Introduction
At present, in the Japanese population the
proportion of elderly people is growing, while the birthrate is
declining (1). The World Health
Organization defines the elderly population as persons with a
chronological age of ≥65 years (2).
The statistics indicate that the proportion of people aged ≥65
years in the total Japanese population was 24.1% in 2010 (3). As recorded in the registry of the
Musculoskeletal Tumor Committee of the Japanese Orthopedic
Association, the incidence of malignant bone and soft tissue tumors
is increasing (4). Aging itself is a
strong predisposing factor for the development of numerous types of
malignant tumors (5); in addition,
the incidence of these tumors increases progressively with age
(6).
Aging has been reported to be an indicator of poor
prognosis in the treatment of bone and soft tissue tumors (6–8); in
general, this was thought to be due to reduced physiologic function
and a decreased general tolerance to cancer treatment in elderly
patients. The majority of orthopedic oncologists are likely to
select less invasive or conservative treatments for elderly
patients, especially for those with poor performance status
(8–13). However, due to recent developments in
multimodal medical technologies, including diagnostic modalities,
chemotherapy, anesthesia and surgical methods, more elderly
patients may be able to undergo surgery with a reduced risk than
has previously been the case (8–13). There
have been few previous studies concerning elderly patients with
primary malignant bone and soft tissue tumors (8–13). The aim
of the present study was to retrospectively analyze the clinical
outcomes of elderly patients diagnosed with these tumors and to
determine any potential prognostic factors.
Patients and methods
Patients
Clinical data was obtained from 90 patients, aged
≥65 years, with a diagnosis of primary malignant bone or soft
tissue tumors (bone, 20 cases; and soft tissue, 70 cases), treated
between March 1993 and May 2013 at the Department of Orthopedic
Surgery, Osaka City University Hospital Affiliated to Osaka City
University Garduate School of Medicine (Osaka, Japan). The data was
not fully analyzed until the last follow-up appointment in
September 2013. The study population consisted of 46 male and 44
female patients, with a mean age at diagnosis of 75.2±6.8 years
(range, 65–94 years). The median follow-up time in the present
study was 44.8 months (range, 1–163 months). The present study was
approved by the Institutional Review Board of Osaka City University
Graduate School of Medicine. Written informed consent was obtained
from all patients.
Patient diagnosis
On initial presentation to the Osaka City University
Hospital, patients underwent radiological evaluated using plain
radiographs, local computed tomography (CT) and magnetic resonance
imaging (MRI) with or without gadolinium enhancement. Distant
metastases to the lungs were also checked for using CT. Systemic
metastases were screened using fluorodeoxyglucose-positron emission
tomography (FDG-PET)/CT. Radiologically, if a malignant tumor was
suspected it was recommended that the patient underwent a biopsy
procedure. All biopsy specimens of resected tissues were diagnosed
by a pathologist with specialized training and expertise in sarcoma
pathology, using standard diagnostic criteria for bone and soft
tissue sarcoma subtyping (14). The
histological grade was determined according to the four grade
system for bone tumors (15) and
according to the Federation Nationale des Centres de Lutte Contres
le Cancer grading system for soft tissue tumors (16). The grading system for bone tumors,
with the exception of the Ewing sarcoma, was based on the technique
described by Broders (15). Grade 1
and 2 tumors were considered as low grade, and grade 3 and 4 tumors
as high grade. With regard to soft tissue tumors, Grade 1 tumors
were classified as low grade, and grade 2 and 3 tumors were
classified as high grade. The clinical staging of each patient was
evaluated in accordance with the American Joint Committee on Cancer
7th edition for soft tissue tumors and bone cancer (17,18).
Parameters
The following parameters were evaluated prior to
treatment: Age, gender, tumor depth, tumor site, tumor size, tumor
type (bone or soft tissue tumor), histological diagnosis,
histological grade, preoperative physical status using the American
Society of Anesthesiologists-Physical Status (ASA-PS)
classification (19) and oncological
outcome. Tumor size and location were estimated using MRI and/or
CT, and size was classified as <5 cm, 5–15 cm and >15 cm. The
ASA-PS scores were assessed by anesthesiologists regarding the
risks associated with surgery. Surgical margins of the resected
specimens were evaluated according to the guidelines of the
Japanese Orthopedic Association (20).
Patient follow-up
Following treatment, patients were generally
followed up at regular intervals of 3 months, with local
examination and chest radiographs or CT for the first 2 years post
treatment. Between 3 and 5 years post treatment, patients were
followed up every 6 months and yearly thereafter. MRI scans were
also conducted in order to supplement local examination for the
detection of local recurrence every 6 months for first 3 years
following treatment. Patients treated more recently were followed
up monthly, with physical examination for the first 3 months post
treatment and the last patient to undergo treatment in May 2013 was
followed up for 4 months. The follow-up time was defined as the
interval from the definitive tumor treatment (surgery or
radiotherapy) to the last follow-up.
Statistical analysis
Curves for the overall survival of patients with
sarcoma following treatment were plotted using the Kaplan-Meier
method (21). The log-rank test was
used to compare overall survival between the subgroups of patients
(22). The Cox proportional hazards
regression model was used to assess the ability of the patient
characteristics to predict overall survival (23). Univariate analysis was performed by
means of the log-rank test. Multivariate analysis was performed
using the Cox proportional hazards regression model, including only
factors where P<0.1 in the univariate analysis. In all analyses,
P<0.05 was considered to indicate a statistically significant
difference between values. The SAS system (SAS 9.3; SAS Institute,
Inc., Cary, NC, USA) was used throughout to perform the various
analyses.
Results
Clinical information
Clinical information for the elderly patients is
summarized in Table I. The median
patient age at the time of the initial visit to the Department of
Orthopedic Surgery, Osaka City University Hospital was 75.2 years
(range, 65–94 years); the study population consisted of 46 male and
44 female patients. Concerning the evaluation of preoperative
physical status, there were 21 patients who had associated
comorbidities with an ASA-PS score of ≥3; of note, cardiovascular
comorbidities, including hypertension, ischemic heart disease,
previous myocardial infarction and previous cerebrovascular
accident, accounted for a number of the total documented conditions
(19). The locations of bone tumors
were as follows: Femur, n=5; pelvis, n=5; rib, n=3; sacrum, n=2;
humerus, n=2; tibia, n=1; and scapula, n=1. The locations of soft
tissue tumors were the lower limb in 38 patients, trunk in 19
patients and upper limbs in 13 patients.
 | Table I.Clinical information for the elderly
patients. |
Table I.
Clinical information for the elderly
patients.
| Factors | Number |
|---|
| Age (years) |
|
|
65–74 | 43 |
| ≥75 | 47 |
| Gender |
|
| Male | 46 |
|
Female | 44 |
| Anatomical site |
|
|
Extremity | 59 |
|
Nonextremity | 31 |
| Tumor depth |
|
| Deep | 81 |
|
Superficial | 9 |
| Tumor size |
|
| 0–5
cm | 14 |
| 5–15
cm | 65 |
| >15
cm | 11 |
| Grade |
|
| Low | 27 |
| High | 63 |
| AJCC stage |
|
| Bone tumor |
|
| IA | 5 |
| IB | 3 |
| IIA | 6 |
| IIB | 4 |
| IVA | 2 |
| Soft
tissue tumor |
|
| I | 20 |
| II | 19 |
| III | 23 |
| IV | 8 |
| ASA-PS |
| 1 | 18 |
| 2 | 51 |
| 3 | 20 |
| 4 | 1 |
Histological diagnosis
Histological diagnosis of the patients is summarized
in Table II. Of the 20 bone
sarcomas, 12 were chondrosarcomas, 4 were osteosarcomas, 3 were
chordomas and 1 was a round cell sarcoma. Of the 70 soft tissue
sarcomas, 39 were liposarcomas, 11 were leiomyosarcomas, 7 were
myxofibrosarcomas, 6 were pleomorphic malignant fibrous
histiocytomas, 2 were malignant peripheral nerve sheath tumors and
there was 1 case each of fibrosarcoma, synovial sarcoma, malignant
solitary fibrous tumor, plasmacytoma and epithelioid sarcoma.
| Table II.Histopathology. |
Table II.
Histopathology.
| Tumor type | Number |
|---|
| Bone |
|
|
Chondrosarcoma | 12 |
|
Osteosarcoma | 4 |
|
Chordoma | 3 |
| Round
cell sarcoma | 1 |
| Soft tissue |
|
|
Liposarcoma | 39 |
|
Liomyosarcoma | 11 |
|
Myxofibrosarcoma | 7 |
|
Plepmorphic malignant fibrous
hystiocytoma | 6 |
|
Malignant periperal nerve
sheath tumor | 2 |
|
Fibrosarcoma | 1 |
|
Synovial sarcoma | 1 |
|
Malignant solitary fibrous
tumor | 1 |
| Soft
tissue plasmacytoma | 1 |
|
Epithelioid sarcoma | 1 |
Treatment of tumors
A total of 79 patients underwent surgical resection
of their tumors; of which, the surgical margins were evaluated as
being wide in 59 cases, marginal in 17 cases and intralesional in 3
cases. A further 11 patients did not receive surgery due to the
location of their tumors, which made resection difficult; in these
cases, preoperative evaluation indicated that they were in an
unsuitable condition for surgery or the patient opted not to
undergo surgery. A total of 5 patients received radiation therapy,
of which 3 underwent heavy particle beam therapy. A total of 4
patients received chemotherapy and the best supportive care was
selected for 2 patient. No patients underwent amputation or
disarticulation.
Oncological outcome
All patients were followed up at the Department of
Orthopedic Surgery, Osaka City University Hospital. The average
follow-up period was 44.8 months (range, 1–163 months). Regarding
oncological outcome at the last follow-up, 52 patients were in a
continuous disease-free condition, 8 demonstrated no evidence of
disease, 13 were alive with disease, 15 succumbed to the disease
and 2 mortalities occurred due to unassociated causes.
Prognostic factors
Univariate analysis revealed that ASA-PS was a
statistically significant prognostic factor for the overall
survival rate of patients (P=0.002) (Table III). In addition, using multivariate
analysis, ASA-PS was identified as a significant prognostic factor
(P=0.003), as was tumor grade (P=0.048) (Table IV).
| Table III.Cox proportional hazards univariate
analysis of overall survival. |
Table III.
Cox proportional hazards univariate
analysis of overall survival.
| Variable | Hazard for | Relative to | Hazard ratio
(CI) | P-value |
|---|
| Age | ≥75 years | 65–74 years | 2.05
(0.66–6.38) | 0.217 |
| Gender | Female | Male | 0.65
(0.24–1.76) | 0.402 |
| Depth | Deep | Superficial | 1.75
(0.28–13.3) | 0.592 |
| ASA-PS | ≥3 | 1–2 | 4.94
(1.79–13.6) | 0.002 |
| Grade | High |
Low/intermediate | 6.56
(0.86–49.8) | 0.069 |
| Table IV.Cox proportional hazards multivariate
analysis of overall survival. |
Table IV.
Cox proportional hazards multivariate
analysis of overall survival.
| Variable | Hazard for | Relative to | Hazard ratio
(CI) | P-value |
|---|
| ASA-PS | ≥3 | 1 and 2 | 5.77
(1.81–18.4) | 0.003 |
| Grade | High |
Low/intermediate | 7.82
(1.02–60.2) | 0.048 |
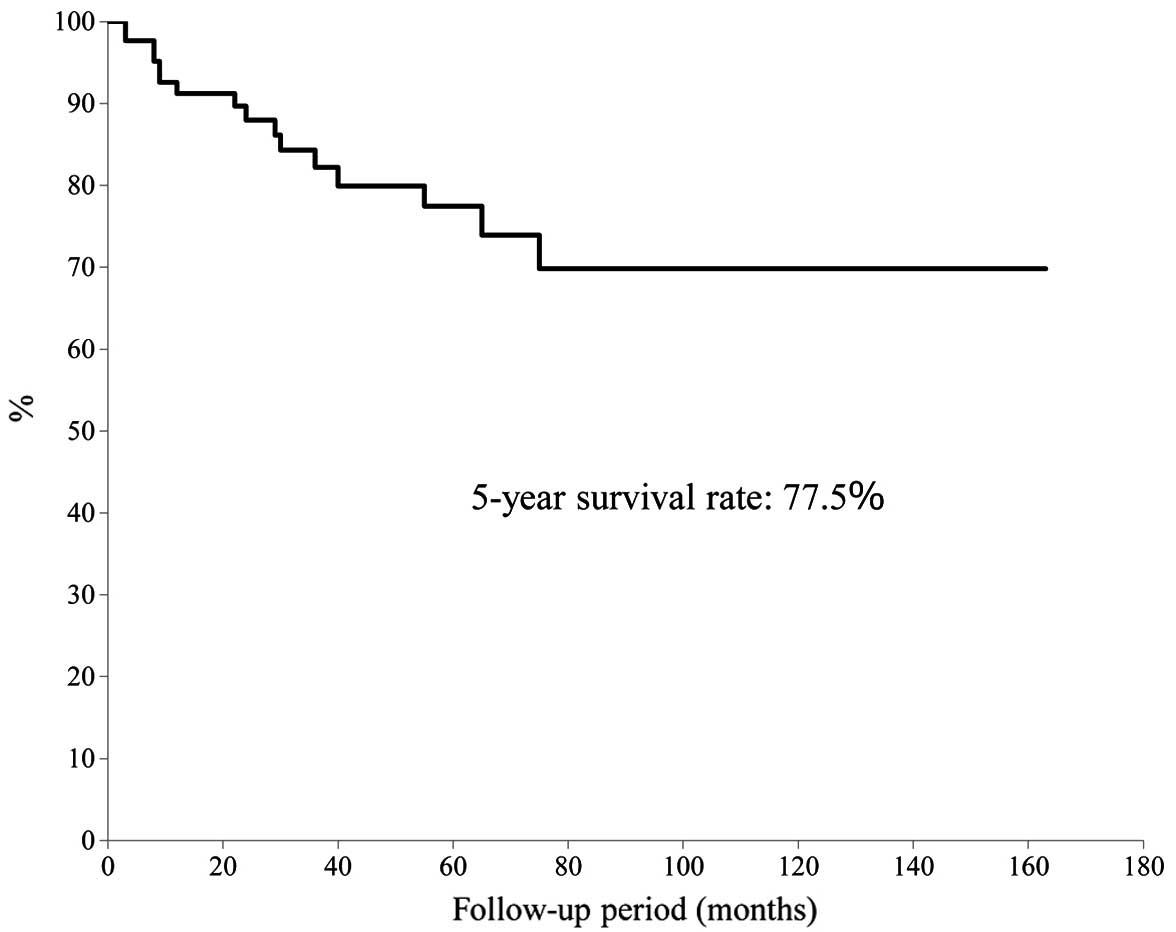
Survival rates
The 5-year overall survival rate was calculated
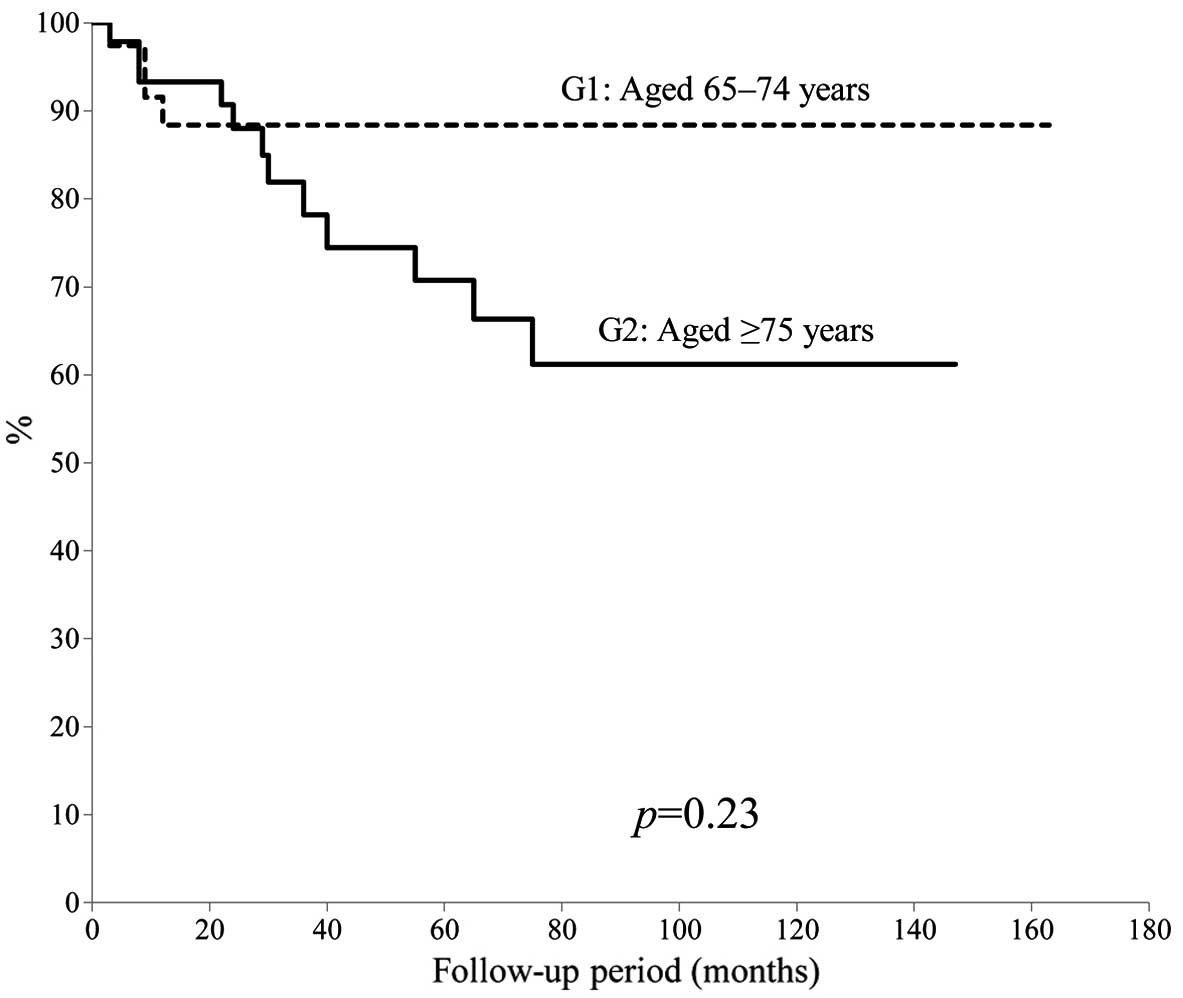
using the Kaplan-Meier survival curve to be 77.5% (Fig. 1). There was no significant difference
in 5-year overall survival between patients aged 65–74-years and
patients aged ≥75 years (P=0.23) (Fig.
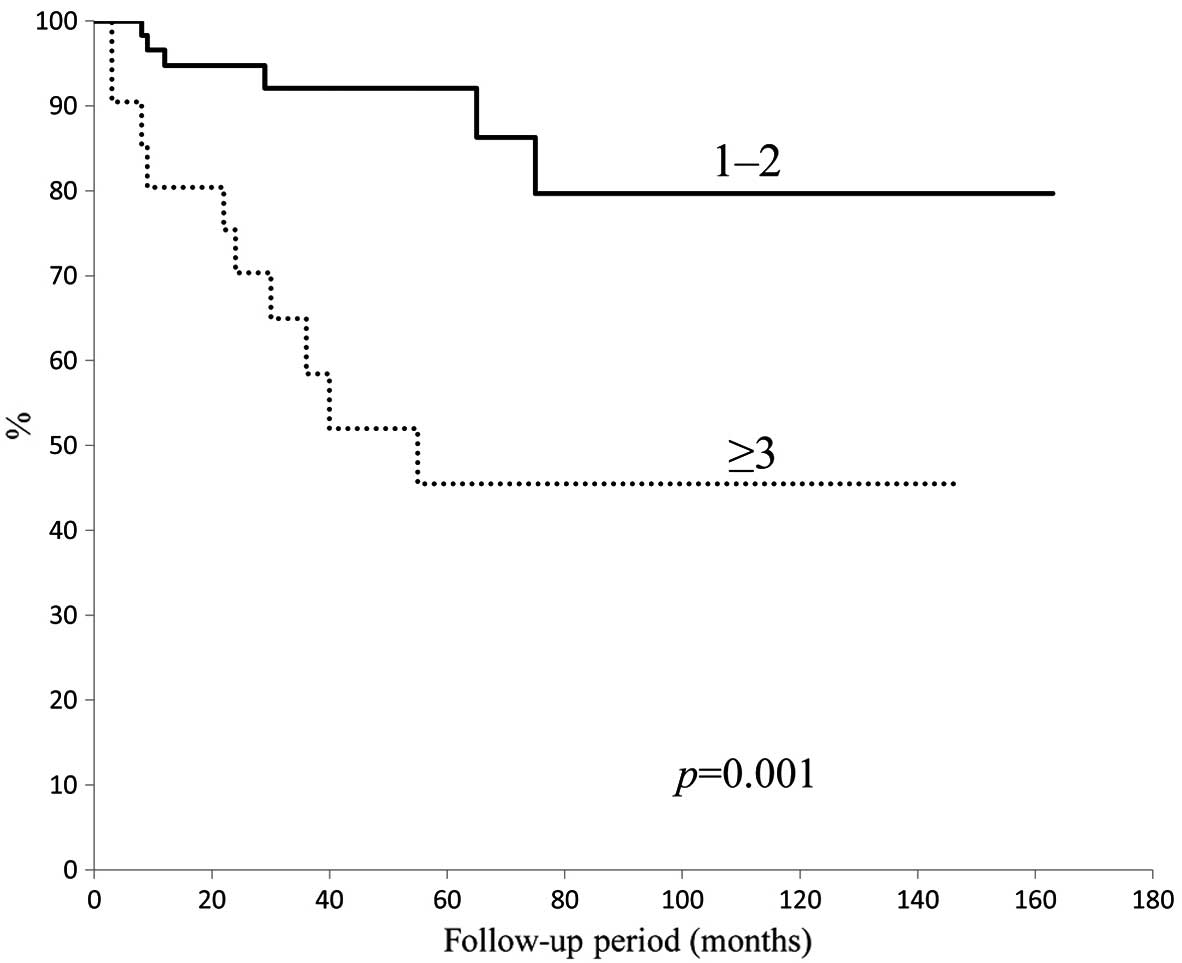
2). In addition, no significant difference was identified
between tumor types (bone vs. soft tissue sarcoma; P=0.43); by
contrast, a significant difference was observed for the ASA-PS
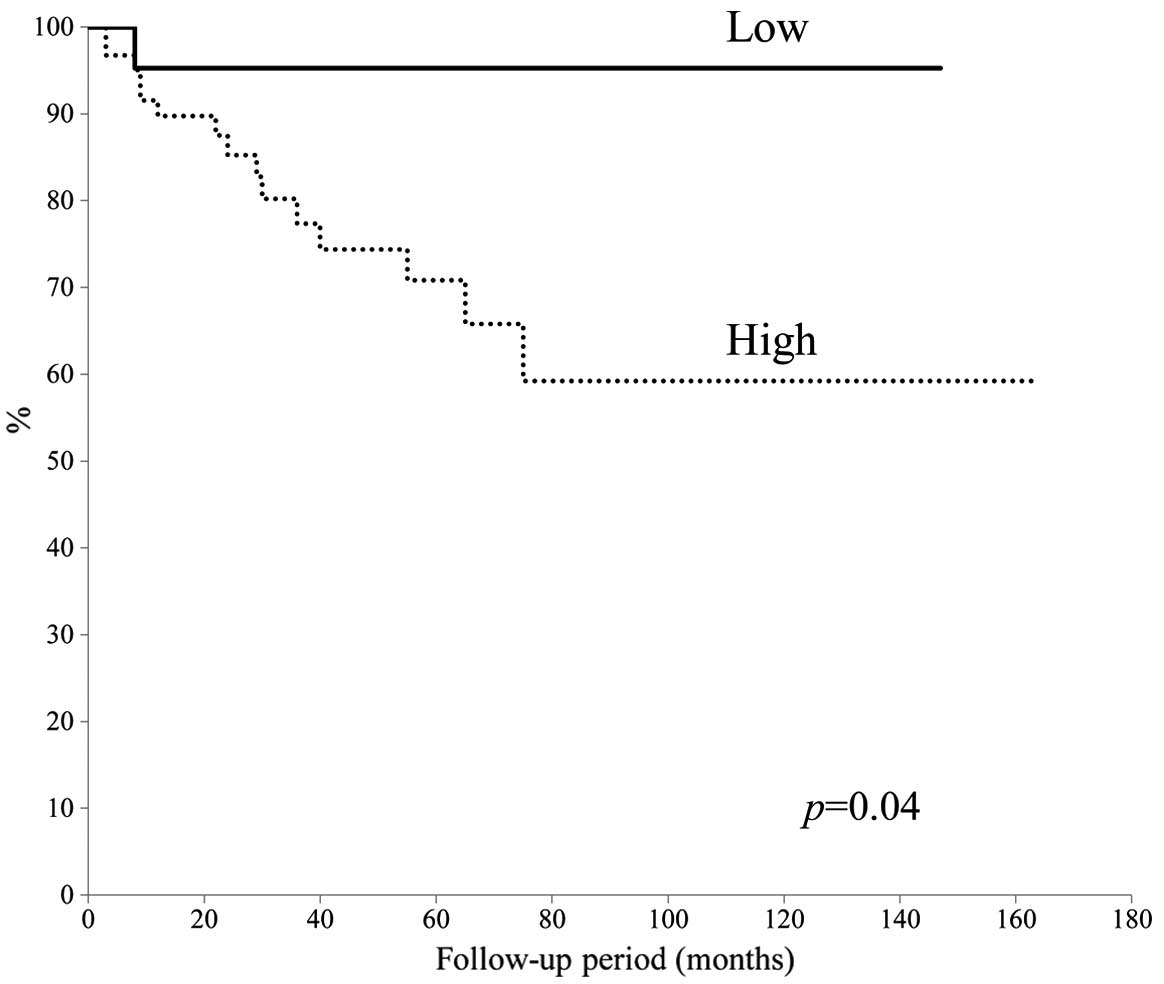
score (P=0.001) (Fig. 3) and tumor
grade (P=0.04) (Fig. 4). The 5-year
overall survival rate for patients with an ASA-PS score of ≥3 was
decreased compared with that for patients with ASA-PSs score of 1
and 2 (45.5 vs. 79.7%). Furthermore, the 5-year overall survival
rate for patients with a high-grade tumor was reduced compared with
that for patients with a low grade tumor (70.8 vs. 95.2%).
Discussion
In Japan, the number of elderly people in the
population has been increasing; of note, it was reported by the
Ministry of Health, Labour and Welfare of Japan that the average
life span is 79.64 years for males and 86.39 years for females
(3). Previously, various factors
associated with aging, including decreased performance status and
the presence of significant comorbidities, have caused surgeons and
medical oncologists to be cautious of using aggressive treatments
for elderly patients with malignant tumors. This is due to the
belief that an aggressive approach may have greater negative
effects on these patients compared with on younger patients
(24). However, with the development
of multidisciplinary modalities, there are increased possibilities
for aggressively treating elderly patients (25).
In the present study, it was demonstrated that the
5-year overall survival rate for elderly patients with primary
malignant bone and soft tissue tumors was 77.5%, which was
comparable to those reported in other previous studies. As shown in
Table V, Lahat et al (9) reported a 5-year disease-specific
survival of 63%, while Kozawa et al (12) reported that the 5-year overall
survival was 72% in elderly patients with bone and soft tissue
tumors. In addition, Yoneda et al (13) conducted a retrospective analysis
involving 158 elderly patients with localized soft tissue sarcoma
and found that the overall 5-year survival rate was 83%.
| Table V.Previous studies concerning the
treatment of elderly patients with bone and soft tissue tumors. |
Table V.
Previous studies concerning the
treatment of elderly patients with bone and soft tissue tumors.
| Author | Year | Age years | No. of
patients | Surgical
margins | Prognostic
factors | 5-year survival
rate (%) | Ref |
|---|
| Osaka et
al | 2003 | ≥65 | 25 | Wide (76%),
marginal (16%), intralesional (8%) | Age, grade | 79.6 | 8 |
| Boden et
al | 2006 | ≥80 | 50 | Clear margin
(76%) | Not identified | 46.0 | 10 |
| Lahat et
al | 2009 | ≥65 | 295 | Margin negative
(63.1%), margin positive (27.7%) | Age, tumor size,
grade | 63.0 | 9 |
| Torigoe et
al | 2010 | ≥70 | 14 | Wide and amputation
(85.7%), marginal (14.3%) | Bone tumor,
grade | 35.0 | 11 |
| Kozawa et
al | 2013 | ≥65 | 78 | Wide (71.8%),
marginal (11.5%), intralesional (3.8%) | Not identified | 72.0 | 12 |
| Yoneda et
al | 2013 | ≥70 | 158 | Adequate wide
(66.5%), inadequate wide (33.5%) | Male gender,
grade | 83.0 | 13 |
| Present study |
| ≥65 | 90 | Wide (65.5%),
marginal (18.9%), intralesional (3.3%) | ASA-PS, grade | 77.5 |
|
Surgical removal is the conventional treatment
method for malignant bone and soft tissue tumors and surgical
margins are considered to be an important factor regarding
curability (20). In the present
study involving elderly patients with malignant bone and soft
tissue tumors, a wide margin was achieved in 65.5%, a marginal
margin in 18.9% and an intralesional margin in 3.3% of patients.
Previous reports have also demonstrated that a surgical margin
without the achievement of a wide margin was evident in 14.3–33.5%
of patients (Table V). This indicates
that as a result of age-associated factors, orthopedic oncologists
have been obliged to select less aggressive surgery for patients
with malignant bone and soft tissue tumors.
In the present study, no patients underwent
amputation or disarticulation. This finding may be associated with
the Japanese culture, as the majority of elderly Japanese patients
and their families refuse to accept amputation, even if curability
may be accomplished with amputation; most of these patients choose
local radiotherapy to inhibit or control tumor growth as much as
possible.
Only 4 cases received systemic chemotherapy in the
present study. The European Society for Medical Oncology Guidelines
(26) state that adjuvant
chemotherapy may improve, or at least delay, distant and local
recurrence in high-risk patients. For elderly patients with
high-grade bone tumors, the use of chemotherapy is disputed.
Adriamycin and ifosfamide remain candidate chemotherapy drugs for
treating soft tissue tumors (27).
Elderly patients have been reported to suffer reduced cardiac
function and renal dysfunction in response to chemotherapy
(28,29). Therefore, it is thought that the use
of systemic chemotherapy should be limited to elderly patients free
of any health problems, due to reduced physiologic function.
The results of the present study indicated that an
ASA-PS score of ≥3 as well as the presence of a high-grade tumor
were significant predictive factors for poor prognosis. Tumor grade
has previously been accepted as being a predictive factor affecting
patient survival (Table V). As a
novel finding in the present study, ASA-PS proved to be a factor
that may be used to predict poor prognosis when evaluated using
univariate and multivariate analysis. Hosking et al
(19) reported that, when used as a
preoperative evaluation system for the general condition of elderly
patients, the ASA-PS score was associated with a poorer patient
survival rate (19). In the present
study, Kaplan-Meier analysis also revealed a significant difference
in patient survival between those with ASA-PS scores of ≥3 and 1–2.
It was therefore suggested that if the preoperative condition of
the patient is classified as an ASA-PS score 1 or 2, surgeons
should aim to resect of as much the tumor as possible, so that the
margin is as negative as possible. The concept of tumor removal may
be similar to that in young patients. If the ASA-PS score is ≥3,
the general condition of the patient and limb function following
tumor removal should be given priority and a less aggressive
treatment should be selected; radiotherapy is one potential
therapeutic option for the control of malignant tumors in these
patients.
The results of the present study confirmed that
there was no statistically significant difference in the 5-year
survival rate between patients' aged 65–74 years and those aged ≥75
years. Previously, the Surveillance Epidemiology and End Results
registries (7) demonstrated that
older age was associated with poor prognostic factors. Aging is
associated with decreased physiological functions and an increased
prevalence of comorbidities (30);
these factors may influence the management and outcome of
treatment. In Japan, life expectancy for individuals aged 65 years
is now 18.9 years for men and 23.9 years for women (1); these values are markedly increased
compared to those reported a decade earlier (1). These finding suggested that orthopedic
oncologists should reserve surgery exclusively for younger
patients.
The present study had several limitations; these
limitations include a small number of patients enrolled and that it
was a retrospective study performed in a single Japanese
institution. In addition, the follow-up period was relatively short
for a complete analysis of patient survival. Furthermore, no
specific guidelines have been established with regard to surgery,
chemotherapy and radiotherapy; thus, treatment plans were
determined by several orthopedic oncologists.
In conclusion, the number of elderly patients is
continuously increasing in Japan; accordingly, the incidence of
primary bone and soft tissue tumors has also been increasing. The
present study demonstrated as a novel finding that preoperative
risk assessment using the ASA-PS score as well as high tumor grade
were significant predictive factors of poor prognosis, whereas
older age was not a significant predictive factor. Thus, orthopedic
oncologists should not determine the aggressiveness of tumor
surgery based only on age.
References
|
1
|
Ministry of Health, Labor and Welfare of
Japan, . 2014 Statistics. Elderly people, natality, life
expectancy. http://www.mhlw.go.jp/toukei/saikin/hw/jinkou/geppo/nengai14/index.htmlAccessed.
30–April. 2014
|
|
2
|
World Health Organization, . Health
statistics and information systems definition of an older or
elderly person. http://www.who.int/healthinfo/en/Accessed.
30–April. 2014
|
|
3
|
Office for Policies on Cohesive Society, .
Cabinet Office, Government of Japan. http://www8.cao.go.jp/souki/index-eng.htmlAccessed.
30–April. 2014
|
|
4
|
Japanese Orthopedic Association
Musculoskeletal Tumor Committee, . Bone Tumor Registry and
Malignant Soft Tissue Tumor Registry in JapanJapanese
Musculoskeletal Oncology Group; Tokyo: 2008
|
|
5
|
Anisimov VN: The relationship between
aging and carcinogenesis: A critical appraisal. Crit Rev Oncol
Hematol. 45:277–304. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Balducci L and Erchler WB: Cancer and
aging: A nexus at several levels. Nat Rev Cancer. 5:655–662. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Al-Refaie WB, Habermann EB, Dudeja V,
Vickers SM, Tuttle TM, Jensen EH and Virnig BA: Extremity soft
tissue sarcoma care in the elderly: Insights into the
generalizability of NCI Cancer Trials. Ann Surg Oncol.
17:1732–1738. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Osaka S, Sugita H, Osaka E, Yoshida Y and
Ryu J: Surgical management of malignant soft tissue tumours in
patients aged 65 years or older. J Orthop Surg (Hong Kong).
11:28–33. 2003.PubMed/NCBI
|
|
9
|
Lahat G, Dhuka AR, Lahat S, Lazar AJ,
Lewis VO, Lin PP, Feig B, Cormier JN, Hunt KK, Pisters PW, et al:
Complete soft tissue sarcoma resection is a viable treatment option
for select elderly patients. Ann Surg Oncol. 16:2579–2586. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Boden RA, Clark MA, Neuhaus SJ, A'hern JR,
Thomas JM and Hayes AJ: Surgical management of soft tissue sarcoma
in patients over 80 years. Eur J Surg Oncol. 32:1154–1158. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Torigoe T, Terakado A, Suehara Y, Kurosawa
H, Yazawa Y and Takagi T: Bone versus soft-tissue sarcomas in the
elderly. J Orthop Surg. 18:58–62. 2010.
|
|
12
|
Kozawa E, Sugiura H, Tsukushi S, et al:
Multiple primary malignancies in elderly patients with high-grade
soft tissue sarcoma. Int J Clin Oncol. 19:384–390. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yoneda Y, Kunisada T, Naka N, Nishida Y,
Kawai A, Morii T, Takeda K, Hasei J, Yamakawa Y and Ozaki TJapanese
Musculoskeletal Oncology Group: Favorable outcome after complete
resection in elderly soft tissue sarcoma patients: Japanese
Musculoskeletal Oncology Group study. Eur J Surg Oncol. 40:49–54.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Flecher C, Unni K and Mertens F: Pathology
and genetics of tumours of soft tissue and boneWorld Health
Organization Classification of Tumours. Kleihues P and Sobin LH:
International Agency for Research on Cancer Press; Lyon: pp. 10–18.
2002
|
|
15
|
Broders AC: Squamous cell epithelioma of
the lip. A study of 537 cases. JAMA. 74:656–664. 1920. View Article : Google Scholar
|
|
16
|
Trojani M, Contesso G, Coindre JM, Rouesse
J, Bui NB, de Mascarel A, Goussot JF, David M, Bonichon F and
Lagarde C: Soft-tissue sarcomas of adults; study of pathological
prognostic variables and definition of a histopathological grading
system. Int J Cancer. 33:37–42. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Edge SB, Byrd DR, Compton CC, et al:
American Joint Committee on Cancer (AJCC): Soft tissue sarcomaAJCC
cancer staging manual. 7th. Springer; New York, NY: pp. 291–296.
2010
|
|
18
|
Edge SB, Byrd DR, Compton CC, et al: AJCC
boneAJCC cancer staging manual. 7th. Springer; New York, NY: pp.
281–290. 2010
|
|
19
|
Hosking MP, Warner MA, Lobdell CM, Offord
KP and Melton LJ III: Outcomes of surgery in patients 90 years of
age and older. JAMA. 261:1909–1915. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kawaguchi N, Ahmed AR, Matsumoto S, Manabe
J and Matsushita Y: The concept of curative margin in surgery for
bone and soft tissue sarcoma. Clin Orthop Relat Res. 419:165–172.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kaplan EL and Meier P: Nonparametric
estimation from incomplete observation. J Am Stat Assoc.
53:448–457. 1958. View Article : Google Scholar
|
|
22
|
Mantel N: Evaluation of survival data and
two new rank order statistics arising in its consideration. Cancer
Chemother Rep. 50:163–170. 1966.PubMed/NCBI
|
|
23
|
Cox DR: Regression models and life-tables.
J R Stat Soc. 34:187–220. 1972.
|
|
24
|
Takano S, Watanabe Y, Ohishi H, Kono S,
Nakamura M, Kubota N and Iwai S: Multimodality treatment for
patients with hepatocellular carcinoma: A single institution
retrospective series. Eur J Surg Oncol. 26:67–72. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Suemitsu R, Yamaguchi M, Takeo S, Ondo K,
Ueda H, Yoshino I and Maehara Y: Favorable surgical results for
patients with nonsmall cell lung cancer over 80 years old: A
multicenter survey. Ann Thorac Cardiovasc Surg. 14:154–160.
2008.PubMed/NCBI
|
|
26
|
ESMO/European Sarcoma, Network Working
Group, . Soft tissue, visceral sarcomas: ESMO clinical practice
guidelines for diagnosis, treatment and follow-up. Ann Oncol. 23
(Suppl 7):vii92–vii99. 2012.PubMed/NCBI
|
|
27
|
Linch M, Miah AB, Thway K, Judson IR and
Benson C: Systemic treatment of soft-tissue sarcoma-gold standard
and novel therapies. Nat Rev Clin Oncol. 11:187–202. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Farry JK, Flombaum CD and Latcha S: Long
term renal toxicity of ifosfamide in adult patients - 5 year data.
Eur J Cancer. 48:1326–1331. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Matushansky I, Dela Cruz F, Insel BJ,
Hershman DL and Neugut AI: Chemotherapy use in elderly patients
with soft tissue sarcoma: A population-based study. Cancer Invest.
31:83–91. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Vigorito C and Giallauria F: Effects of
exercise on cardiovascular performance in the elderly. Front
Physiol. 5:512014. View Article : Google Scholar : PubMed/NCBI
|