp. 282000, (In Chinese).
|
|
7
|
Benoit BG and Wortzman G: Traumatic
cerebral aneurysms. Clinical features and natural history. J Neurol
Neurosurg Psychiatry. 36:127–138. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sahs AL, Perret GE, Locksley HB and
Nishroka H: Intracranial aneurysms and subarachnoid hemorrhage: a
co-operative study. J.B. Lippincott; Philadelphia, PA: pp.
2961969
|
|
9
|
Amacher AL, Drake CG and Hovind L: The
results of operation upon cerebral aneurysms and angiomas in
children and adolescents. II. Cerebral angiomas. Childs Brain.
5:166–173. 1979.PubMed/NCBI
|
|
10
|
Storrs BB, Humphreys RP, Hendrick EB and
Hoffman HJ: Intracranial aneurysms in the pediatric age-group.
Childs Brain. 9:358–361. 1982.PubMed/NCBI
|
|
11
|
Hang ZX, Wang JB and Kong WJ: Cervical
vascular diseasesPractice of Otorhinolaryngology-Head and Neck
Surgery. People's Medical Publishing House; Beijing: pp. 6202008,
(In Chinese).
|
|
12
|
Leonetti JP, Smith PG and Linthicum FH:
The petrous carotid artery: Anatomic relations in skull base
surgery. Otolaryngol Head Neck Surg. 102:3–12. 1990.PubMed/NCBI
|
|
13
|
Hesselink JR and Weber AL: X-ray study of
the month Petrous carotid aneurysm. Ann Otol Rhinol Laryngol.
92:207–208. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Love MHS and Bell KE: Case report: Giant
aneurysm of the intrapetrous carotid artery presenting as a
cerebellopontine angle mass. Clin Radiol. 51:587–588. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Conley J and Hildyard V: Aneurysm of the
internal carotid artery presenting in the middle ear. Arch
Otolaryngol. 90:35–38. 1969. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Gum GK, Nadell JA, Numaguchi Y and
Robinson AE: Giant aneurysm of bilateral internal carotid arteries
in a child. Childs Nerv Syst. 4:161–163. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
International Study of Unruptured
Intracranial Aneurysms Investigators: Unruptured intracranial
aneurysms - risk of rupture and risks of surgical intervention. N
Engl J Med. 339:1725–1733. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Skrap M, Petralia B and Toniato G: Temory
balloon occlusion during the surgical treatment of giant
paraclinoid and vertebrobasilar aneurysm. Acta Neurochir (Wien).
152:435–442. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Dimtza A: Aneurysms of the carotid
arteries: report of two cases. Angiology. 7:218–227. 1956.
View Article : Google Scholar : PubMed/NCBI
|