Introduction
Teratomas are a common type of germ cell tumor. They
are composed of well-differentiated or incompletely differentiated
elements of at least two of the three germ cell layers (endoderm,
mesoderm and ectoderm). Well-differentiated teratomas are termed
mature teratomas (1). Teratomas are
usually found in the gonadal organs, such as the ovaries and testes
(2), while ~15% of all teratomas are
extragonadal (3). The retroperitoneum
is the least common location (3) and
26% of retroperitoneal teratomas are malignant (4). Mature cystic teratomas in the
retroperitoneum are most commonly identified in the first 6 months
of childhood and in early adulthood (5) with an incidence of only 10–20% in adults
aged >30 years old (6). However,
many teratoma patients are asymptomatic and thus, are not diagnosed
until much later in childhood or adulthood. Furthermore, primary
retroperitoneal teratoma in adults is quite rare, accounting for
<10% of all primary retroperitoneal tumors (5). Teratomas in this location are typically
well developed and can occasionally resemble normal fetal elements
on computed tomography (CT) scans (7). The symptoms of teratoma vary depending
on the tumor location and organ of origin. Patients with ovarian
teratomas often present with abdominal or pelvic pain, which is
caused by torsion of the ovary or irritation of its ligaments
(8). Diagnostic techniques include
ultrasound, magnetic resonance imaging and computed tomgraphy.
However, definitive diagnosis is based on tumor histology (7). At present, the treatment of choice is
complete surgical removal, which exhibits a good prognosis in
benign teratomas, however, for malignant tumors, chemotherapy
treatment is also administered following surgery (9). A previous study of 183 infants and
children diagnosed with teratoma, revealed that the 10-year event
free and overall survival rates following surgery were 90.4% and
98.0% respectively (10).
Furthermore, immature teratomas are associated with a significantly
higher mortality rate than mature teratomas (11). Ocular myasthenia gravis is believed to
be an autoimmune disease with the postsynaptic defect of
neuromuscular transmission as the common feature (12). Neuromuscular transmission failure in
myasthenia gravis is most commonly elicited by auto-antibodies to
the acetylcholine receptor (AchR) (12). No cases of retroperitoneal teratoma
associated with myasthenia gravis have been reported in the
literature thus far. The present study reports a case of a primary
retroperitoneal mature teratoma in an adult with ocular myasthenia
gravis.
Case report
A 22-year-old male was referred to Shandong
Provincial Qianfoshan Hospital (Jinan, China) on September 1, 2014,
from an external institution for the treatment of persistent ptosis
and limited eyeball movement. A neostigmine test demonstrated that
symptoms associated myasthenia gravis improved following injection
with 1 mg neostigmine, while repeat nerve stimulation decreased
electrical potential of ocular muscles. Thus, the diagnosis of
ocular myasthenia gravis was confirmed by neostigmine test and
repeat nerve stimulation. The patient had previously been treated
unsuccessfully with adrenal cortical hormone (prednisone and
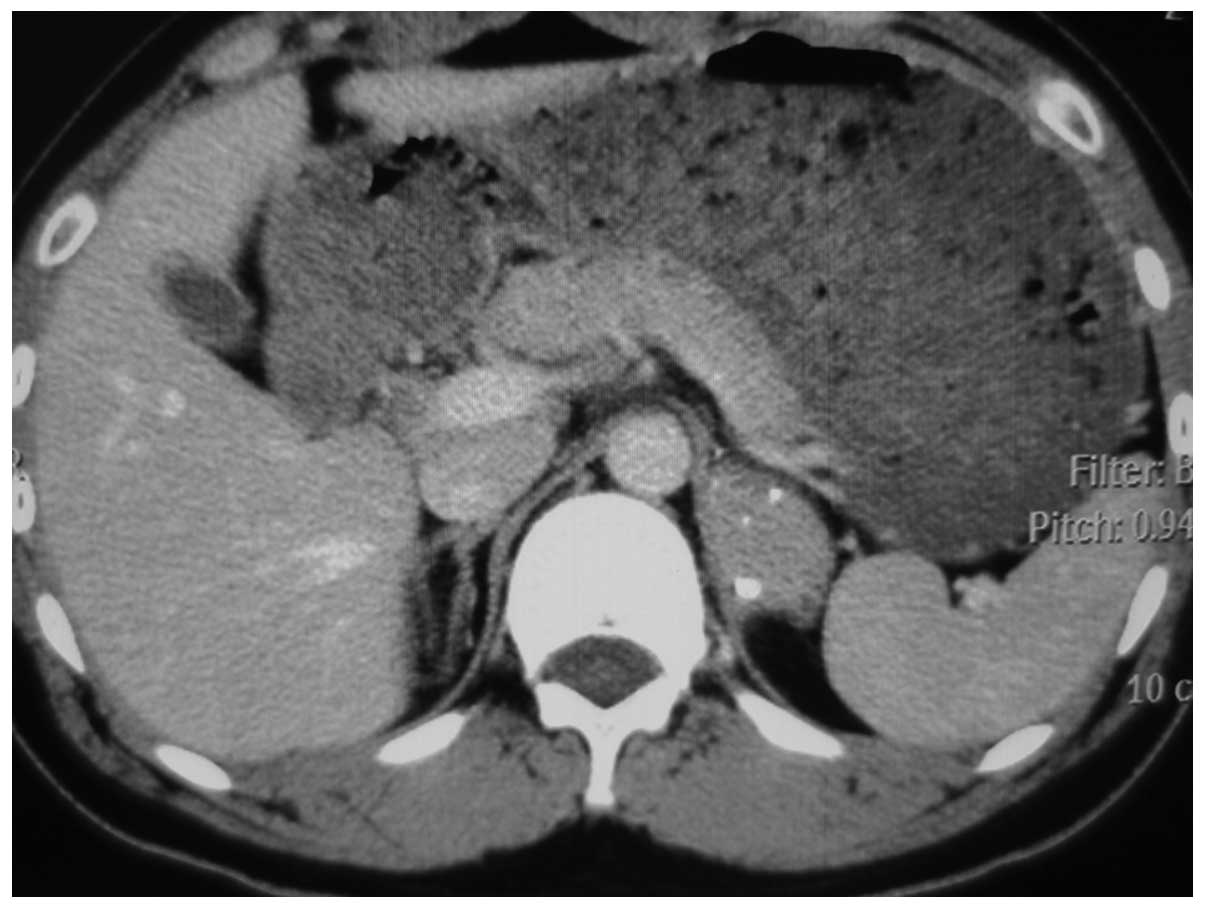
urbason) 14 years prior to the current presentation. A
thoracoabdominal CT scan, which was performed to exclude thymoma,
revealed a 5.8×2.9-cm ovoid-shaped retroperitoneal tumor with
dense, irregular calcification in the soft tissue above the left
adrenal gland (Fig. 1). There was no
tumor in the thymus and the levels of adrenal cortical hormone in
the serum were normal.
The patient was subsequently treated with a
transperitoneal laparoscopic resection of the tumor. The tumor was
located above the left adrenal gland, left and to the bottom of the
stomach, adherent to the diaphragm. During the procedure, the
capsule wall was unintentionally cut open and a large quantity of
white viscous liquid flowed out. A nodule of ~0.5 cm in diameter
was also found in the upper pole of the left adrenal gland and was
resected during the surgery. Histological analysis demonstrated
that the retroperitoneal tumor was a mature cystic teratoma and
that the adrenal nodule was cortical nodular hyperplasia. The
retroperitoneal tumor was a solid cystic lesion with thick regular
borders, and well-differentiated components within the cyst, while
the cortical nodular hyperplasia identified in the adrenal gland
consisted of proliferative and hypertrophic vacuolated cells,
containing numerous lipid droplets. On post-operative day 1, the
ptosis had disappeared and the eyeball movement was almost normal.
Written informed consent was obtained from the patient for
publication of this study.
Discussion
Teratoma is a common form of germ cell tumor,
containing all three germ cell layers. Teratomas are classified as
mature or immature, depending on the degree of differentiation of
its components (7). The tumors are
most commonly observed in the gonads of newborns and children.
Primary teratomas of the retroperitoneum are not usual in the adult
population (5), and most adult cases
are in females. Teratomas in this location tend to be well
developed. In the majority of cases, they present as asymptomatic,
making the diagnosis at an earlier stage more difficult (13).
In the present case, the patient had been diagnosed
with ocular myasthenia gravis for a long period of time and had
previously been unsuccessfully treated with pyridostigmine bromide
and adrenal cortical hormone. The orbital CT scan in Shandong
Provincial Qianfoshan Hospital was normal, and consultations from a
number of departments confirmed the diagnosis. No similar cases
have previously been reported in the literature.
The retroperitoneal teratoma was identified by
chance in this patient and was characterized by benign cystic
features with irregular calcifications. A transperitoneal
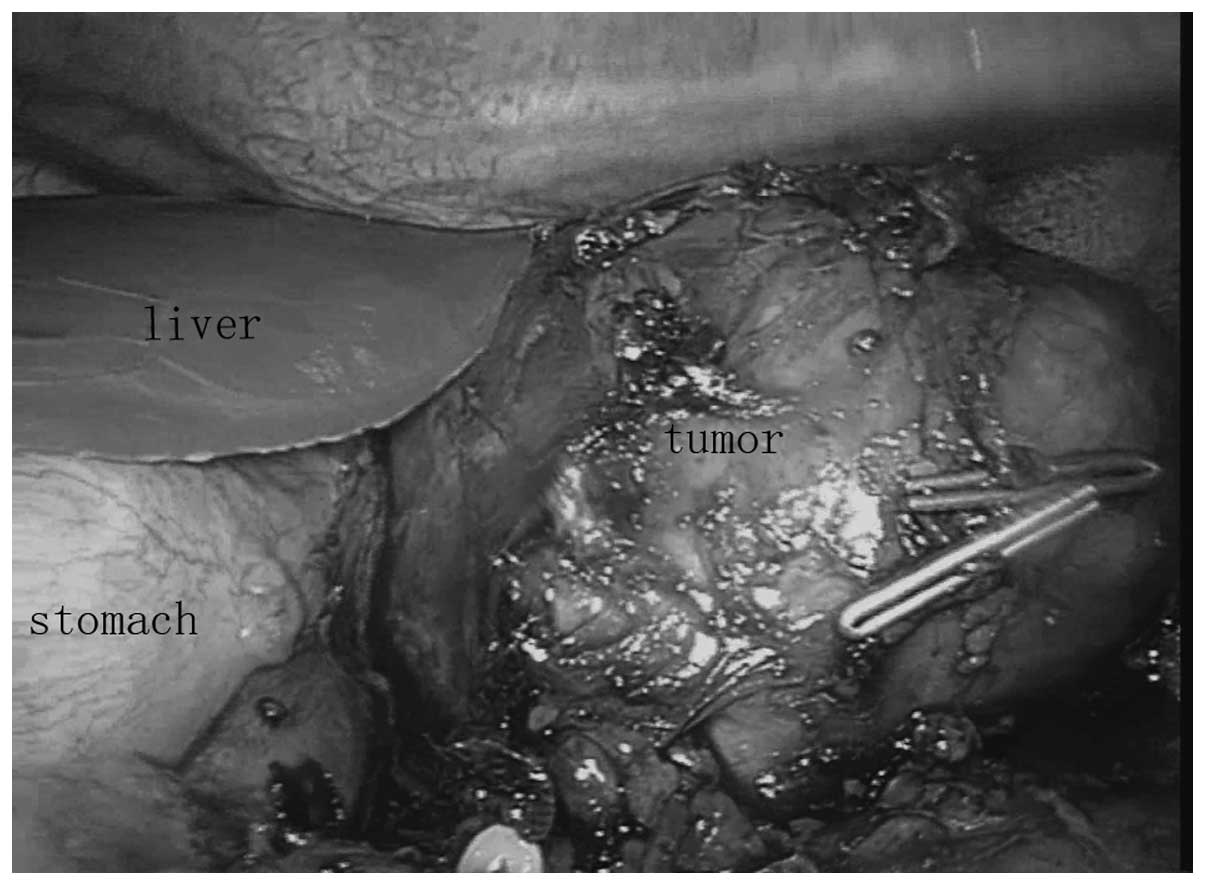
laparoscopic resection of the tumor was performed. During the
surgery, the tumor exhibited the same physical appearance and was
proximal to the stomach, and as we had not previously encountered
this situation, an intraoperative gastroscopy was performed. The
tumor was shown not to communicate with the stomach or be a part of
it (Fig. 2). A resection was then
perfomed, during which the tumor capsule was inadvertently cut. A
large amount of white viscous liquid was released and then
suctioned, and the whole capsule was eventually removed completely.
Unexpectedly, the next day, the ptosis was found to have
disappeared and the patient's eyeballs were able to move in almost
all directions.
As a classic autoimmune disease, myasthenia gravis
is believed to be caused by impairment of the AchRs induced by
anti-AchR antibody (12). In the
present study, the patient's teratoma was mature and may have
contained myoid cells with antigenicity for AchR, as has been
established in the thymus (14). The
existence of this tumor could have led to the continuous
stimulation of anti-AchR antibody and unsatisfactory therapeutic
efficacy with hormones. Although it is known that certain lung
cancers can cause myasthenia gravis, it was unclear whether there
was an endocrine substance secreted by the tumor that led to the
ptosis due to a lack experimental tests (15). Long-term follow-up should be performed
to determine if the patient's ptosis is resolved and to observe
whether any recurrence of the teratoma will occur as a result of
the tumor rupture.
The present study reported a rare case of a
retroperitoneal teratoma accompanied by ptosis, which was treated
successfully by a complete resection of the tumor. The potential
mechanism was unclear, but we hypothesized that the anti-AchR
antibody may have been involved. The diagnosis of a retroperitoneal
teratoma could be made on the basis of imaging studies, and the
gold standard treatment strategy for this neoplasm is surgical
resection without rupture.
References
|
1
|
Prokhorova TA, Harkness LM, Frandsen U,
Ditzel N, Schrøder HD, Burns JS and Kassem M: Teratoma formation by
human embryonic stem cells is site dependent and enhanced by the
presence of Matrigel. Stem Cells Dev. 18:47–54. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Shindo K, Ueda J, Toubo T, Nakamura M, Oda
Y, Eguchi T and Tanaka M: Primary carcinoid tumor in a
retroperitoneal mature teratoma: Report of a case. Surg Today.
43:694–697. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bedri S, Erfanian K, Schwaitzberg S and
Tischler AS: Mature cystic teratoma involving adrenal gland. Endocr
Pathol. 13:59–64. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Scott AL, AbbassiGhadi N, Archer CM, Swamy
R and Gupta S: Neuroendocrine carcinoma arising within a
retroperitoneal mature teratoma. Ann R Coll Surg Engl. 92:W5–W8.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Gatcombe HG, Assikis V, Kooby D and
Johnstone PA: Primary retroperitoneal teratomas: A review of the
literature. J Surg Oncol. 86:107–113. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Panageas E: General diagnosis case of the
day. Primary retroperitoneal teratoma. AJR Am J Roentgenol.
156:1292–1294. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Peterson CM, Buckley C, Holley S and
Menias CO: Teratomas: A multimodality review. Curr Probl Diagn
Radiol. 41:210–219. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sundar S, Umman P and Chisthi M: Mature
ovarian teratoma presenting as small bowel obstruction. Indian J
Surg. 75:411–413. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Göbel U, Schneider DT, Calaminus G, Haas
RJ, Schmidt P and Harms D: Germ-cell tumors in childhood and
adolescence. GPOH MAKEI and the MAHO study groups. Ann Oncol.
11:263–271. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
LoCurto M, D'Angelo P, Cecchetto G, et al:
Mature and immature teratomas: Results of the first paediatric
Italian study. Pediat Surg Int. 23:315–322. 2007. View Article : Google Scholar
|
|
11
|
Yoneda A, Usui N, Taguchi T, Kitano Y,
Sago H, Kanamori Y, Nakamura T, Nosaka S and Oba MS: Impact of the
histological type on the prognosis of patients with prenatally
diagnosed sacrococcygeal teratomas: The results of a nationwide
Japanese survey. Pediatr Surg Int. 29:1119–1125. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Blissitt PA: Clinical practice guideline
series update. J Neurosci Nurs. 45:3172013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yamasaki T, Yagihashi Y, Shirahase T,
Hashimura T and Watanabe C: Primary carcinoid tumour arising in a
retroperitoneal mature teratoma in an adult. Int J Urol.
11:912–915. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Keijzers M, NogalesGadea G and de Baets M:
Clinical and scientific aspects of acetylcholine receptor
myasthenia gravis. Curr Opin Neurol. 27:552–557. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lee JH, Shin HY, Kim SM and Sunwoo IN: A
case of lambert-eaton myasthenic syndrome with small-cell lung
cancer and transient increase in
anti-acetylcholine-receptor-binding antibody titer. J Clin Neurol.
8:305–307. 2012. View Article : Google Scholar : PubMed/NCBI
|