Introduction
Multiple primary malignant tumors (MPMTs) are rarely
observed in clinical practice, however, certain fundamental factors
for the potential etiology have been described in the literature,
including the environment and behavior (tobacco, occupation,
pollution and ultraviolet light), genetic predisposition
(Li-Fraumeni or Beckwith-Wiedemann syndromes), previous medical
treatment (radiotherapy or chemotherapy) and complex interaction
between all these factors (1). The
association between varying cancer types can be classified into two
categories, which are dependent on the timing of their discovery.
An American review stated that the tumors are synchronous when the
cancers occur at the same time or within 2 months of each other,
whereas metachronous tumors occur when the cancers follow in
sequence more than 2 months apart (2). The most widely accepted definition is
that described by Moertel, which stated that synchronous neoplasms
may be defined as ≥2 primary neoplasms that are diagnosed within 6
months of each other, while metachronous neoplasms may be defined
as those detected following an interval of >6 months (3). These definitions are all based on the
time that the neoplasms are discovered rather than on the onset of
disease. MPMT was documented for the first time in a single patient
in a study by Billroth in 1889 (4).
The majority of MPMTs that occur in multiple organs are
metachronous, while the presence of synchronous lesions is less
common, and in accordance with the behavior of malignancy lesions,
these tumors are more frequent with aging. Ray et al
reported that 13.5% of patients with multiple primary malignancies
have genitourinary tumors (5). The
current study presents the case of a patient who developed primary
right renal cell carcinoma (RCC), and metachronous prostate and
left palatine tonsil neoplasms. To the best of our knowledge, this
combination of primary tumors has not previously been reported.
Case report
A 70-year-old male ex-smoker (20 to 30 cigarettes
per day from the age of 20 years old) was referred to the
outpatient office of the Urology Unit, Sapienza University of Rome
(Latina, Italy) with lower urinary tract symptoms due to benign
prostatic enlargement. The laboratory investigations were within
normal limits, with a prostate-specific antigen (PSA) level of 3.91
ng/ml (normal range: 0–4 ng/ml). The digital rectal examination
(DRE) was negative. The medical history revealed high blood
pressure and diabetes. The family history was negative for
malignancies. The ultrasound examination of the urogenital system
revealed nodular hyperplasia of the prostate and a right renal
mass. A full-body computed tomography (CT) scan was performed for
staging of the disease and showed a lesion with irregular contours
in the superior pole of the right kidney. The largest diameter of
the tumor was 11.5 cm. The CT scan also revealed lymphadenopathy in
the context of the hepatogastric ligament, coeliac artery and
interaortocaval region. The patient underwent right a radical
nephrectomy to remove the lesion, with a wedge resection.
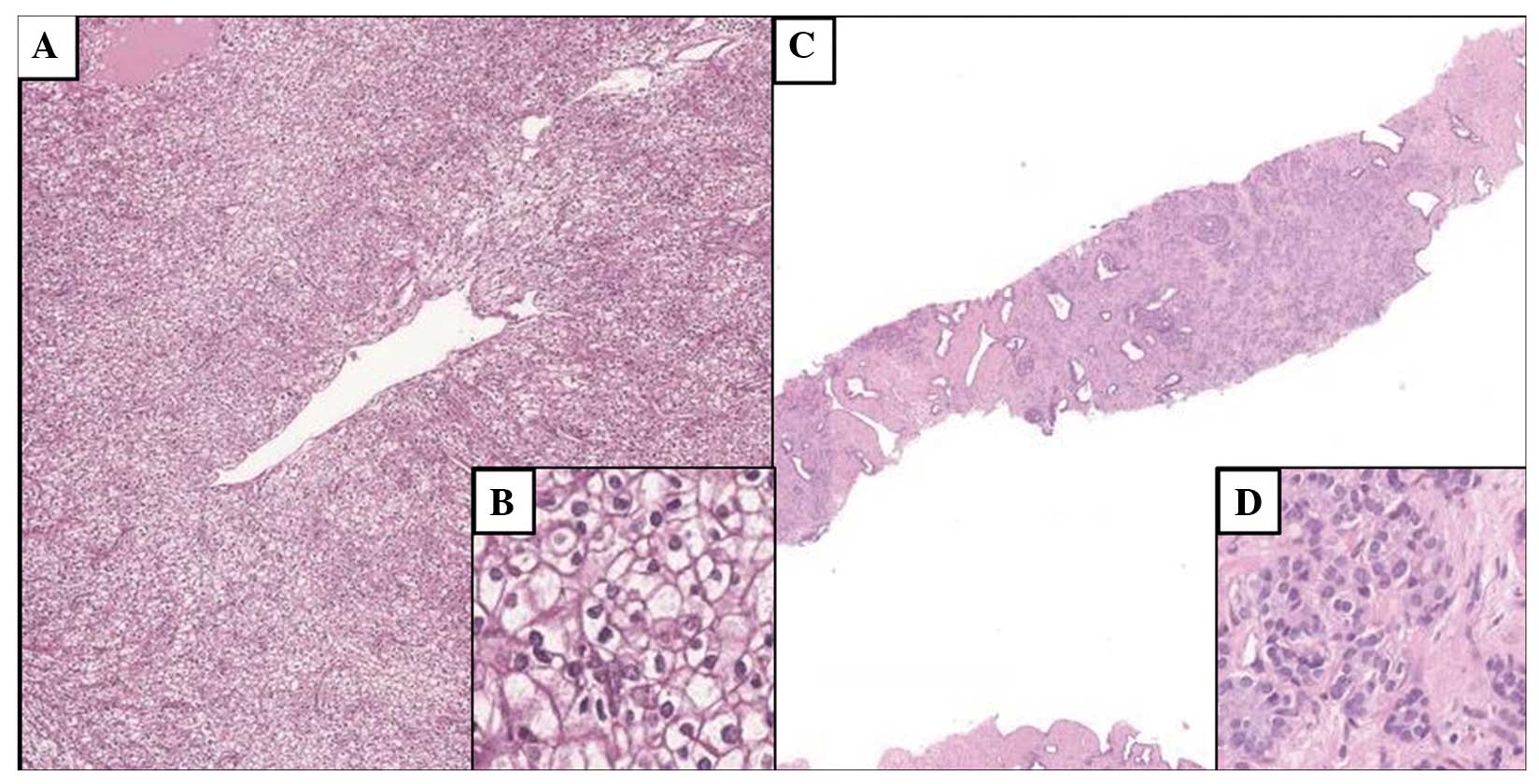
Pathological examination showed renal parenchyma infiltrate by the
proliferation of medium-large size cells with slightly irregular
nuclei, with the nucleoli easily visible, clear cytoplasm and
distinct cell membranes, organized in nest structures; the
diagnosis was renal cell carcinoma, clear cell type, nuclear
Furhman grade 2, with involvement of the renal vein and perinephric
fat (Fig. 1A and B). The tumor
pathological stage according to the American Cancer Committee Union
for International Cancer Control (2009) was pT2b (6).
At ~7 months after the kidney surgery, positron
emission tomography using
2-[18F]fluoro-2-deoxy-D-glucose, in combination with CT,
demonstrated a pathological cancer focus in the left palatine
tonsil. During a routine follow-up examination, a serum PSA level
of 5.93 ng/ml was detected. DRE was negative again and finally, a
transperineal ultrasound-guided sextant biopsy of the prostate was
performed. Histological examination of the tonsillar tissue
revealed a poorly-differentiated (G3) squamous cell carcinoma
(Fig. 1C and D).A histological
examination of the prostatic needle core biopsies showed a
proliferation of small/medium size glands, often fused, composed of
cellular elements with hyperchromatic nuclei, with evident
nucleolus, and slightly eosinophilic cytoplasm. The diagnosis was
adenocarcinoma of the prostate, Gleason score 8 (4+4) (Fig. 1C and D). The patient began a treatment
program with external beam radiotherapy (EBR; 70 Gy in 1.8 to 2.0
Gy fractions) and concurrent chemotherapy with carboplatin (target
AUC 2 on days 1, 8 and 15 for 6 cycles every 28 days) for the
palatine tonsil squamous tumor. Furthermore, at the end of the
tonsil cancer treatment, the patient is scheduled to start prostate
EBR and hormonal therapy with a luteinizing hormone-releasing
hormone agonist. The patient provided written informed consent for
publication of this case report.
Discussion
The incidence of MPMT is estimated to be between
0.73 and 11.7% (7). In order to
establish a definitive diagnosis of multiple neoplasms, the
criteria described by Warren and Gates in 1932 must be adhered to
(8). Each of the tumors must present
a definite picture of malignancy and each one must be distinct from
the other; the probability of one tumor being a metastasis of the
other must excluded (8). The present
case met the criteria set by Warren and Gates. The study reported a
patient who developed three distinct malignancies, all of which
originated from epithelial elements; the RCC, and metachronous
prostate and left palatine tonsil neoplasms occurred within a
period of <1 year. There were no predisposing factors for these
tumors, with the exception that the patient was a heavy smoker.
RCCs account for 90–95% of malignant neoplasms
arising from the kidney (9). The
Fuhrman histological classification system is the most widely
accepted for grading tumors. Identified etiological factors are
mainly associated with lifestyle, such as smoking status, obesity
and hypertension, however, the majority of patients do not present
with any specific symptoms (9). A
variety of factors, including tumor size and location, local or
distant spread, renal function, comorbidities and performance
status, must be considered when assessing the treatment for RCC
(9).
Prostate cancer is the most common neoplasm in
European men, particularly elderly men (10). In fact, 15% of male cancers are
prostate cancers in developed countries. Three well-established
risk factors are associated with prostate cancer, namely,
increasing age, ethnic origin and heredity. The Gleason score is
the recommended methodology for grading prostate cancer (10). Diagnostic techniques for prostate
cancer include DRE, analysis of serum PSA concentration and
transrectal ultrasound-guided biopsy. The diagnosis of prostate
cancer is based on the histological examination. The choice of
treatment depends primarily on the characteristics of the patient
and the stage of disease, and will vary for patients with low-,
intermediate- and high-risk prostate cancer (10).
Squamous cell carcinoma of the head and neck is
classified based on the following affected regions: Oral cavity,
oropharynx, nasopharynx, hypopharynx and larynx, with the tonsils
considered to be a subsite of the oropharynx (11). There is a strict association between
this tumor and tobacco use and alcohol consumption. Squamous cell
carcinoma of the oropharynx exhibits non-specific symptoms and the
rich lymphatic drainage of the tonsils is believed to promote early
spread (11). The diagnosis of tonsil
palatine cancer is based on histological examination. Treatment of
the head and neck cancer can consist mainly of radiation therapy,
surgery or surgery with radiation therapy as an adjunctive
treatment (11).
The incidence of MPMT is currently rising due to
improved diagnostic modalities and therapeutic protocols, which
result in a greater number of patients with cancer surviving long
enough to develop a second cancer. The incidence of cancer,
including MPMT, increases with age (12). With improvements in the survival rates
and the aging of the population, the frequency of individuals with
multiple cancers will increase in the future. Warren and Gates
(8) stated that the occurrence of a
first malignancy is a risk for a second malignancy in that
individual; in fact, the first neoplasm was likely initiated by
factors and agents that may initiate a second neoplasm as well.
Luciani and Balducci (12) recognized
two etiological hypotheses for MPMT: The inheritance of
predisposing genomic defects and field carcinogenesis. The first
theory concerns certain germ-line mutations that may result in
malignancies in multiple organ systems (such as xeroderma
pigmentosum) or in malignancies confined to one organ system (such
as familial polyposis coli). The second theory supports the
hypothesis that those organ systems with neoplasms are likely to
develop multiple and independent neoplasms, as all cells have been
exposed to the same dose of carcinogens for the same time. The
concept of field carcinogenesis can justify the association of
aging and multiple malignancies: The longer a person lives, the
greater the risk of developing tumors (12). Luciani and Balducci concluded that the
incidence of MPMT increases with the age; this increment does not
appear be caused by an aging phenotype, but rather it represents a
random event (12).
In a study on 1,425 patients with RCC, Beisland
et al (13) found that 16%
presented with only 1 tumor, 1.6% presented with 2 tumors and 0.2%
presented with 3 other primary malignancies. On average, 46.7% of
tumors occurred as metachronous tumors. The most common second
malignancy was prostatic cancer. This is in agreement with the
order of occurrence in the present patient. In the study by
Beisland et al (13), the
cumulative risk of developing second primary malignancy was found
to be as high as 26.6% in males with RCC. Therefore, it was
concluded that patients with RCC have a significantly higher risk
of developing further primary malignancies. Genetic, environmental
and dietary factors, as well as obesity, were indicated to be
etiological factors for the development of cancer of the prostate,
breast, kidney and colon (13). In
our previous studies, two cases of urinary tract synchronous
involvement from other malignancies were described. The first study
reported a case of synchronous primary tumors (bladder, breast and
skin) in a male patient (14), and
the second reported a case of synchronous ureteral and bladder
metastases from invasive ductal breast carcinoma in an elderly
female (15).
The present case highlights the fact that
synchronous or metachronous malignancies should be considered in
cases where a new tumor appears in a previous cancerous patient.
Since an association between RCC and other malignancies has been
shown in the literature, the present study poses the question as to
whether patients with renal cell carcinoma can have an increased
risk of subsequent second primary malignancy. To the best of our
knowledge, this is the first reported case in the literature of
this combination of primary neoplasms.
References
|
1
|
Rabbani F, Grimaldi G and Russo P:
Multiple primary malignancies in renal cell carcinoma. J Urol.
160:1255–1259. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Howe HL: A Review of the Definition for
Multiple Primary Cancers in the United States. Workshop Proceedings
From December 4–6, 2002. Princeton, New Jersey. North American
Association of Central Cancer Registries, Springfield, IL. May.
2003
|
|
3
|
Moertel CG: Multiple primary malignant
neoplasms: Historical perspectives. Cancer. 40 (Suppl):1786–1792.
1977. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Billroth T: Die allgemeine chirurgische
pathologie and therapie51 Vorlesungen-Ein Handbuch fur Studierende
and Artze, 14. Reimer G: Berlin: Auflage; 1889
|
|
5
|
Ray P, Sharifi R, Ortolano V and Guinan P:
Involvement of the genitourinary system in multiple primary
malignant neoplasms: A review. J Clin Oncol. 1:574–581.
1983.PubMed/NCBI
|
|
6
|
Moch H, Artibani W, Delahunt B, et al:
Reassessing the current UICC/AJCC TNM staging for renal cell
carcinoma. Eur Urol. 56:636–643. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Demandante CG, Troyer DA and Miles TP:
Multiple primary malignant neoplasms: Case report and a
comprehensive review of the literature. Am J Clin Oncol. 26:79–83.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Warren S and Gates O: Multiple primary
malignant tumors: A survey of the literature and a statistical
study. Am J Cancer. 16:1358–1414. 1932.
|
|
9
|
Ljungberg B, Cowan NC, Hanbury DC, et al:
EAU guidelines on renal cell carcinoma: The 2010 update. Eur Urol.
58:398–406. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Heidenreich A, Bastian PJ, Bellmunt J,
Bolla M, Joniau S, van der Kwast T, Mason M, Matveev V, Wiegel T,
Zattoni F and Mottet NEuropean Association of Urology: EAU
guidelines on prostate cancer. Part 1 Screening, diagnosis, and
local treatment with curative intent - update 2013. Eur Urol.
65:124–137. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Fort MM, Gathings R and Domanski MC:
Squamous cell carcinoma of the tonsil masquerading as a
peritonsillar abscess. Am J Emerg Med. 31:1002.e3–1002.e4. 2013.
View Article : Google Scholar
|
|
12
|
Luciani A and Balducci L: Multiple primary
malignancies. Semin Oncol. 31:264–273. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Beisland C, Talleraas O, Bakke A and
Norstein J: Multiple primary malignancies in patients with renal
cell carcinoma: A national population-based cohort study. BJU Int.
97:698–702. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Pastore AL, Palleschi G, Autieri D, Leto
A, Ripoli A, Maggioni C, Moschese D, Al Salhi Y, Porta N, Di
Cristofano C, Fuschi A, Silvestri L, Della Rocca C, Tomao S,
Petrozza V and Carbone ASapienza University of Rome, Faculty of
Pharmacy and Medicine: Synchronous primary neoplasms of the
bladder, skin and breast in a male patient: A case report. World J
Surg Oncol. 11:2822013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Pastore AL, Palleschi G, Tubaro A, De
Nunzio C, Stoppaciaro A, Silvestri L, Serafini GM, Stagnitti F and
Carbone A: Synchronous urinary tract metastases from breast cancer.
Urologia. 76:66–67. 2009.PubMed/NCBI
|