Introduction
Oral squamous cell carcinoma (OSCC) is the sixth
most frequently diagnosed type of cancer worldwide, and accounts
for 90% of all oral cancers (1,2).
Environmental factors including smoking, regular alcohol
consumption, a diet low in fruit and vegetables, and papillomavirus
infection are associated with the incidence of OSCC (2,3). A number
of genetic syndromes are also associated with OSCC, including
Li-Fraumeni syndrome, Fanconi anemia and lupus erythematosus
(4). In addition, certain oncogenes
have been identified to be activated in OSCC, such as c-Met, c-SRC
and Ras (5,6).
Receptor tyrosine kinases have crucial roles in
signal transduction during normal and malignant development, and
are involved in cellular proliferation, differentiation, migration
and apoptosis (7). The c-ros oncogene
1 (ROS1) is an orphan receptor tyrosine kinase proto-oncogene that
plays an important role in certain tumor types (7). The mechanisms underlying wild-type ROS1
protein expression and regulation in normal human tissues are yet
to be elucidated. In a previous study, ROS1 was undetectable in
normal heart, lung, ovary, pancreas, and testis tissues, was
expressed at low levels in parathyroid glands, eye, larynx, adrenal
gland and skeletal muscle tissues, and was strongly expressed in
the cerebellum, peripheric nerves, stomach, small intestine, colon
and kidney (8).
A number of point mutations and fusion events have
led to high ROS1 expression in a variety of tumor cell lines,
including non-small cell lung cancer, gastric carcinoma and
glioblastoma (7–11). In preclinical models, ROS1 fusions
have been demonstrated to correlate with sensitivity to tyrosine
kinase inhibitors, such as crizotinib (12–14).
As a number of receptor tyrosine kinases, including
c-MET, vascular endothelial growth factor receptor (VEGFR) and Akt
(15–18), are involved in OSCC, it can be
hypothesized that ROS1 may also be involved in the development of
OSCC. However, the presence of ROS1 in normal oral epithelium
tissues remains unknown.
The present study aimed to investigate the
expression of ROS1 in OSCC and in adjacent oral epithelium tissue
by immunohistochemistry (IHC). The associations between ROS1
expression and the pathological and clinical characteristics of
patients were also examined. Results of the present study may
provide new insight into the treatment of OSCC.
Materials and methods
Patients and samples
Archived formalin-fixed, paraffin-embedded surgical
tissue specimens from 31 OSCC patients were obtained from the
Department of Pathology of the Zhongshan Hospital, Fudan University
(Shanghai, China). The study population included 22 males and 9
females, with a mean age of 61.8 years (range, 47–88 years), who
had undergone surgery between January 2000 and December 2007. The
patients had not received chemotherapy, radiation therapy or any
other cancer therapy prior to surgery. Written informed consent was
obtained from each patient or the patient's family.
The sections were stained with hematoxylin and eosin
(H and E). The diagnoses and histological grading were established
according to the Broder's classification system (19,20). The
patients presented with well- (n=6), moderately- (n=20) and poorly-
(n=5) differentiated carcinomas. Details regarding lymph node
metastases, according to the tumor-node-metastasis (TNM)/Union for
International Cancer Control (UICC) criteria, were obtained from
the patients' medical records (21).
Follow-up assessment was based upon medical records and interviews
with patients/patients' families. The median follow-up period was
7.6 years, with all patients having at least a 5-year follow-up.
The study was approved by the ethics committee of the Zhongshan
Hospital, Fudan University (Shanghai, China).
Immunohistochemical analysis
IHC was performed using the EnVision™ peroxidase/3,
3′-diaminobenzidine (DAB) rabbit/mouse detection systems (Dako,
Glostrup, Denmark; catalog no. k4065). Initially, 4-µm sections
were deparaffinized in xylene, rehydrated in decreasing
concentrations of ethanol and then treated with 3% hydrogen
peroxide for 20 min at room temperature in order to block
endogenous peroxidase activity. Following this, the sections were
subjected to antigen retrieval by heating in a microwave in citrate
buffer (pH 6) for 20 min. The slides were then treated with 2%
normal goat serum (Abcam, Cambridge, MA, USA) and incubated
overnight with an anti-ROS1 antibody (Abcam; catalog no. ab5512;
dilution, 1:80) at 4°C. Subsequent to washing in phosphate-buffered
saline (PBS), the sections were incubated with biotinylated
secondary antibodies for 1 h, and staining was performed using ABC
reagents and DAB (provided with the EnVision™ kit). The slides were
counterstained with H and E for 5 min, and then dehydrated and
mounted. Negative controls, which were established by replacing the
primary antibody with PBS, showed no immunoreactivity.
Each case was evaluated independently by two
experienced pathologists who were blinded to the clinical data.
ROS1 immunoreactivity was analyzed by measuring the intensity of
staining and the percentage of positivity area. The staining
intensity was determined in a semi-quantitative manner as follows:
i) 0, negative; ii) 1, weak; iii) 2, moderate; and iv) 3, strong.
The area of positivity was calculated as a percentage of the total
tumor area as <10%, 10–89% or ≥90%. These two variables were
used to establish a final score as follows: i) score 0, negative or
intensity 1 staining with a <10% area; ii) score 1, intensity 1
with a 10–100% area or intensity 2 or 3 with a <10% area; iii)
score 2, intensity 2 with a >10% area or intensity 3 <90%
area; or iv) score 3, intensity 3 with a >90% area (22). The cytoplasmic ROS1 score was then
divided into two groups, negative/low: 0–1 and moderate/strong:
2–3, and the nuclear ROS1 expression was divided into two groups,
negative or low.
Cell culture and
immunofluorescence
The human oral cancer CAL-27 cells were obtained
from the Laboratory of Oral Oncology, The Ninth People's Hospital,
Shanghai Jiao Tong University School of Medicine (Shanghai, China).
The cells were maintained in Dulbecco's modified Eagle's medium
supplemented with 10% heat-inactivated fetal bovine serum (Gibco
Life Technologies, Carlsbad, CA, USA), and then cultured in a
humidified atmosphere of 5% CO2 at 37°C.
The CAL-27 cells growing on coverslips were fixed
with 4% (v/v) paraformaldehyde in PBS for 10 min, washed, and then
incubated for 1 h at room temperature with the primary anti-ROS1
antibody (dilution, 1:80; Abcam), which was diluted in a staining
solution of 0.5% (w/v) bovine serum albumin and 0.2% (w/v) saponin
in PBS. Subsequent to washing with PBS, the cells were incubated
for 1 h at room temperature with Alexa Fluor 555 goat anti-rabbit
immunoglobulin G (dilution, 1:1000; Cell Signaling Technology,
Inc., Danvers, MA, USA; catalog no. 4413), and then stained with
100 ng/ml of 4′,6-diamidino-2-phenylindole for 10 min (Invitrogen
Life Technologies, Carlsbad, CA, USA). The cells were then washed
and mounted onto slides with Fluoromount-G (SouthernBiotech,
Birmingham, AL, USA). All images were captured using a LSM 5 Pascal
confocal microscope (Carl Zeiss AG, Oberkochen, Germany) with
appropriate filters.
Statistical analysis
Statistical analyses were performed using SPSS
version 16.0 software (SPSS Inc., Chicago, IL, USA). The
normally-distributed data were compared using Student's
t-test, and are presented as the mean ± standard deviation.
The categorical variables are expressed as proportions, and were
compared using Fisher's exact test or Kruskal-Wallis test, as
appropriate. The Kaplan-Meier and log-rank test were used for the
survival analysis. The Cox regression analysis was used for the
multivariate survival analysis. A value of P<0.05 was used to
indicate a statistically significant difference.
Results
Expression patterns of ROS1 in OSCC
and adjacent epithelium
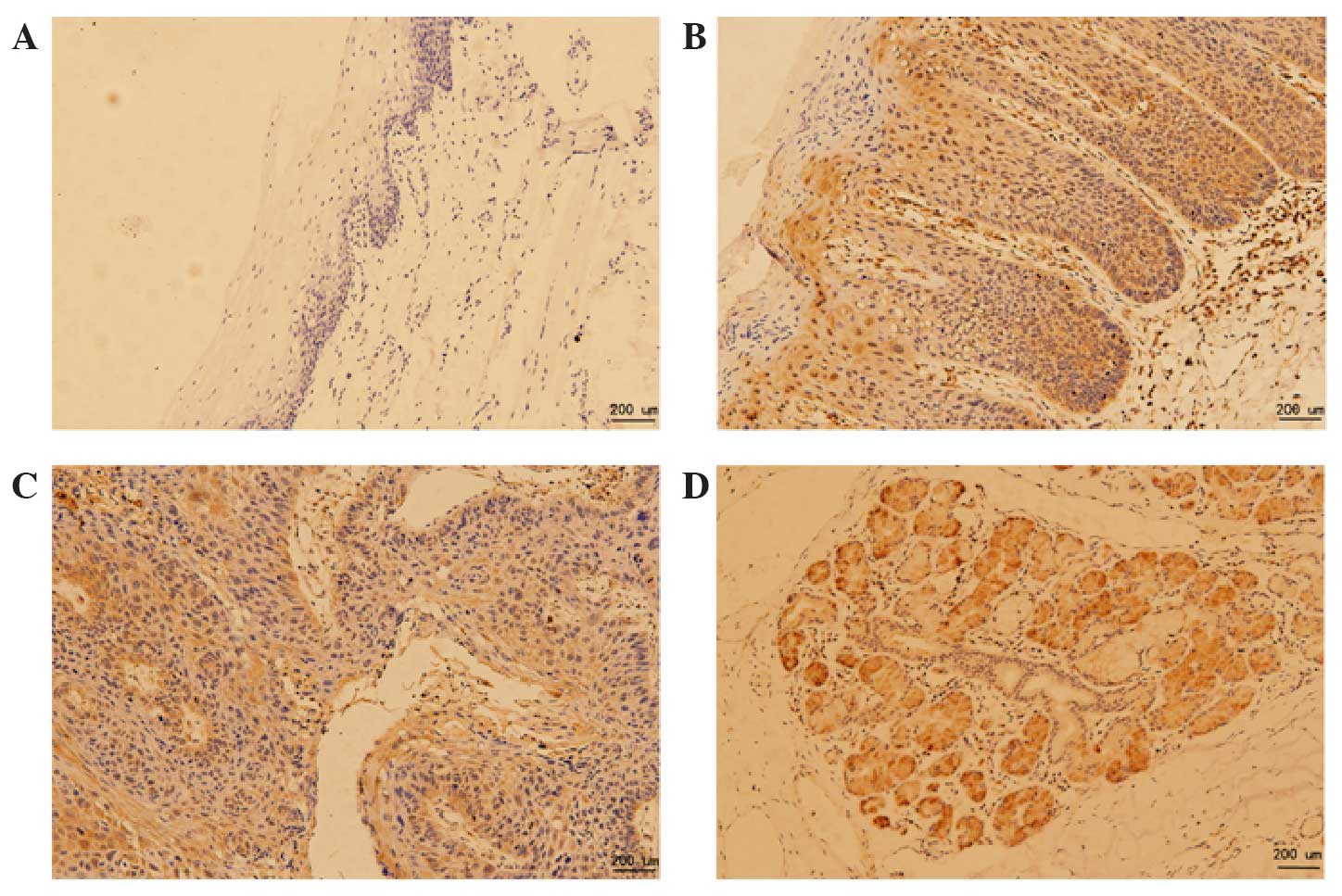
In total, 67.7% of the OSCC samples were positive
for cytoplasmic ROS1 expression (moderately or strongly; Fig. 1C). By contrast, none of the adjacent
normal epithelial samples (Fig. 1A)
were positive for cytoplasmic ROS1 (P=0.001; Table I). A certain amount of staining (2/16,
12.5%) was observed in the adjacent dysplastic epithelia (Fig. 1B and Table
I). In total, 80.6% of the OSCC samples, 75% of the adjacent
dysplastic epithelial tissues, and 18.8% of the adjacent normal
epithelial samples were negative for nuclear ROS1 expression
(Table I). Overall, only one of the
OSCC samples exhibited no ROS1 IHC staining.
 | Table I.Immunohistochemical evaluation of ROS1
in OSCC, adjacent dysplastic epithelial tissues and adjacent normal
epithelial tissues. |
Table I.
Immunohistochemical evaluation of ROS1
in OSCC, adjacent dysplastic epithelial tissues and adjacent normal
epithelial tissues.
|
|
| Cytoplasmic ROS1, n
(%) |
| Nuclear ROS1, n
(%) |
|
|---|
|
|
|
|
|
|
|
|---|
| Tissue | n | Negative/low | Moderate/strong | P-value | Negative | Low | P-value |
|---|
| OSCC | 31 | 10 (32.3) | 21 (67.7) | <0.001 | 25 (80.6) | 6
(19.4) | <0.001 |
| DE | 16 | 14 (87.5) | 2
(12.5) |
| 3
(18.8) | 13 (81.3) |
|
| NE | 8 | 8 (100.0) | 0
(0.0) |
| 6
(75.0) | 2
(25.0) |
|
Table II shows that
ROS1 was exclusively localized in the cytoplasm in 80.0% of the
OSCC samples, in the nucleus in 3.3% of the samples (one case), and
in the cytoplasm and nucleus in 16.7% of the samples. This gave a
total cytoplasmic localization of 96.7%. In the adjacent dysplastic
epithelial tissues, ROS1 was localized in the cytoplasm and nucleus
in 80.0% of the samples, in the cytoplasm alone in 13.3% of the
samples, and exclusively localized in the nucleus in 6.7% of the
samples (one case).
| Table II.ROS1 localization in OSCC and adjacent
dysplastic epithelial tissues. |
Table II.
ROS1 localization in OSCC and adjacent
dysplastic epithelial tissues.
|
|
| ROS1, n (%) |
|
|---|
|
|
|
|
|
|---|
| Tissue | n | Nucleus | Cytoplasm | Nucleus and
cytoplasm | P-value |
|---|
| OSCC | 30a | 1 (3.3) | 24 (80.0) | 5
(16.7) | <0.001 |
| DE | 15a | 1 (6.7) | 2
(13.3) | 12 (80.0) |
|
Positive ROS1 staining was observed in the normal
salivary gland cells (Fig. 1D).
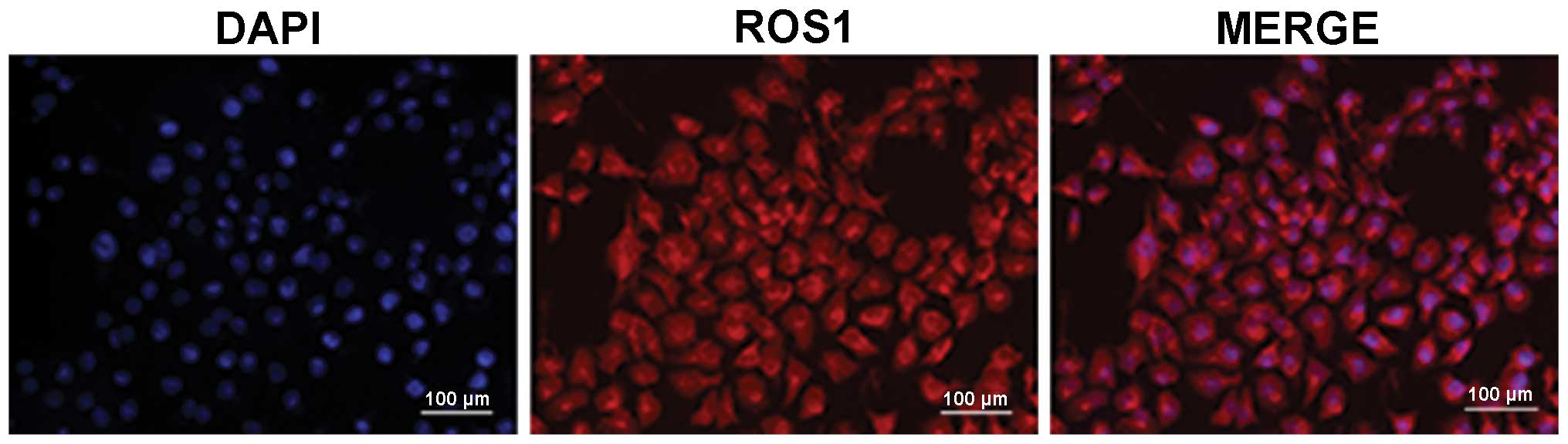
Confocal laser-scanning microscopy revealed nuclear and cytoplasmic
ROS1 staining in CAL-27 cells (Fig.
2).
ROS1 expression and its association
with the clinical and pathological characteristics of OSCC
patients
Table III shows the
clinicopathological characteristics of the patients according to
cytoplasmic ROS1 expression (negative/low vs. moderate/strong). No
significant associations were identified between cytoplasmic ROS1
expression and the clinical and pathological characteristics of
age, gender, differentiation, pathological nodal (N) stage and
clinical stage classification. Table
IV shows the clinicopathological characteristics of the
patients according to the nuclear ROS1 expression (negative vs.
low). The mean age was higher in patients with low nuclear ROS1
expression (72.5±10.8 vs. 59.2±10.7 years; P=0.01). No significant
associations were identified between nuclear ROS1 expression and
the clinicopathological characteristics of gender, differentiation,
pathological N stage and clinical stage classification (Table IV).
| Table III.Correlation between cytoplasmic ROS1
expression and clinicopathological characteristics. |
Table III.
Correlation between cytoplasmic ROS1
expression and clinicopathological characteristics.
|
|
| Cytoplasmic ROS1, n
(%) |
|
|---|
|
|
|
|
|
|---|
| Characteristic | n | Negative/low | Moderate/strong | P-value |
|---|
| OSCC, n | 31 | 10 (32.3) | 21 (67.7) |
|
| Age, mean ± SD,
years |
| 62.70±10.20 | 61.38±12.70 | 0.776a |
| Gender, n (%) |
|
|
|
|
|
Male | 22 | 8
(36.4) | 14 (63.6) |
|
|
Female | 9 | 2
(22.2) | 7
(77.8) | 0.677b |
| Differentiation, n
(%) |
|
|
|
|
|
Well | 6 |
0 (0.0) | 6 (100.0) |
|
|
Moderate | 20 | 9
(45.0) | 11 (55.0) |
|
|
Poor | 5 | 1
(20.0) | 4
(80.0) | 0.109b |
| Pathological N
stage, n (%) |
|
|
|
|
|
pN0 | 23 | 8
(34.8) | 15 (65.2) |
|
|
pN1+pN2+pN3 | 8 | 2
(25.0) | 6
(75.0) | 1.000b |
| Clinical stage
classification, n (%) |
|
|
|
|
|
I+II | 23 | 7
(30.4) | 16 (69.6) |
|
|
III+IV | 8 | 3
(37.5) | 5
(62.5) | 1.000b |
| Table IV.Correlations between nuclear ROS1
expression and clinicopathological characteristics. |
Table IV.
Correlations between nuclear ROS1
expression and clinicopathological characteristics.
|
|
| Nuclear ROS1, n
(%) |
|
|---|
|
|
|
|
|
|---|
| Characteristic | n | Negative | Low | P-value |
|---|
| OSCC, n (%) | 31 | 25 (80.6) | 6 (19.4) |
|
| Age, mean ± SD,
years |
| 59.24±10.69 | 72.50±10.77 | 0.011a |
| Gender, n (%) |
|
|
|
|
|
Male | 22 | 17 (77.3) | 5 (22.7) |
|
|
Female | 9 | 8
(88.9) | 1 (11.1) | 0.642b |
| Differentiation, n
(%) |
|
|
|
|
|
Well | 6 | 4
(66.7) | 2 (33.3) |
|
|
Moderate | 20 | 18 (90.0) | 2 (10.0) |
|
|
Poor | 5 | 3
(60.0) | 2 (40.0) | 0.145b |
| Pathological N
stage, n (%) |
|
|
|
|
|
pN0 | 23 | 20 (87.0) | 3 (13.0) |
|
|
pN1+pN2+pN3 | 8 | 5
(62.5) | 3 (37.5) | 0.161b |
| Clinical stage
classification, n (%) |
|
|
|
|
|
I+II | 23 | 20 (87.0) | 3 (13.0) |
|
|
III+IV | 8 | 5
(62.5) | 3 (37.5) | 0.161b |
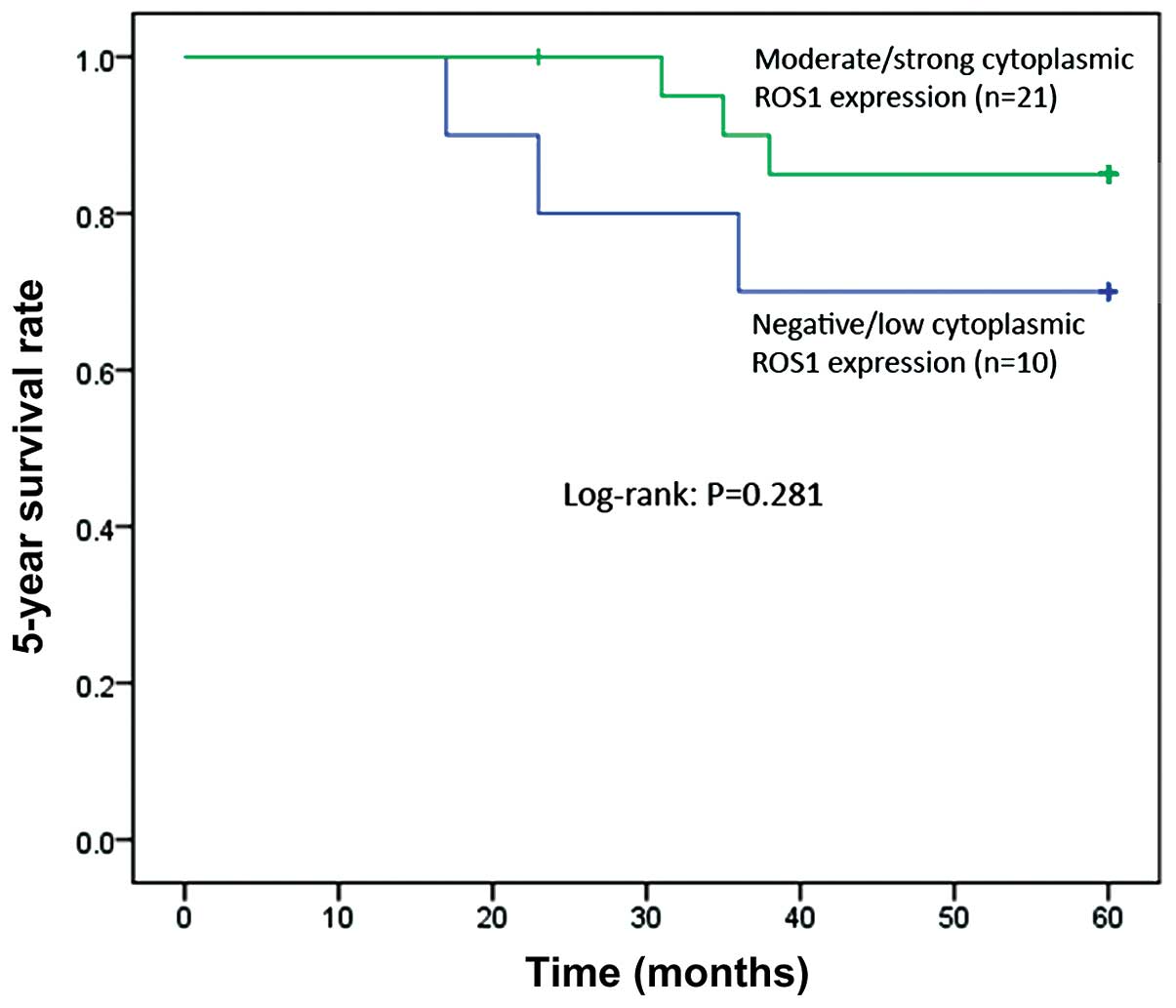
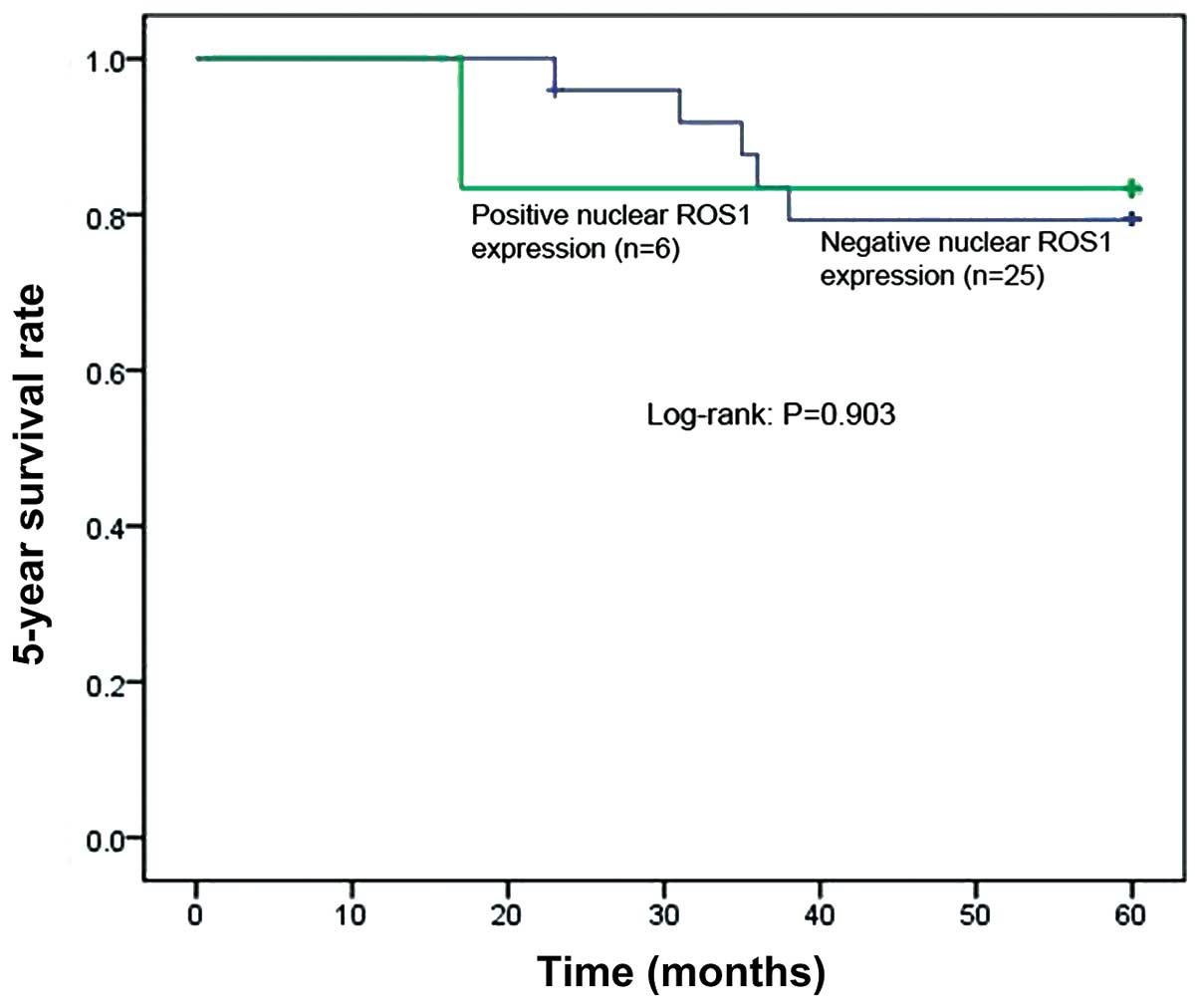
Survival analysis
No associations were identified between cytoplasmic
(P=0.28; Fig. 3) or nuclear ROS1
expression and the 5-year survival rates (P=0.90; Fig. 4). Furthermore, the multivariate Cox
analysis indicated that no factor was associated with 5-year
survival rates of the patients (Table
V).
| Table V.Multivariate Cox regression analysis
of the clinicopathological variables and 5-year survival of
patients with OSCC. |
Table V.
Multivariate Cox regression analysis
of the clinicopathological variables and 5-year survival of
patients with OSCC.
| Covariate | β coefficient | Hazard ratio | 95% confidence
interval | P-value |
|---|
| Age |
0.065 | 1.068 | 0.949–1.201 | 0.276 |
| Gender | −0.674 | 0.510 | 0.032–8.006 | 0.631 |
| Clinical stage
classification | 16.153 |
1.035×107 |
0.000–3.34×10150 | 0.924 |
| Pathological N
stage | 13.750 | 936653.769 |
0.000–2.96×10149 | 0.935 |
|
Differentiation | −0.592 | 0.553 | 0.079–3.854 | 0.550 |
| Nuclear ROS1 | −2.379 | 0.093 | 0.001–9.363 | 0.312 |
| Cytoplasmic
ROS1 | −0.540 | 0.583 | 0.077–4.436 | 0.602 |
Discussion
The present study aimed to analyze the expression of
ROS1 in OSCC samples, and investigate the association between its
expression and the clinicopathological parameters of OSCC patients.
ROS1 was predominantly localized in the cytoplasm of the OSCC
tissues. The expression of ROS1 was higher in the OSCC tissues than
in normal epithelial tissues adjacent to the tumor. No association
was identified between the 5-year survival rates and the
cytoplasmic or nuclear expression of ROS1.
A number of previous studies have investigated ROS1
expression in different tumor types (7–11).
ROS1 gene upregulation and/or mutation were primarily
detected in brain and lung cancers, but also in breast
fibroadenomas, liver, colon and kidney cancers, and in
chemically-induced stomach cancers (13). The aberrant expression, in addition to
the various mutant forms of ROS1, suggests a role for
ROS1 in tumorigenesis. The present study demonstrated that
the ROS1 protein was expressed in the majority of OSCC tissues and
in certain adjacent dysplastic epithelial tissues, but not in the
adjacent normal epithelial tissues. To the best of our knowledge,
the present study is the first to suggest a role for ROS1 in
OSCC.
The molecular architecture of the ROS1 protein
consists of an extracellular domain, a single transmembrane domain
and an intracellular region containing the carboxy-terminal
tyrosine kinase domain, which enables ROS1 to transduce signals
(23). Previous studies have
demonstrated that ROS1 is expressed in a spatial-, temporal- and
cell type-specific manner (9). In
addition, the staining pattern of ROS1 has been identified to
differ in different types of tumors. Cytoplasmic staining patterns
were observed in human non-small cell lung cancers (NSCLCs),
gastric adenocarcinomas, glioblastomas, HCC78 cells and U118MG
cells (11,24); membrane and cytoplasmic patterns were
evident in breast carcinomas, and membrane patterns were apparent
in hepatocarcinomas (25). The
factors responsible for these different localization patterns are
yet to be elucidated (24). However,
it is conceivable to hypothesize that different subcellular
localizations may have different roles during cancer development.
The IHC and immunofluorescence results of the present study
demonstrated similar diversity in the localization of ROS1.
Cytoplasmic staining was present in the majority of the OSCC
samples, while nuclear staining was more prominent in the adjacent
dysplastic epithelial tissues. By contrast, the adjacent normal
epithelial tissues exhibited no cytoplasmic ROS1 expression.
Previous data has established that ROS1 initiates
important signaling events during the differentiation of epithelial
tissues (9). In addition, ROS1
expression has been shown to be associated with the differentiation
of tumors, including gastric adenocarcinomas (11), astrocytomas (26), and invasive breast carcinomas
(25). Further studies are required
in order to address the function of ROS1 signaling in the context
of cell differentiation and transformation.
The present study did not identify any association
between the 5-year survival rates of patients and the cytoplasmic
or nuclear expression of ROS1. This result is in agreement with the
results of a previous study concerning gastric carcinomas (11), but contradict with a study that
examined breast carcinomas, which revealed improved survival with
increasing ROS1 expression (25), and
with a study that investigated cases of NSCLC, which demonstrated
poorer survival rates with increasing ROS1 expression (11). Previous studies that analyzed other
receptor tyrosine kinases, including c-MET, VEGF and Akt, revealed
that these receptors are involved in the development and prognosis
of OSCC (15–18). However, further studies are required
in order to assess the role of ROS1 expression in the survival of
OSCC patients.
The majority of the studies cited in the present
study have investigated the rearrangements of ROS1 genes in
human tumors, but not the wild-type ROS1 gene, or the ROS1
protein. Although several aberrant genomic changes in the
ROS1 oncogene are required in order for it to function as an
active oncogene (27), there is an
extremely low incidence of ROS1 gene rearrangement in human
tumors. This has been identified to be as low as 1.6% in cases of
NSCLC in China (8), and highest in
cholangiocarcinomas (8.7%) (10).
Further studies are required in order to elucidate the function of
ROS1 without any aberrant genomic change in
tumorigenesis.
The present study has certain limitations. Firstly,
the sample size was small. A larger number of patients may
therefore allow for the identification of further associations
between ROS1 expression and clinicopathological factors, in
addition to survival and prognosis. Secondly, the samples were
obtained from a single population, which could introduce a bias as
a result of the genetic background of this population. Finally, due
to the retrospective nature of the present study, the data was
limited to what was available in the medical charts. Therefore,
future studies should include a larger number of patients, and aim
to assess a full array of clinicopathological variables.
In conclusion, the present study revealed that there
was a high frequency of cytoplasmic ROS1 expression in OSCC
samples, whilst no expression in the adjacent normal epithelial
tissues. These results suggest that ROS1 is involved in the
pathogenesis of OSCC, and may therefore provide a novel therapeutic
target and prognostic tool for the treatment of OSCC.
Acknowledgements
This study was supported by a grant from the
National Natural Science Foundation of China (grant no.
81001202).
References
|
1
|
Koumaki D, Kostakis G, Koumaki V, et al:
Novel mutations of the HRAS gene and absence of hotspot mutations
of the BRAF genes in oral squamous cell carcinoma in a Greek
population. Oncol Rep. 27:1555–1560. 2012.PubMed/NCBI
|
|
2
|
Feller L and Lemmer J: Oral squamous cell
carcinoma: epidemiology, clinical presentation and treatment. J
Cancer Ther. 3:263–268. 2012. View Article : Google Scholar
|
|
3
|
Petti S: Lifestyle risk factors for oral
cancer. Oral Oncol. 45:340–350. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Scully C and Bagan J: Oral squamous cell
carcinoma overview. Oral Oncol. 45:301–308. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sen B, Peng S, Saigal B, Williams MD and
Johnson FM: Distinct interactions between c-Src and c-Met in
mediating resistance to c-Src inhibition in head and neck cancer.
Clin Cancer Res. 17:514–524. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Murugan AK, Munirajan AK and Tsuchida N:
Ras oncogenes in oral cancer: the past 20 years. Oral Oncol.
48:383–392. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Blume-Jensen P and Hunter T: Oncogenic
kinase signalling. Nature. 411:355–365. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Rimkunas VM, Crosby KE, Li D, et al:
Analysis of receptor tyrosine kinase ROS1-positive tumors in
non-small cell lung cancer: identification of a FIG-ROS1 fusion.
Clin Cancer Res. 18:4449–4457. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Acquaviva J, Wong R and Charest A: The
multifaceted roles of the receptor tyrosine kinase ROS in
development and cancer. Biochim Biophys Acta. 1795:37–52.
2009.PubMed/NCBI
|
|
10
|
Gu TL, Deng X, Huang F, et al: Survey of
tyrosine kinase signaling reveals ROS kinase fusions in human
cholangiocarcinoma. PLoS One. 6:e156402011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lee HJ, Seol HS, Kim JY, et al: ROS1
receptor tyrosine kinase, a druggable target, is frequently
overexpressed in non-small cell lung carcinomas via genetic and
epigenetic mechanisms. Ann Surg Oncol. 20:200–208. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Bergethon K, Shaw AT, Ou SH, et al: ROS1
rearrangements define a unique molecular class of lung cancers. J
Clin Oncol. 30:863–870. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
El-Deeb IM, Yoo KH and Lee SH: ROS
receptor tyrosine kinase: a new potential target for anticancer
drugs. Med Res Rev. 31:794–818. 2011.PubMed/NCBI
|
|
14
|
Davies KD and Doebele RC: Molecular
pathways: ROS1 fusion proteins in cancer. Clin Cancer Res.
19:4040–4045. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lo Muzio L, Leonardi R, Mignogna MD, et
al: Scatter factor receptor (c-Met) as possible prognostic factor
in patients with oral squamous cell carcinoma. Anticancer Res.
24:1063–1069. 2004.PubMed/NCBI
|
|
16
|
Maeda T, Matsumura S, Hiranuma H, et al:
Expression of vascular endothelial growth factor in human oral
squamous cell carcinoma: its association with tumour progression
and p53 gene status. J Clin Pathol. 51:771–775. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lim J, Kim JH, Paeng JY, et al: Prognostic
value of activated Akt expression in oral squamous cell carcinoma.
J Clin Pathol. 58:1199–1205. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Smith BD, Smith GL, Carter D, Sasaki CT
and Haffty BG: Prognostic significance of vascular endothelial
growth factor protein levels in oral and oropharyngeal squamous
cell carcinoma. J Clin Oncol. 18:2046–2052. 2000.PubMed/NCBI
|
|
19
|
Roland NJ, Caslin AW, Nash J and Stell PM:
Value of grading squamous cell carcinoma of the head and neck. Head
Neck. 14:224–229. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Akhter M, Hossain S, Rahman QB and Molla
MR: A study on histological grading of oral squamous cell carcinoma
and its co-relationship with regional metastasis. J Oral Maxillofac
Pathol. 15:168–176. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Sobin L, Gospodarowicz M and Wittekind C:
TNM Classification of Malignant Tumors. 7th. Wiley-Blackwell;
Oxford: 2009
|
|
22
|
Mrena J, Wiksten JP, Thiel A, et al:
Cyclooxygenase-2 is an independent prognostic factor in gastric
cancer and its expression is regulated by the messenger RNA
stability factor HuR. Clin Cancer Res. 11:7362–7368. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Chen JM, Heller D, Poon B, Kang L and Wang
LH: The proto-oncogene c-ros codes for a transmembrane tyrosine
protein kinase sharing sequence and structural homology with
sevenless protein of Drosophila melanogaster. Oncogene. 6:257–264.
1991.PubMed/NCBI
|
|
24
|
Charest A, Kheifets V, Park J, et al:
Oncogenic targeting of an activated tyrosine kinase to the Golgi
apparatus in a glioblastoma. Proc Natl Acad Sci USA. 100:916–921.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Eom M, Lkhagvadorj S, Oh SS, Han A and
Park KH: ROS1 expression in invasive ductal carcinoma of the breast
related to proliferation activity. Yonsei Med J. 54:650–657. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Mapstone T, McMichael M and Goldthwait D:
Expression of platelet-derived growth factors, transforming growth
factors and the ros gene in a variety of primary human brain
tumors. Neurosurgery. 28:216–222. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Jun HJ, Johnson H, Bronson RT, et al: The
oncogenic lung cancer fusion kinase CD74-ROS activates a novel
invasiveness pathway through E-Syt1 phosphorylation. Cancer Res.
72:3764–3774. 2012. View Article : Google Scholar : PubMed/NCBI
|