Introduction
Gliomas are tumors that originate within brain
tissues; they arise from glial cells and are the most common brain
tumors, making up ~45% of all tumors found in the brain (1). According to the data from the World
Health Organization (WHO), glioblastoma is the second leading cause
of cancer-related mortality in children and young adults below the
age of 35 (2).
The early detection and diagnosis of gliomas has
been improved significantly in recent years. However, the survival
rate of patients with gliomas remains low. An urgent requirement
therefore exists to understand the molecular mechanisms that
underlie the occurrence and progression of gliomas and develop
novel methods for the diagnosis and treatment of this type of brain
tumor. In the majority of cases, the diagnosis of glioma at an
early stage relies on the combination of clinical observation,
imaging and pathological examination (3). In addition, cancer biomarkers hold
promise for use in early tumor detection and diagnosis. Cyclin A
and Ki-67 are highly expressed in several malignant tumors.
Recently, their expression has been used as a powerful index for
malignant cell proliferation and prognosis, but their roles in
gliomas and their metastasis have remained poorly understood
(4,5).
In the present study, the expression and mutation of
Cyclin A and Ki-67 were detected in glioma tissues from patients,
and their association with glioma classification and lymphatic
metastasis was investigated. The results may provide useful
information on the diagnosis, evaluation, treatment and prognosis
of glioma patients.
Materials and methods
Glioma tissues
Specimens of brain tumors were obtained from glioma
patients who received surgery between March 2009 and January 2014
in Xinxiang Central Hospital (Xinxiang, Henan, China). The degree
of differentiation, infiltration levels, lymphatic metastasis and
degree of malignancy were recorded for each patient. A total of 186
patients were included in the study. Of these patients, 107 were
male and 79 were female, with ages ranging from 27 to 76 years old
(mean, 48.92±8.29 years). According to the 1999 WHO classification
system (6), the patients were divided
into the following categories: 47 cases of astrocytic tumors, 21
cases of oligodendrogliomas, 19 cases of ependymoma, 26 cases of
mixed gliomas, 15 cases of choroid plexus tumors, 17 cases of mixed
neuronal-glial tumors, 26 cases of pineal parenchymal tumors, 9
cases of embryonal tumors and 6 cases of neuroblastomas. According
to the 2000 WHO grading system (7),
which categorizes gliomas into low-grade glioma (WHO grade I–II)
and high-grade glioma (WHO grade III–IV) (8), out of the 186 patients, 84 were grade
I–II and 102 were grade III–IV. This study was conducted in
accordance with the declaration of Helsinki. This study was
conducted with approval from the Ethics Committee of Xinxiang
Central Hospital. Written informed consent was obtained from all
participants.
Immunohistochemistry
Paraffin blocks of surgical specimen from glioma
patients were sectioned into 4-µm slices, deparaffinized and
rehydrated. The slides were washed with phosphate-buffered saline,
treated with antibody signal enhancer, and incubated with mouse
anti-human monoclonal antibody against Cyclin A (1:500; cat. no.
LBP-IHC-M057) and mouse anti-human monoclonal antibody against
Ki-67 (1:500; cat. no. LBP-IHC-R098) (both Daan Gene Inc.,
Guangzhou, China). Immunosignals were developed with DAB (Daan Gene
Inc.) as the chromogen. The sections were contrast-stained with
hematoxylin and mounted in neutral resin.
DNA extraction, polymerase chain
reaction (PCR) and sequencing
Fresh tissue samples (30 mg) from glioma specimens
or metastatic lymph nodes were homogenized with MagNA Lyser (Roche,
Basel, Switzerland). The concentration of extracted genomic DNA was
measured using NanoDrop 2000 (Thermo Scientific, Rockford, IL,
USA), and the genomic DNA was diluted to a working concentration of
30–50 ng/l.
Four exons of Cyclin A and two codons of KRAS were
amplified by PCR. Each reaction (in a total of 20 µl reaction
volume) contained 1X Hot Startaq buffer, 2.0 mM Mg2+,
0.2 mM dNTP, 0.2 µM of each primer, 1 unit of Hot Startaq
polymerase and 10 ng DNA template. PCR conditions were as follows:
95°C for 5 min, followed by 25 cycles of 94°C for 40 sec, 56°C for
30 sec and 72°C for 40 sec and final elongation at 72°C for 3 min.
The product was purified and sequenced using an ABI 3130XL Genetic
Analyzer (Applied Biosystems, Foster City, CA, USA). The sequencing
results were analyzed using PolyPhred analysis software (http://droog.gs.washington.edu/polyphred/real_polymorphism.html).
Detection of gene mutations
The mutations in Cyclin A and Ki-67 were detected
using Cyclin A and Ki-67 Mutation Detection kits from Daan Gene
Inc. Light Cycler 480 II (Roche) was used to detect the changes in
the EGFR4 and KRAS genes.
Criteria and standards for
immunohistochemistry
The positive signal was localized to the cytoplasm
and membrane for Cyclin A staining, and to the membrane or
cytoplasmic puncta for Ki-67 staining. The intensity of staining
was evaluated in 10 areas of each section. The percentage of cells
with positive staining was scored as follows: 0, <5% staining;
1, 6–25% staining; 2, 26–50% staining; 3, 51–75% staining and 4,
>75% staining. The staining intensity was scored as follows: 3,
brown; 2, yellow; and 1, light yellow. The scores for percentage of
positive cells and staining intensity were combined to generate an
overall score index: Strongly positive (+++), 6–9 points;
moderately positive (++), 4–5 points; weakly positive (+), 2–3
points; and negative (−), 0–1 points (9).
Statistical analysis
Statistical analysis was performed using SPSS 14.0
software (SPSS Inc., Chicago, IL, USA). The t-test was used
to compare the difference between two groups. P<0.05 was used to
indicate a statistically significant difference.
Results
Expression of Cyclin A and Ki-67 in
glioma
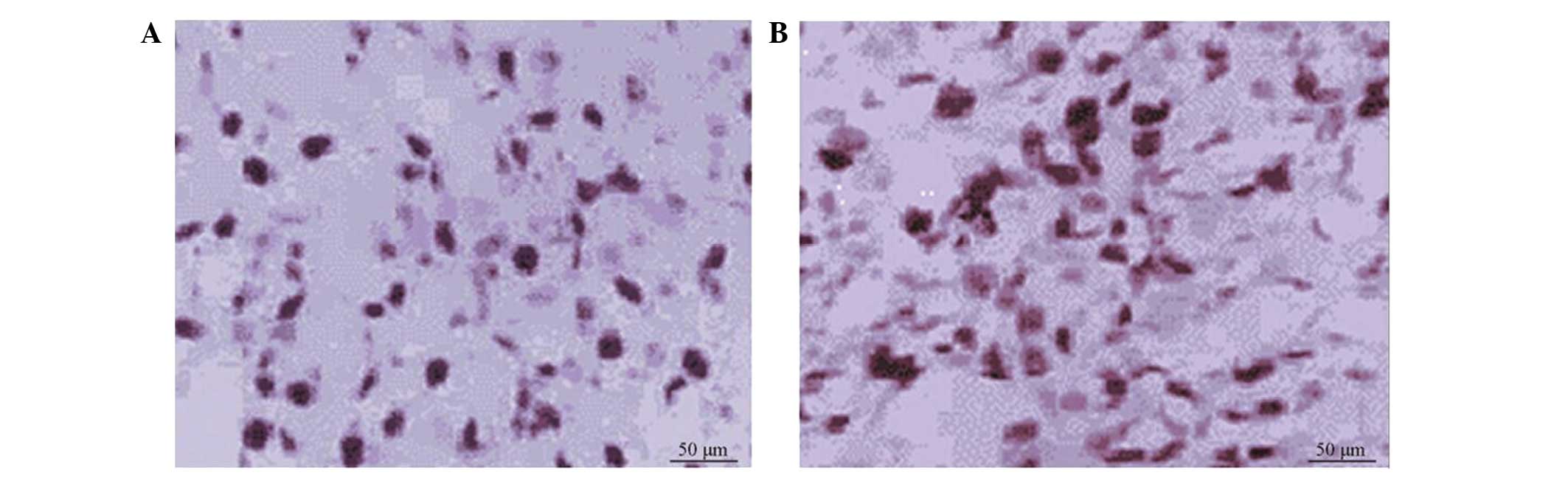
Out of 186 patients, 64 (34.41%) were positive for
Cyclin A staining and 68 (36.56%) for Ki-67 staining in the glioma
tissues or metastatic lymph nodes. Statistical analysis showed that
the expression of Cyclin A and Ki-67 exhibited no correlation with
the clinicopathological factors of age, gender, tumor size and
smoking history (P>0.05) (Table
I), but was correlated with the clinical stage, degree of
differentiation and lymphatic metastasis. In the patients with
poorly-differentiated tumors, lymphatic metastasis or grade III–IV
gliomas, the positive expression rates for Cyclin A were 42.22,
47.25 and 47.12%, respectively, and for Ki-67, these rates were
41.48, 45.05 and 48.08%, respectively (Table I). The positive rate for Cyclin A and
Ki-67 in these patients was significantly higher than that in
patients with well-differentiated tumors, no lymphatic metastasis
or grade I–II gliomas (P<0.05) (Table
I; Fig. 1).
 | Table I.Association between Cyclin A and Ki-67
expression and gliomas (mean ± standard deviation). |
Table I.
Association between Cyclin A and Ki-67
expression and gliomas (mean ± standard deviation).
|
|
| Cyclin A expression,
n |
|
| Ki-67 expression,
n |
|
|
|---|
|
|
|
|
|
|
|
|
|
|---|
| Characteristic | n | (−) | (+) | Positive rate, % | P-value | (−) | (+) | Positive rate, % | P-value |
|---|
| Patients | 186 | 122 | 64 |
|
| 118 | 68 |
|
|
| Gender |
|
|
|
| 0.827 |
|
|
| 0.952 |
| Male | 107 | 69 | 38 | 35.51 |
| 68 | 39 | 36.45 |
|
| Female | 79 | 53 | 26 | 32.91 |
| 50 | 29 | 36.71 |
|
| Age, years |
|
|
|
| 0.762 |
|
|
| 0.985 |
| <60 | 123 | 79 | 44 | 35.77 |
| 78 | 45 | 36.59 |
|
| ≥60 | 63 | 43 | 20 | 31.75 |
| 40 | 23 | 36.51 |
|
| Smoking history |
|
|
|
| 0.962 |
|
|
| 0.809 |
| Yes | 73 | 48 | 25 | 34.25 |
| 45 | 28 | 38.36 |
|
| No | 113 | 74 | 39 | 34.51 |
| 73 | 40 | 35.40 |
|
| Tumor size, cm |
|
|
|
| 0.274 |
|
|
| 0.217 |
| ≤4 | 99 | 70 | 29 | 29.29 |
| 69 | 30 | 30.30 |
|
| >4 | 87 | 52 | 35 | 40.23 |
| 49 | 38 | 43.68 |
|
| TNM grading |
|
|
|
| 0.011a |
|
|
| 0.024a |
| I–II | 82 | 67 | 15 | 18.29 |
| 64 | 18 | 21.95 |
|
| III–IV | 104 | 55 | 49 | 47.12 |
| 54 | 50 | 48.08 |
|
| Differentiation |
|
|
|
| 0.003a |
|
|
| 0.041a |
| Well | 51 | 44 | 7 | 13.73 |
| 39 | 12 | 23.53 |
|
| Poor | 135 | 78 | 57 | 42.22 |
| 79 | 56 | 41.48 |
|
| Lymphatic
metastasis |
|
|
|
| 0.028a |
|
|
| 0.049a |
| Yes | 91 | 48 | 43 | 47.25 |
| 50 | 41 | 45.05 |
|
| No | 95 | 74 | 21 | 22.12 |
| 68 | 27 | 28.42 |
|
Mutation analysis of Ki-67 and Cyclin
A genes in glioma tissues and metastatic lymph nodes
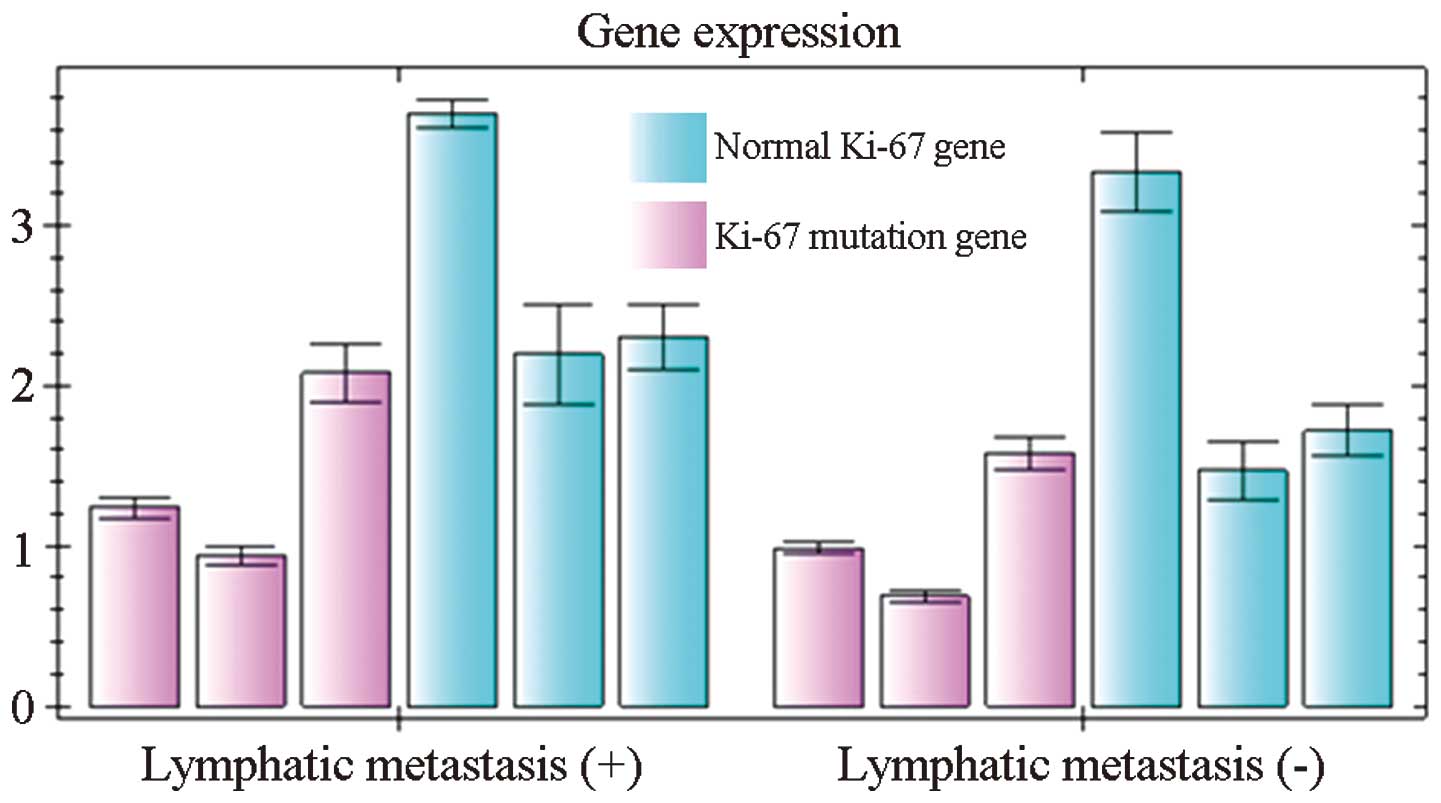
Of the 186 patients, 91 presented with lymphatic
metastasis. In the 95 patients without lymphatic metastasis, 27
were found to have Ki-67 expression. In the 91 patients with
lymphatic metastasis, 34 were found to have Ki-67 expression in the
glioma tissues and 41 in the metastatic lymph nodes. There were
significant differences in the mutation rate of Ki-67 between the
glioma and metastatic tissue sites (P<0.05). Point mutations of
Ki-67 were detected in 1 glioma tissue and 7 metastatic tissues. Of
these mutations, 5 were mutated in the codon for amino acid 12 and
2 in the codon for amino acid 13. Statistical analysis showed that
the Ki-67 mutation rate was not associated with patient gender,
smoking history and tumor subtype (Fig.
2).
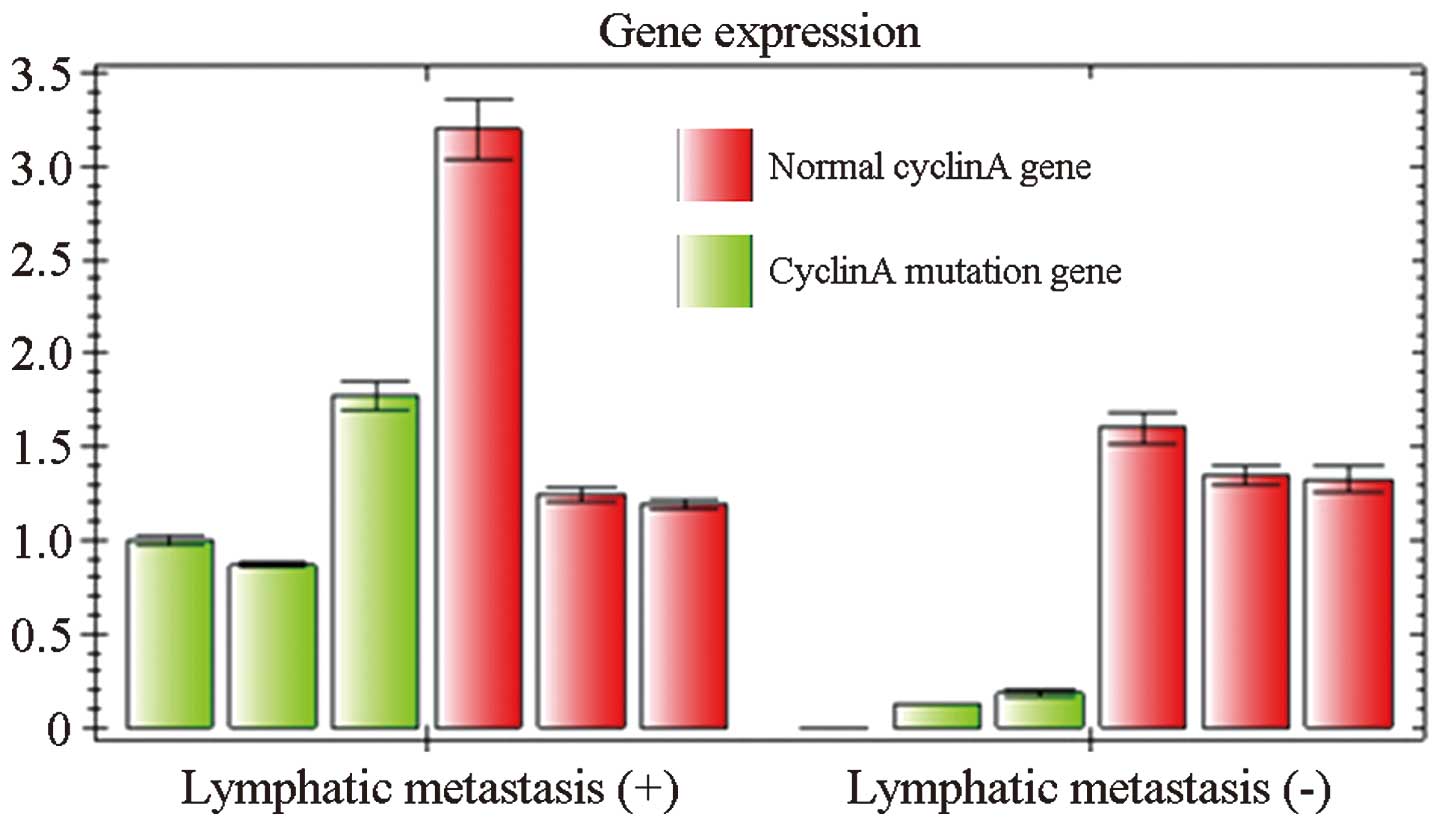
With regard to Cyclin A, 21 of the patients without
lymphatic metastasis were positive for its expression. In the
patients with lymphatic metastasis, 32 were positive for Cyclin A
expression in the glioma tissues and 43 in the metastatic tumor
sites. Mutations in Cyclin A were identified in 21 glioma tissues
and 26 metastatic tumor tissues. There was no significant
difference in the mutation rate of Cyclin A between the glioma
tissues and the metastatic tissue sites (P>0.05). Statistical
analysis showed that the mutation rate of Cyclin A in non-smoking
women was significantly higher than that in men who smoked
(P<0.05) (Fig. 3).
Discussion
Glioma is a primary brain tumor that originates from
glial cells. The tumor has one of the worst prognoses. A better
prognosis for glioma depends on its early detection and diagnosis.
The rapid development of molecular biology and its application in
cancer biology revolutionized the research on gliomas, and has
generated significant insights into the mechanisms underlying
glioma pathogenesis. Clinical observations suggest that the same
gliomas diagnosed by conventional analysis of pathological features
may have significant differences in their response to treatments
and their prognosis, as well as in the invasion, recurrence and
metastasis of these tumors (10,11).
Experimental data have shown that these differences are due to
changes in genes, which necessitates the use of molecular biology
and immunohistochemical techniques to detect gene or protein
changes (12–14). In the present study, Ki-67 and Cyclin
A, two important genes that are associated with malignant tumors,
were selected and their expression and mutation in patients with
gliomas was investigated.
Cyclin A belongs to the Cyclin family, a group of
proteins that regulate the cell cycle. Cyclin A positively
regulates the cell cycle. First identified in hepatitis B virus DNA
integration sites in tumor cells of primary liver cancer, Cyclin A
was believed to possess oncogenicity. Cyclin A is essential for
cells to pass S phase and G2/M phase. It accumulates in the late
G1 phase prior to DNA synthesis, and participates in DNA
replication, synthesis and the entry of cells into mitosis.
Therefore, the expression level of Cyclin A is critical for the
normal growth and proliferation of cells. Abnormal expression of
Cyclin A may cause mismatch or incomplete synthesis of DNA, which
is believed to lead to carcinogenesis. Cyclin A is highly expressed
in several tumor cells, and has been used as an index of malignant
proliferation of these cells and poor prognosis (15,16). Ki-67
is a nuclear protein that is associated with cellular
proliferation. Although it is necessary for mitosis, the exact
mechanism is unknown. Positive expression of Ki-67 indicates an
active proliferation of cancer cells. In addition, Ki-67 is also a
protein that is associated with the cell cycle. Therefore, it is
used as a biomarker for various malignant cancers. The expression
of Ki-67 in poorly-differentiated tumor tissues is significantly
higher than its expression in well-differentiated adenocarcinoma
tissues, which indicates that the expression level of Ki-67 is
correlated with histological grading (17,18). The
present results suggest that the expression of Ki-67 is associated
with the occurrence and development of gliomas, and is a sign of
poor prognosis.
The detection of mutations in Ki-67 is important for
the understanding of cancer progression and the development of
proper therapeutic strategies. Mutations in Ki-67 occur at the
early stages of tumorigenesis, and these mutations are similar in
primary cancer and metastatic tissues. It has been hypothesized
that the status of the KRAS genes will not be changed by therapies.
Approximately 20% of gliomas have Ki-67 mutations. Gliomas are
tumors with extreme heterogeneity. Therefore, the confirmation of
the consistent expression of Cyclin A and Ki-67 in primary tumor
sites and metastatic tumor sites is important for those who choose
targeted cancer therapies (19).
Our results showed that the expression of Cyclin A
was not correlated with gender, age, degree of invasion, tumor
size, distant metastasis or clinical grading (P>0.05). However,
it was associated with the degree of differentiation and lymphatic
metastasis. The expression of Ki-67 was not correlated with gender,
age, tumor size, distant metastasis and degree of differentiation
(P>0.05), but was associated with the degree of invasion,
lymphatic metastasis and clinical grading (Table I). These data suggest that the
detection of Cyclin A and Ki-67 has clinical significance in
determine the metastasis, progression and prognosis of glioma
patients who receive surgery. In addition, these results showed
that the genes of Cyclin A and Ki-67 can be changed during tumor
metastasis, although the underlying mechanisms remain unknown. This
phenomenon can explain the different responses of glioma patients
to targeted therapies.
In clinical treatment, personalized and targeted
therapies are becoming optimized choices for oncologists and
patients. Adjuvant therapies have been used in the treatment of
glioma patients prior to surgery. By reducing the size of tumors
and lowing the grade of regional tumors, certain terminal cancer
patients may obtain the opportunity for surgery. Examination of
lymphatic metastasis can provide more accurate information for
glioma grading, which will be useful for choosing the best
treatment for the patients (20).
Patients who are negative in conventional examination may have
micrometastasis in the mediastinum, bone marrow and lungs. Such
patients have reached grade IV, and should be treated with new
adjuvant chemotherapy prior to any surgery. For glioma patients
with metastasis in the bone marrow and peripheral blood, early
chemotherapy should be administered prior to surgery, which has
been shown to lower the grades of 35% of patients with grade III–IV
gliomas (21). Certain studies have
indicated that distant metastasis may occur in patients diagnosed
with grade I gliomas. For such patients, the detection of
biomarkers of tumors is necessary to identify metastasis and the
requirement for chemotherapy prior to surgery (22).
In the present study, it was demonstrated that
mutations in the Ki-67 and Cyclin A genes are not only important
for tumorigenesis, but also promote invasion and metastasis. Thus,
detecting the expression and mutation of Ki-67 and Cyclin A in
primary tumor sites and metastatic lymph nodes may provide critical
information for clinical diagnosis, disease evaluation, treatment
and prognosis.
References
|
1
|
Scheidegger R, Wong ET and Alsop DC:
Contributors to contrast between glioma and brain tissue in
chemical exchange saturation transfer sensitive imaging at 3Tesla.
Neuroimage. 99:256–268. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Stupp R, Hegi ME, Mason WP, van den Bent
MJ, Taphoorn MJ, Janzer RC, Ludwin SK, Allgeier A, Fisher B,
Belanger K, et al: Effects of radiotherapy with concomitant and
adjuvant temozolomide versus radiotherapy alone on survival in
glioblastoma in a randomised phase III study: 5-year analysis of
the EORTC-NCIC trial. Lancet Oncol. 10:459–466. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sanai N, Chang S and Berger MS: Low-grade
gliomas in adults. J Neurosurg. 115:948–965. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tökés AM, Szász AM, Geszti F, et al:
Expression of proliferation markers Ki67, cyclin A, geminin and
aurora-kinase A in primary breast carcinomas and corresponding
distant metastases. J Clin Pathol. 68:274–282. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bosserhoff AK: Novel biomarkers in
malignant melanoma. Clin Chim Acta. 367:28–35. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kleihues P and Cavenee WK: World Health
Organization Classification of TumoursPathology and Genetics of
Tumours of the Nervous System. IARC Press; Lyon: 2000
|
|
7
|
Biernat W: 2000 World Health Organization
classification of tumors of the nervous system. Pol J Pathol.
51:107–114. 2000.PubMed/NCBI
|
|
8
|
Thomas L, Di Stefano AL and Ducray F:
Predictive biomarkers in adult gliomas: The present and the future.
Curr Opin Oncol. 25:689–694. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Masuda TA, Inoue H, Sonoda H, Mine S,
Yoshikawa Y, Nakayama K, Nakayama K and Mori M: Clinical and
biological significance of S-phase kinase-associated protein 2
(Skp2) gene expression in gastric carcinoma: Modulation of
malignant phenotype by Skp2 overexpression, possibly via p27
proteolysis. Cancer Res. 62:3819–3825. 2002.PubMed/NCBI
|
|
10
|
Katsetos CD, Reginato MJ, Baas PW, et al:
Emerging microtubule targets in glioma therapy. Semin Pediatr
Neurol. 22:49–72. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
He X, Huang Q, Qiu X, et al: LAP3 promotes
glioma progression by regulating proliferation, migration and
invasion of glioma cells. Int J Biol Macromol. 72:1081–1089. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Takanami I: The prognostic value of
overexpression of Skp2 mRNA in non-small cell lung cancer. Oncol
Rep. 13:727–731. 2005.PubMed/NCBI
|
|
13
|
Mason WP, Maestro RD, Eisenstat D, Forsyth
P, Fulton D, Laperrière N, Macdonald D, Perry J and Thiessen B:
Canadian GBM Recommendations Committee: Canadian recommendations
for the treatment of glioblastoma multiforme. Curr Oncol.
14:110–117. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kamata Y, Watanabe J, Nishimura Y, Arai T,
Kawaguchi M, Hattori M, Obokata A and Kuramoto H: High expression
of skp2 correlates with poor prognosis in endometrial endometrioid
adenocarcinoma. J Cancer Res Clin Oncol. 131:591–596. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hart MG, Grant R, Garside R, Rogers G,
Somerville M and Stein K: Temozolomide for high grade glioma.
Cochrane Database Syst Rev. 4:CD0074152008.PubMed/NCBI
|
|
16
|
Mamillapalli R, Gavrilova N, Mihaylova VT,
Tsvetkov LM, Wu H, Zhang H and Sun H: Pten regulates the
ubiquitin-dependent degradation of the CDK inhibitor p27 (KIP1)
through the ubiquitin E3 ligase SCF (SKP2). Curr Biol. 11:263–267.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
von der Lehr N, Johansson S, Wu S, Bahram
F, Castell A, Cetinkaya C, Hydbring P, Weidung I, Nakayama K,
Nakayama KI, et al: The F-box protein Skp2 participates in c-Myc
proteosomal degradation and acts as a cofactor for c-Myc-regulated
transcription. Mol Cell. 11:1189–1200. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hua W, Yao Y, Chu YW, et al: Phase I study
of dendritic cells pulsed with tumor stem-like cells associated
antigens against malignant glioma in recurrent patients. Zhong Hua
Shen Jing Wai Ke Za Zhi. 27:90–94. 2011.(In Chinese).
|
|
19
|
Athanassiou H, Synodinou M, Maragoudakis
E, Paraskevaidis M, Verigos C, Misailidou D, Antonadou D, Saris G,
Beroukas K and Karageorgis P: Randomized phase II study of
temozolomide and radiotherapy compared with radiotherapy alone in
newly diagnosed glioblastoma multiforme. J Clin Oncol.
23:2372–2377. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Yang G, Ayala G, De Marzo A, Tian W,
Frolov A, Wheeler TM, Thompson TC and Harper JW: Elevated Skp2
protein expression in human prostate cancer: Association with loss
of the cyclin-dependent kinase inhibitor p27 and PTEN and with
reduced recurrence-free survival. Clin Cancer Res. 8:3419–3426.
2002.PubMed/NCBI
|
|
21
|
Dong Y, Sui L, Watanabe Y, Sugimoto K and
Tokuda M: S-phase kinase-associated protein 2 expression in
laryngeal squamous cell carcinomas and its prognostic implications.
Oncol Rep. 10:321–325. 2003.PubMed/NCBI
|
|
22
|
Stupp R, Mason WP, van den Bent MJ, Weller
M, Fisher B, Taphoorn MJ, Belanger K, Brandes AA, Marosi C, Bogdahn
U, et al: Radiotherapy plus concomitant and adjuvant temozolomide
for glioblastoma. N Engl J Med. 352:987–996. 2005. View Article : Google Scholar : PubMed/NCBI
|