Introduction
Mutations in the epidermal growth factor receptor
(EGFR) gene are closely associated with the response of cells to
EGFR tyrosine kinase inhibitors (TKIs), including erlotinib and
gefitinib, particularly in lung adenocarcinoma. The incidence of
resistance to EGFR TKIs in patients with non-small-cell lung
carcinoma (NSCLC) is 10–20% (1).
Furthermore, clinical trials have revealed that oral EGFR TKIs may
lead to increased response rates and progression-free survival
rates compared with standard chemotherapies in patients with NSCLC
(2,3).
However, numerous patients with NSCLC eventually develop resistance
to these EGFR inhibitors. The T790M mutation in exon 20 of the EGFR
gene has been reported as one of the driving mutations for the
acquired resistance to gefitinib (4).
Approximately one-half of the patients that acquire resistance to
gefitinib are found to harbor the T790M EGFR mutation (5). In addition, 15–20% of NSCLC tumors
harbor mutations in exon 2 of the Kirsten rat sarcoma viral
oncogene homolog (KRAS) gene (6–8). As a
prognostic marker, KRAS mutations in resected NSCLC tissues have
been found to be associated with a shorter overall survival time
compared with patients with EGFR mutations. Although numerous
current studies suggest that EGFR and KRAS mutations are mutually
exclusive (9–11), as a downstream signal molecule of the
EGFR pathway, a mutation in KRAS may be a predictor for primary
resistance to TKI therapy in patients with NSCLC (12). Patients that harbor a KRAS mutation
and EGFR mutations in exons 21 and 20 are extremely rare.
Case report
A 69-year-old man that had smoked 10 cigarettes/day
for 20 years was admitted to The First Affiliated Hospital of Sun
Yat-Sen University (Guangzhou, Guangdong, China) in September 2011,
due to the presence of an abnormal shadow in the right upper lung
that was identified on chest X-ray. Physical examination revealed
no significant abnormalities. Chest computed tomography (CT)
revealed a 28×36 mm tumor in the upper lobe of the right lung,
which was classified as tumor-node-metastasis (TNM) stage T3N0M1.
Bronchoscopy revealed a tumor occluding the right upper bronchus,
with active bleeding. In order to relieve the respiratory symptoms
that resulted from hemoptysis, the patient underwent lobectomy of
the right upper lung and mediastinal lymph node dissection. The
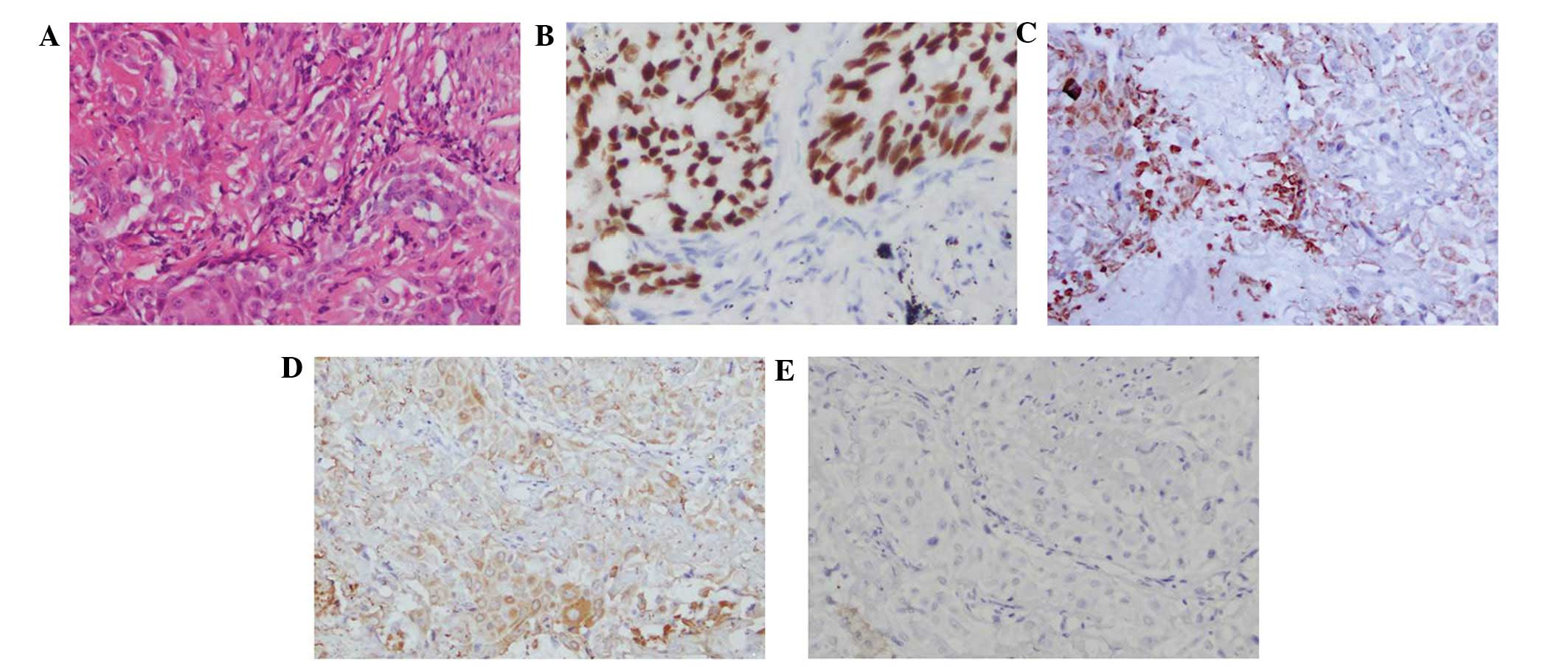
resected tumor exhibited typical adenocarcinomatous characteristics
on hematoxylin and eosin staining. Immunohistochemical (IHC)
staining demonstrated strong expression of the transcription
factor-1 (Abbott, USA), carcinoembryonic antigen (CEA; Dako,
Glostrup, Denmark) and cytokeratin-7 (Dako) proteins. The findings
of laboratory examinations were within the normal range, with the
exception of CEA, which demonstrated a serum level of 6.24 ng/ml
(normal range, 0.00–5.00 ng/ml). The pathological diagnosis of the
tumor specimen was acinar adenocarcinoma (Fig. 1) harboring one EGFR mutation in exon
21, the L858R mutation. Subsequent to consideration of the poor
condition of the patient, treatment with gefitinib was selected at
a dose of 250 mg/day for 3 months.
A chest X-ray performed 20 days later revealed that
the completely occluded left main bronchus had reopened and that
the right lung atelectasis was considerably improved. There were no
severe side-effects, such as lung toxicity. However, 3 months
following the initiation of gefitinib therapy, the tumor began to
enlarge (Fig. 2). Gefitinib therapy
was discontinued in order to introduce second-line chemotherapy,
consisting of docetaxel (75 mg/m2, once) and gefitinib
(250 mg/day) for 3 weeks, which induced infusion reaction. No
notable response was observed. Following discontinuation of the
second-line chemotherapy, tumor growth induced empyema and the
general condition of the patient gradually deteriorated.
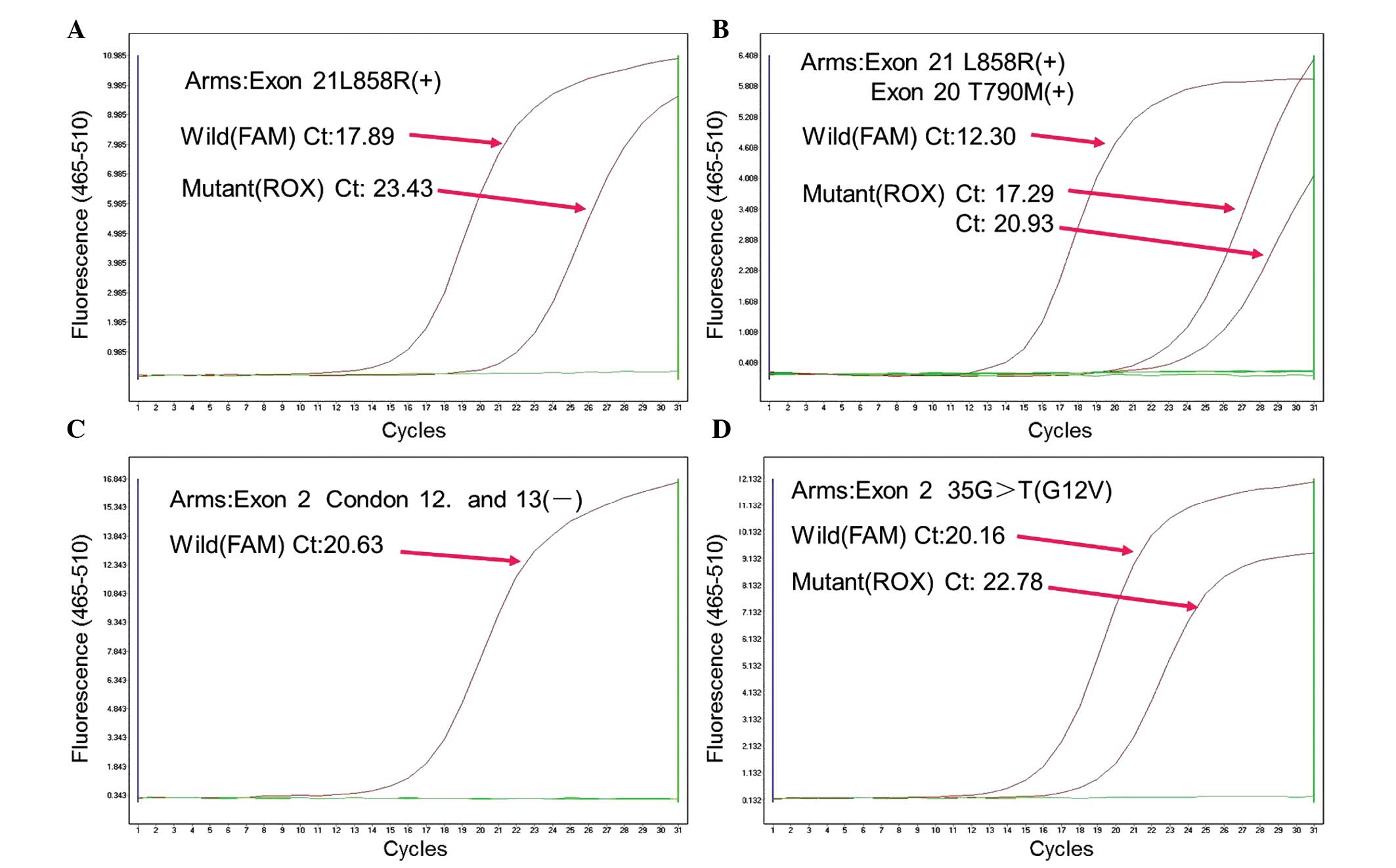
Trans-bronchial lung biopsy of the right lung was then performed to
perform EGFR and KRAS mutation analysis using amplification
refractory mutation system (Amoy Diagnostics Co., Ltd., Haicang,
Xiamen, China). In the tumor DNA, the point mutations L858R, in
which leucine at amino acid 858 is replaced by arginine, and T790M,
in which threonine at amino acid 790 is replaced by methionine,
were detected in the EGFR gene, in addition to the KRAS G12V
mutation (Fig. 3). However, these
findings could not be applied to the treatment strategy as the
patient succumbed to respiratory failure 2 months later. The
present study was approved by the ethics committee of Sun Yat-Sen
University and written informed consent was obtained from the
patient's family.
Discussion
It has been demonstrated that the majority of
patients with EGFR TKI-sensitive lung cancer harbor activating
mutations in the TK domain of EGFR (13–15), which
supports the hypothesis that identifying genetic signatures
associated with oncogenic alterations may yield predictive
biomarkers for corresponding molecular target inhibitors. Compared
to smokers, EGFR mutations have consistently been found to be more
common in never-smokers (16). It has
been demonstrated that the majority of tumors with activating EGFR
mutations present with a non-squamous histology. Retrospective data
reported by Tanaka et al reveals that 3–8% of patients with
NSCLC that demonstrated squamous histology present in activating
EGFR mutations (17). The present
diagnosis of squamous cell carcinoma or adenocarcinoma was based on
histomorphological analysis, in cases where the appearance was
characteristic, or IHC staining, which was performed using
antibodies against TTF-1, p63, CEA and CK. Nuclear expression of
TTF-1, identified by IHC, demonstrated the lesion in the present
patient to be of primary pulmonary origin. Furthermore, tumor cells
were CEA-positive and p63-negative, indicating that they may
originate from the glandular epithelium.
Deletion mutations in exon 19 that affect the
conserved LREA motif and a single amino acid substitution, leucine
to arginine, at codon 858 in exon 21 are associated with increased
sensitivity to EGFR TKIs, including gefitinib and erlotinib
(18–20). The clinical observation that the
present patient with a L858R mutation achieved radiographic tumor
regression may be indicative that patients with EGFR L858R-bearing
tumors can benefit from gefitinib at the usual clinical doses.
However, in a previous study >20% of patients demonstrated
resistance to EGFR TKIs and all tumors ultimately developed
resistance following the initial response (21). The most common molecular mechanism of
acquired resistance is a mutation at a second site in the EGFR
tyrosine kinase domain, T790M. This mutation confers resistance by
increasing the affinity for ATP, with which inhibitors must compete
for binding, and also by modestly decreasing the intrinsic affinity
for TKIs (22).
In the present study, 3 months subsequent to the
initiation of gefitinib therapy, the tumor relapsed and a CT scan
demonstrated progressive disease. Molecular analysis demonstrated
the presence of an adenocarcinoma harboring two different EGFR
mutations, consisting of a mutation in exon 20 (T790M) and a
mutation in exon 21 (L858R). Consistent with the role of KRAS
mutations as driver mutations, KRAS mutations do not occur in
association with EGFR mutations (23–26),
although rare exceptions do occur (27). However, the present study reported the
case of a patient that possessed tumor DNA harboring KRAS and EGFR
mutations, a phenomenon that has been rarely reported. Furthermore,
a meta-analysis has revealed that tumors harboring a KRAS mutation
are resistant to EGFR TKIs (28), as
KRAS mutations lead to constitutive activation of pathways
downstream of EGFR. The aforementioned data demonstrated that the
recurrence and rapid resistance to gefitinib observed in the
present patient may be attributed to the T790M mutation in EGFR and
the KRAS mutation simultaneously. In particular, it has been
demonstrated in colorectal cancer of an advanced stage that under
conditions of EGFR-blockade, pre-existing undetected KRAS mutant
cells contribute to relapse (29,30). There
are several reasons to expect that KRAS may play a similar role in
the acquired resistance to EGFR blockade in lung adenocarcinoma.
First, KRAS mutant subpopulations have been identified in lung
adenocarcinoma tumors (31).
Secondly, in lung adenocarcinoma lesions, KRAS mutation has been
reported to confer primary resistance to EGFR blockade (9). Thus, the exploration of a more sensitive
detecting system for tumor tissues is urgently required in order to
provide more reasonable treatment options for patients.
Resistance to targeted therapies is an increasingly
reported issue, into which genomic analyses may provide important
mechanistic insights for future rational therapeutic approaches.
The present study reported a rare case of lung cancer harboring a
KRAS mutation and a compound T790M EGFR substitution mutation,
which was identified subsequent to the administration of gefitinib
treatment to the patient. Thus, to improve the guidance for optimal
treatment schemes in individual patients, additional studies that
aim to identify the genetic causes of drug resistance at various
points during the clinical course are required.
Acknowledgements
The present study received financial support from
the National Natural Science Foundation of China (grant nos.,
30900650/H1615, 81372501/H1615, 81172232/H1615 and 81172564/H1625),
Guangdong Natural Science Foundation (grant nos., S2012010008378
and S2013010015327), Research Fund for the Doctoral Program of
Higher Education of China (grant no., 20120171120086) and Science
and Technology Planning Project of Guangdong Province (grant no.,
2012B061700078).
Glossary
Abbreviations
Abbreviations:
|
KRAS
|
kirsten rat sarcoma viral oncogene
homolog
|
|
EGFR
|
epidermal growth factor receptor
|
|
TKI
|
tyrosine kinase inhibitor
|
|
NSCLC
|
non-small cell lung cancer
|
|
CT
|
computed tomography
|
|
IHC
|
immunohistochemical
|
|
CEA
|
carcinoembryonic antigen
|
References
|
1
|
Gaughan EM and Costa DB: Genotype-driven
therapies for non-small cell lung cancer: Focus on EGFR, KRAS and
ALK gene abnormalities. Ther Adv Med Oncol. 3:113–125. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Rosell R, Carcereny E, Gervais R, et al
Spanish Lung Cancer Group in collaboration with Groupe Français de
Pneumo-Cancérologie and Associazione Italiana Oncologia Toracica:
Erlotinib versus standard chemotherapy as first-line treatment for
European patients with advanced EGFR mutation-positive
non-small-cell lung cancer (EURTAC): A multicentre, open-label,
randomised phase 3 trial. Lancet Oncol. 13:239–246. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Takano T, Ohe Y, Sakamoto H, et al:
Epidermal growth factor receptor gene mutations and increased copy
numbers predict gefitinib sensitivity in patients with recurrent
non-small-cell lung cancer. J Clin Oncol. 23:6829–6837. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kobayashi S, Boggon TJ, Dayaram T, et al:
EGFR mutation and resistance of non-small-cell lung cancer to
gefitinib. N Engl J Med. 352:786–792. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kosaka T, Yatabe Y, Endoh H, et al:
Analysis of epidermal growth factor receptor gene mutation in
patients with non-small cell lung cancer and acquired resistance to
gefitinib. Clin Cancer Res. 12:5764–5769. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Riely GJ, Kris MG, Rosenbaum D, et al:
Frequency and distinctive spectrum of KRAS mutations in never
smokers with lung adenocarcinoma. Clin Cancer Res. 14:5731–5734.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
De Luca A and Normanno N: Predictive
biomarkers to tyrosine kinase inhibitors for the epidermal growth
factor receptor in non-small-cell lung cancer. Curr Drug Targets.
11:851–864. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Mao C, Qiu LX, Liao RY, et al: KRAS
mutations and resistance to EGFR-TKIs treatment in patients with
non-small cell lung cancer: A meta-analysis of 22 studies. Lung
Cancer. 69:272–278. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Pao W, Wang TY, Riely GJ, et al: KRAS
mutations and primary resistance of lung adenocarcinomas to
gefitinib or erlotinib. PLoS Med. 2:e172005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Stella GM, Scabini R, Inghilleri S, et al:
EGFR and KRAS mutational profiling in fresh non-small cell lung
cancer (NSCLC) cells. J Cancer Res Clin Oncol. 139:1327–1335. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Pennycuick A, Simpson T, Crawley D, et al:
Routine EGFR and KRAS Mutation analysis using COLD-PCR in non-small
cell lung cancer. Int J Clin Pract. 66:748–752. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hammerman PS, Jänne PA and Johnson BE:
Resistance to epidermal growth factor receptor tyrosine kinase
inhibitors in non-small cell lung cancer. Clin Cancer Res.
15:7502–7509. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lynch TJ, Bell DW, Sordella R, et al:
Activating mutations in the epidermal growth factor receptor
underlying responsiveness of non-small-cell lung cancer to
gefitinib. N Engl J Med. 350:2129–2139. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sequist LV, Martins RG, Spigel D, et al:
First-line gefitinib in patients with advanced non-small-cell lung
cancer harboring somatic EGFR mutations. J Clin Oncol.
26:2442–2449. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Paez JG, Jänne PA, Lee JC, et al: EGFR
mutations in lung cancer: Correlation with clinical response to
gefitinib therapy. Science. 304:1497–1500. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Cortes-Funes H, Gomez C, Rosell R, et al:
Epidermal growth factor receptor activating mutations in Spanish
gefitinib-treated non-small-cell lung cancer patients. Ann Oncol.
16:1081–1086. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Tanaka T, Matsuoka M, Sutani A, et al:
Frequency of and variables associated with the EGFR mutation and
its subtypes. Int J Cancer. 126:651–655. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Mitsudomi T, Morita S, Yatabe Y, et al
West Japan Oncology Group: Gefitinib versus cisplatin plus docetaxel
in patients with non-small-cell lung cancer harbouring mutations of
the epidermal growth factor receptor (WJTOG3405): An open label,
randomised phase 3 trial. Lancet Oncol. 11:121–128. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mok TS, Wu YL, Thongprasert S, et al:
Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N
Engl J Med. 361:947–957. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Rosell R, Viteri S, Molina MA, et al:
Epidermal growth factor receptor tyrosine kinase inhibitors as
first-line treatment in advanced nonsmall-cell lung cancer. Curr
Opin Oncol. 22:112–120. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Pao W and Chmielecki J: Rational,
biologically based treatment of EGFR-mutant non-small-cell lung
cancer. Nat Rev Cancer. 10:760–774. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Yun CH, Mengwasser KE, Toms AV, et al: The
T790M mutation in EGFR kinase causes drug resistance by increasing
the affinity for ATP. Proc Natl Acad Sci USA. 105:2070–2075. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Yip PY, Yu B, Cooper WA, et al: Patterns
of DNA mutations and ALK rearrangement in resected node negative
lung adenocarcinoma. J Torac Oncol. 8:408–414. 2013. View Article : Google Scholar
|
|
24
|
Ding L, Getz G, Wheeler DA, et al: Somatic
mutations affect key pathways in lung adenocarcinoma. Nature.
455:1069–1075. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Shigematsu H, Lin L, Takahashi T, et al:
Clinical and biological features associated with epidermal growth
factor receptor gene mutations in lung cancers. J Natl Cancer Inst.
97:339–346. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Tam IY, Chung LP, Suen WS, et al: Distinct
epidermal growth factor receptor and KRAS mutation patterns in
non-small cell lung cancer patients with different tobacco exposure
and clinicopathologic features. Clin Cancer Res. 12:1647–1653.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Schmid K, Oehl N, Wrba F, et al:
EGFR/KRAS/BRAF mutations in primary lung adenocarcinomas and
corresponding locoregional lymph node metastases. Clin Cancer Res.
15:4554–4560. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Linardou H, Dahabreh IJ, Kanaloupiti D, et
al: Assessment of somatic k-RAS mutations as a mechanism associated
with resistance to EGFR-targeted agents: A systematic review and
meta-analysis of studies in advanced non-small-cell lung cancer and
metastatic colorectal cancer. Lancet Oncol. 9:962–972. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Misale S, Yaeger R, Hobor S, et al:
Emergence of KRAS mutations and acquired resistance to anti-EGFR
therapy in colorectal cancer. Nature. 486:532–536. 2012.PubMed/NCBI
|
|
30
|
Diaz LA Jr, Williams RT, Wu J, et al: The
molecular evolution of acquired resistance to targeted EGFR
blockade in colorectal cancers. Nature. 486:537–540.
2012.PubMed/NCBI
|
|
31
|
Parsons BL and Myers MB: Personalized
cancer treatment and the myth of KRAS wild-type colon tumors.
Discov Med. 15:259–267. 2013.PubMed/NCBI
|