Introduction
Myxomas are benign neoplasms that are characterized
by slow growth (1). The most frequent
location of those neoplasms is the cardiac muscle, where they
account for 50% of all benign lesions (2). Myxoma is rare in the leg, but can occur
within its muscles (1). To date,
<10 cases of myxoma located in the leg have been documented
(1,3–5). Computed
tomography usually shows a well-delimited mass with an absorption
density between that of muscle and water. The most precise
examination technique that enables diagnosis is magnetic resonance
(MR) imaging (6,7), and radical removal of the whole lesion
is the most effective method of treating myxomas (8). The present study reports a case of
myxoma localized to the leg and interlinked with the pelvic cavity,
which was treated with palliative surgery. To the best of our
knowledge, this study is the first to describe the possibility of a
leg myxoma originating from an appendiceal mucinous neoplasm.
Case report
An 88-year-old female was hospitalized at Yantai
Affiliated Hospital of Binzhou Medical University (Yantai, China)
in January 2014 with a large tumor in the right upper leg. The
tumor had existed for 15 years and had ulcerated through the skin 4
days prior to admittance. The function and appearance of the right
lower limb were seriously affected. Laboratory examinations showed
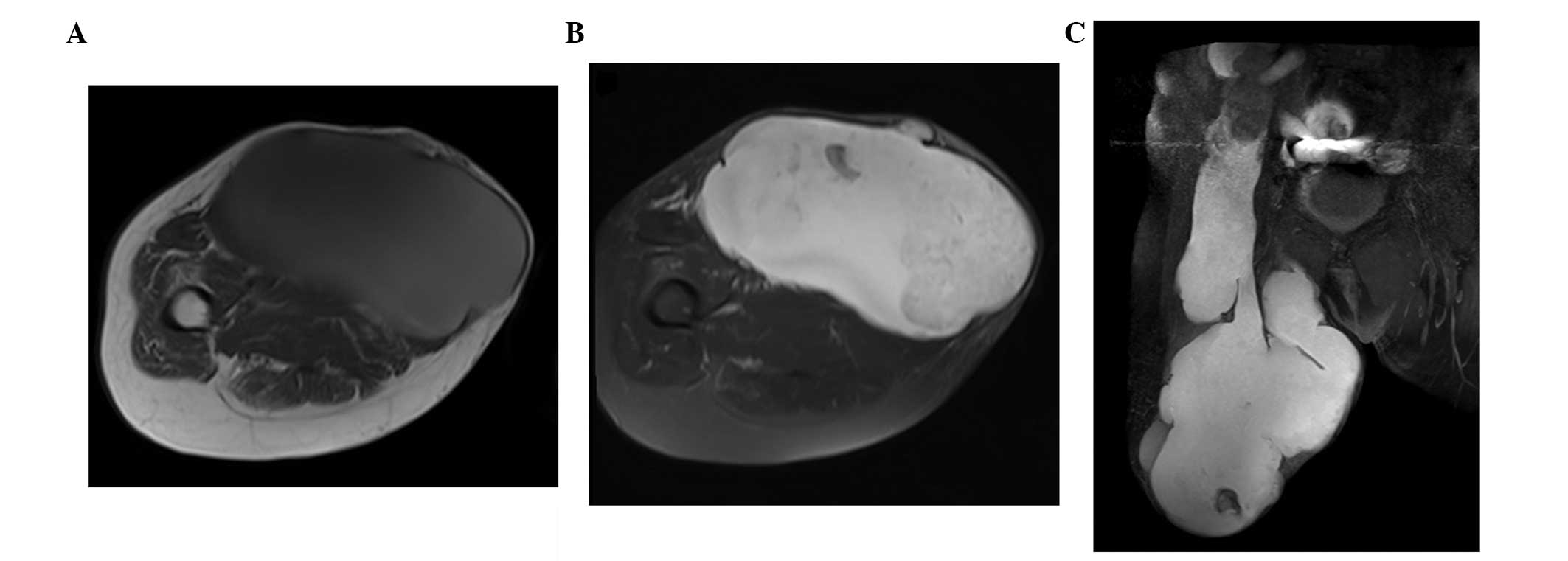
no abnormalities and no other symptoms were observed. The MR
studies were performed by a SIEMENS Avanto 1.5T MR scanner. A large
tumor (45×15×20 cm) in the right thigh was found with a slight high
signal on T1-weighted imaging (Fig.
1A) and an appreciable high signal on T2-weighted imaging
(Fig. 1B). The tumor extended to the
pelvic cavity and was found to be connected with a cystic and solid
neoplasm (Fig. 1C). Due to the older
age of the patient, total resection was considered to be too
traumatic. Instead, the patient underwent palliative surgery for
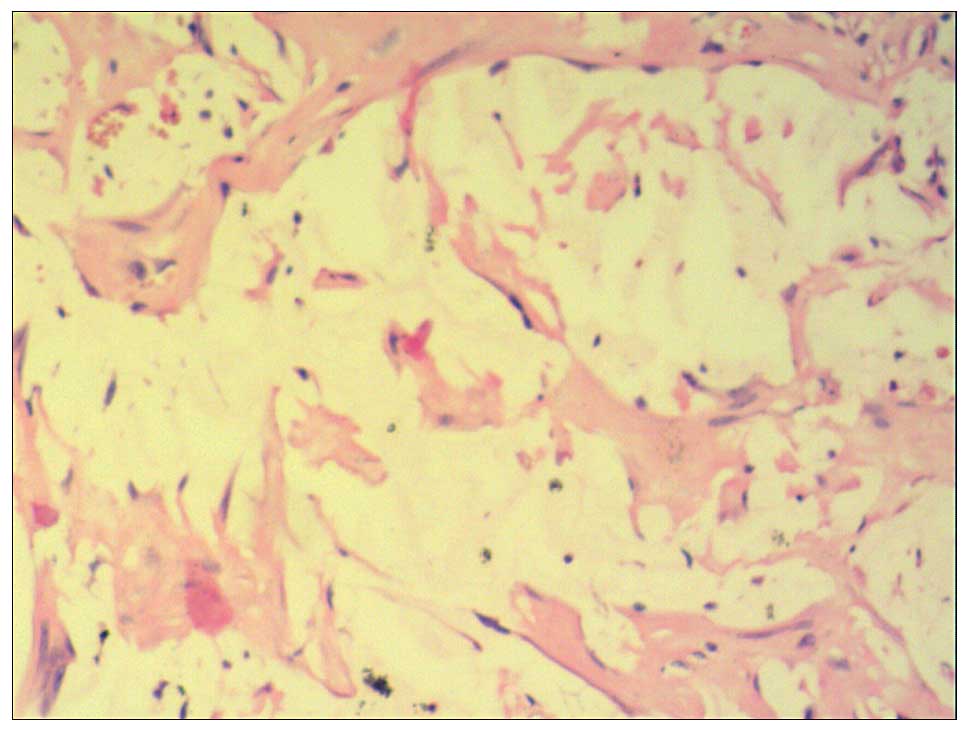
the tumor in the upper leg, and the tumor was found to be full of
brown and yellow gelatinous material. Myxoma was finally diagnosed
via histological examination (Fig.
2). Following surgery, the patient recovered well and was
subsequently discharged. The patient rejected further treatment and
no follow-up examination was planned. At the time of writing, the
patient was alive.
This study was approved by the Ethics Committee of
Binzhou Medical University (Yantai, Shandong, China) and written
informed consent was obtained from the patient.
Discussion
Myxoma is rare in the upper leg (3). Similarly to a previous study (1), the growth of the myxoma in the present
case was slow. A plain X-ray may be normal or rarely visualize the
lesion within the soft tissues as shading with calcifications
inside (9). An ultrasonographic
examination usually visualizes hypoechogenic lesions with fluid
compartments located within the muscles. Computed tomography
usually shows a well-delimited mass with an absorption density
between that of muscle and water. The most precise examination
technique that enables diagnosis is magnetic resonance imaging
(6,7).
Similarly to previous studies (1,6,9), the myxoma in the present study had a
sharply defined border. In addition, it exhibited a signal
intensity lower than that of the skeletal muscles on T1-weighted
images and brighter than adipose tissue on T2-weighted images.
In the present case, the large tumor of the thigh
was interlinked with the pelvic cavity. It is important to observe
the association between the lesion and pelvic organs, such as the
appendix or ovaries, as appendiceal mucinous neoplasm may invade
organizations outside of the mucous layer of the appendix and cause
secondary peritoneal myxoma (10).
Inside the mucus, epithelial cells rich in secretory functions can
be found (11). In the present case,
no epithelial cells were found through pathological examination.
The reason for this may be associated with an inadequate local
palliative surgery.
The patient rejected further treatment and no
follow-up examination was planned. Since the tumor extended to the
pelvic cavity and was found to be connected with a cystic and solid
neoplasm that was adjacent to the ascending colon in the right
lower quadrant, this case of myxoma probably originated from an
appendiceal mucinous neoplasm.
In conclusion, the present study showed that the
growth of myxoma is slow, with a long disease course. Furthermore,
appendiceal mucinous neoplasms may invade outside of the mucosal
layer of the appendix, leading to secondary myxoma, which may
extend to the leg, as observed in the present study.
References
|
1
|
Spychała A, Murawa D and Niziołek A:
Intramuscular myxoma of the left leg - Case report of the lesion
observed for several years. Rep Pract Oncol Radiother. 16:71–74.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Reynen K: Cardiac myxomas. N Engl J Med.
333:1610–1617. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Luna A, Martinez S and Bossen E: Magnetic
resonance imaging of intramuscular myxoma with histological
comparison and a review of the literature. Skeletal Radiol.
34:19–28. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ganchev G and Kunev S: A case of myxoma of
the left leg with malignant clinical course. Khirurgiia (Sofiia).
20:166–168. 1967.(In Bulgarian). PubMed/NCBI
|
|
5
|
Avninder S, Ramesh V and Vermani S: Benign
nerve sheath myxoma (myxoid neurothekeoma) in the leg. Dermatol
Online J. 13:142007.PubMed/NCBI
|
|
6
|
Murawa D, Gowin E, Pawelska A and Murawa
P: Cases of giant retroperitoneal liposarcomas. Rep Pract Oncol
Radiother. 10:147–151. 2005. View Article : Google Scholar
|
|
7
|
VanRoggen J, McMenamin M and Fletcher D:
Cellular myxoma of soft tissue: A clinicopathologic study of 38
cases confirming indolent clinical behaviour. Histopathology.
39:287–297. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Luebke AM, Gocke C, Priemel M, Grob TJ and
Zustin J: Intramuscular myxoma of the lower leg. Pathologe.
34:360–363. 2013.(In German). View Article : Google Scholar : PubMed/NCBI
|
|
9
|
McCook T, Martinez S, Korobkin M, Ram PC,
Bowen JH, Breiman RS, Harrelson JM and Gehweiler JA Jr:
Intramuscular myxoma. Radiographic and computed tomographic
findings with pathologic correlation. Skeletal Radiol. 7:15–19.
1981. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Honnef I, Moschopulos M and Roeren T:
Appendiceal mucinous cystadenoma. Radiographics. 28:1524–1527.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Caracappa D, Gullà N, Gentile D, Listorti
C, Boselli C, Cirrochi R, Bellezza G and Noya G: Appendiceal
mucocele. A case report and literature review. Ann Ital Chir.
82:239–245. 2011.PubMed/NCBI
|