Introduction
Solitary plasmacytoma (SP) is a rare plasma cell
dyscrasia that is characterized by the presence of bone or
extramedullary monoclonal plasma cell tumors, without evidence of
multiple myeloma (MM) (1). According
to the location, SP can be categorized into two groups: Solitary
plasmacytoma of the bone (SPB) and extramedullary plasmacytoma
(EMP) (1). EMP accounts for 3–5% of
all plasma cell tumors, with an incidence of only 0.04 cases per
100,000 individuals (2).
Approximately 80% of EMPs occur in the upper respiratory tract
(3), but they can also occur in
numerous other sites (3,4), including the gastrointestinal tract
(5,6),
brain (7), orbits (8), thyroid gland (9), breasts (10), lungs (11), pleura (12), kidneys (13),bladder (14), urethra (15), ovaries (16), testes (17) and skin (18). Usually, EMPs have no specific clinical
manifestations. They typically present as well-localized submucosal
masses or swellings in the fifth to seventh decades of the life,
with a male to female ratio of 3:1 (3). As the majority of patients can be cured
by local radiotherapy, EMP carries an optimistic prognosis, with
only 5–20% recurrence (3,4,5,19).
EMP in the vulva is extremely rare (20) and to the best of our knowledge, no
case involving the labia majora has previously been reported. The
present study describes the first case of EMP occurring in the left
labia majora in a young female during early pregnancy. The
strengths of the case were the uncommon location and the function
preservation treatment strategy. Written informed consent was
obtained from the patient for inclusion in the present study.
Case report
In November 2013, a 36-year-old female (gravida 2,
para 1) in the seventh week of pregnancy presented to the West
China Hospital (Chengdu, China) with a gradually enlarging mass on
the left labia majora, accompanied by ulceration and pain that had
persisted for 2 months since August 2013. The mass presented as a
small nodule ~2 cm in diameter at the onset, with a rough surface
and tenderness, which quickly expanded to the whole left labia
majora and ulcerated with a purulent exudate. The diagnosis of a
vulvar ulcer was made previously in a local hospital in October
2013, therefore, anti-inflammation treatment with intravenous
benzylpenicillin (3 million units every 8 h for 10 consecutive
days) and debridement were performed. However, the symptoms were
not alleviated and the patient was subsequently transferred to the
West China Hospital.
Upon admission to the West China Hospital in
November 2013, an irregular 7×4×2-cm mass was found in the left
labia majora, with blood scabs and a purulent exudate. The mass was
hard and tender on palpation. There were no palpable inguinal lymph
nodes. The patient reported persistent spontaneous pain with a
score of 6 in the numerical rating scale (21).
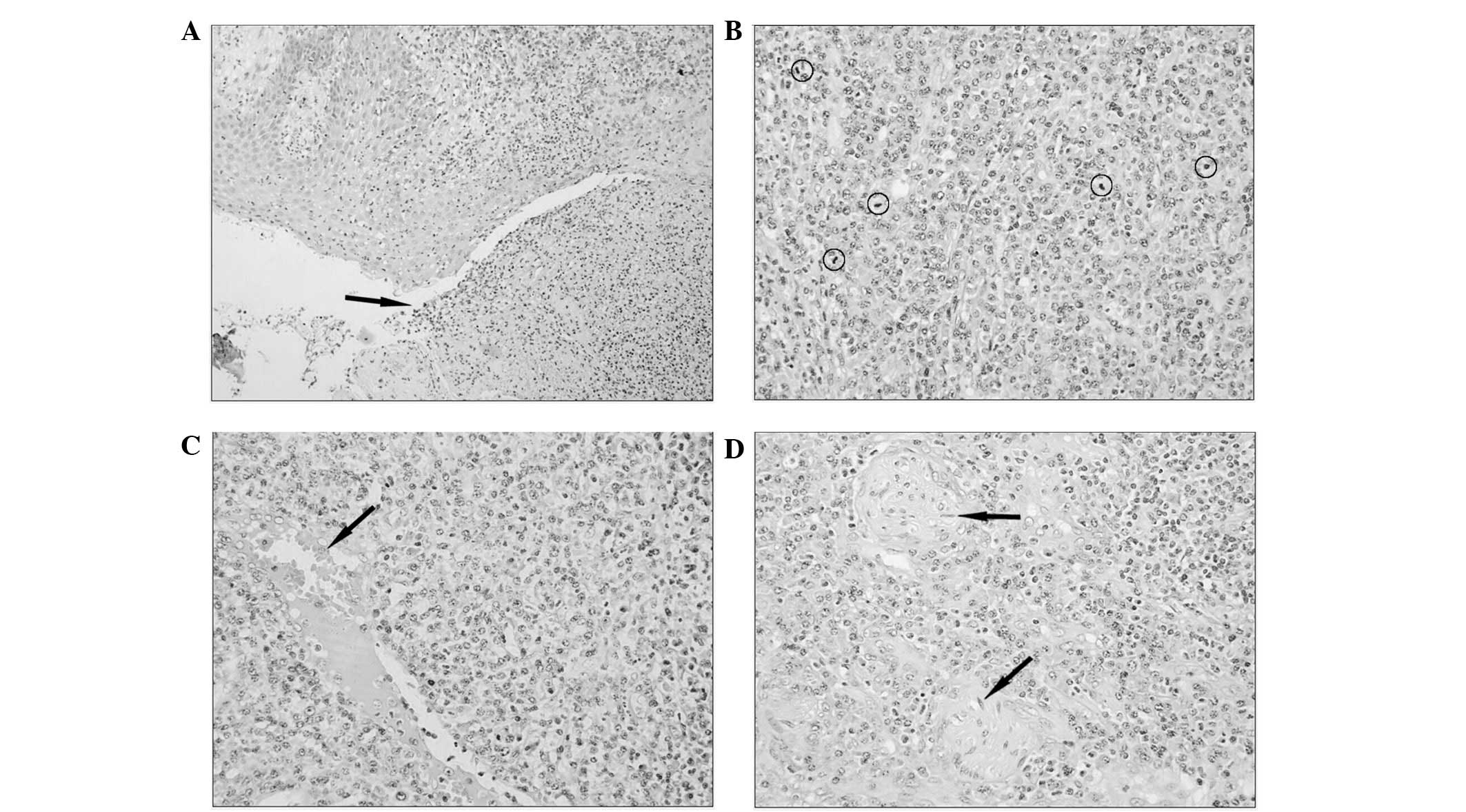
A biopsy was performed and the histopathology
results revealed a diffuse infiltration of plasmacytoid cells in
the dermis and subcutaneous tissue, a number of which invaded the
nerves and vessels (Fig. 1). The
cells were positive for cluster of differentiation (CD)79a and
κ-light chain, partly positive for CD132, and negative for CD20,
λ-light chain, CD23, CD5, CD3, B-cell lymphoma (Bcl)-2, Bcl-6 and
CD10. Ki-67 staining revealed a high cell proliferation rate with
~50% immunoreactive cells. No monoclonal gene rearrangement of
immunoglobulin (Ig)H or IgK was detected. Therefore, a diagnosis of
EMP was proposed.
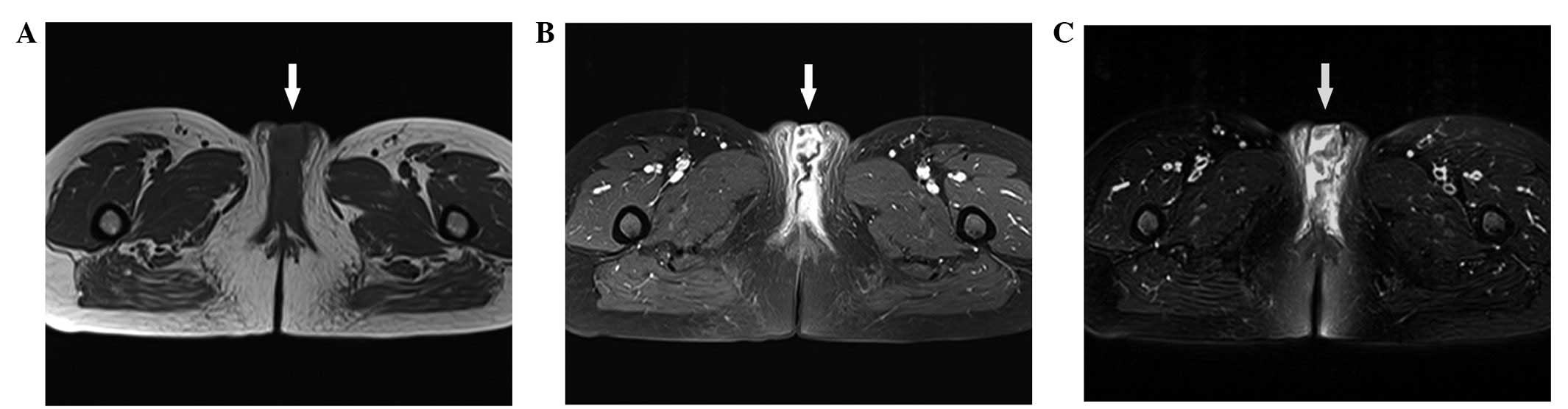
Subsequently, an extensive medical workup was
performed to delineate the extent of the lesion and to rule out
coexistence with MM. As the patient had decided to terminate the
pregnancy, imaging examinations were conducted. An irregular mass
with mixed signals and without lymphadenopathy was found on
magnetic resonance imaging (MRI) (Fig.
2). No metastases were found on chest and abdominal computed
tomography (CT) scans. A normal result with only 0.5% plasma cells
was yielded upon bone marrow aspiration and biopsy. No bone lesions
were found on bone single-photon emission CT. No anemia,
hypercalcemia or renal impairment were detected. Serum
electrophoresis did not show the M-band and Bence-Jones proteinuria
was not detected. Serum albumin and Ig levels were normal, and
serum and urinary β2 microglobulin levels were unremarkable. On the
basis of these results, a definitive diagnosis of EMP was
established.
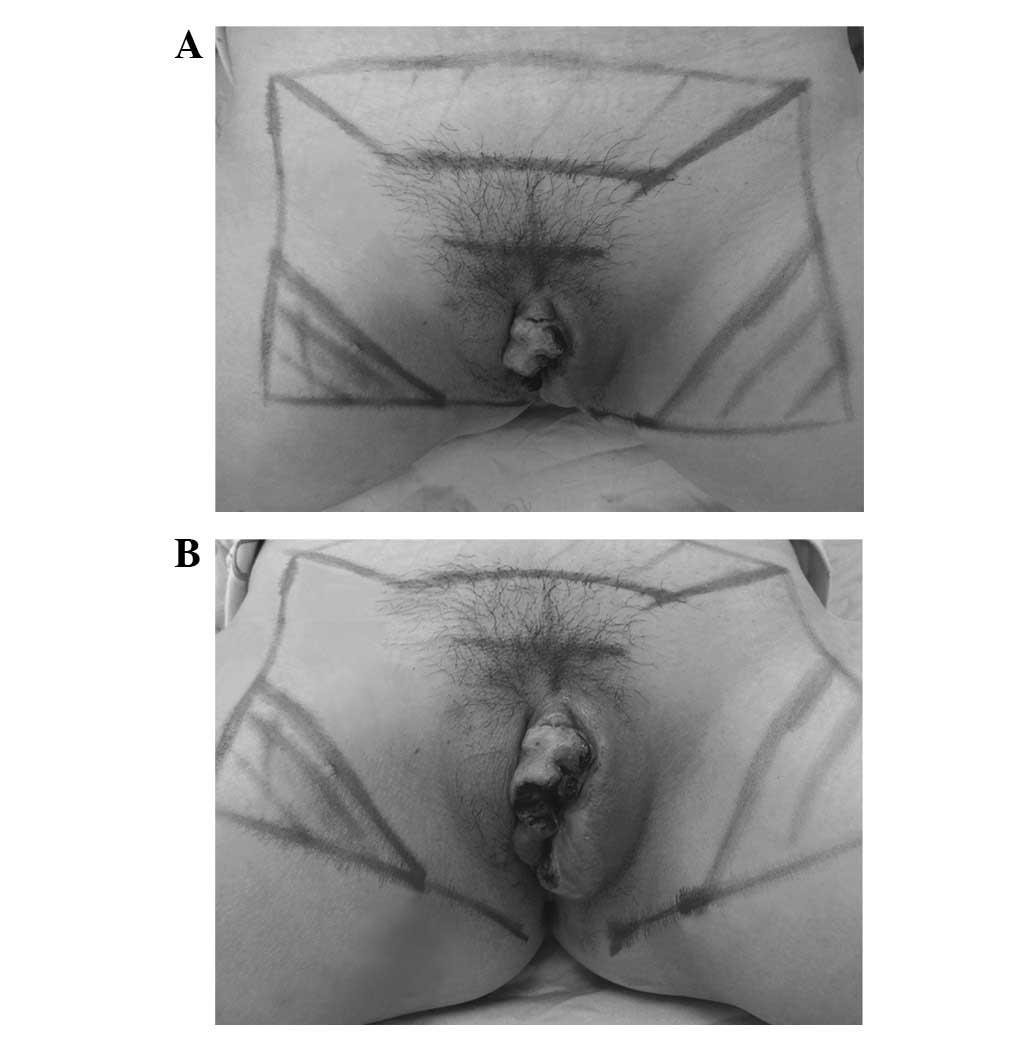
Following termination of the pregnancy,
pre-operative external irradiation with a 6-MV photon beam though
an anterior portal was applied to the vulvar area and the
inguinofemoral lymph nodes (Fig. 3)
using daily fractionation of 200 cGy in five fractions weekly (21
fractions in total), except for the third fraction in which 500 cGy
was adopted due to aggravated pain. Dynamic observations of the
mass were made every week. No severe moist desquamation or
maceration of the perineal skin occured. The total 4,500-cGy
treatment was completed over 32 days, and compared with the initial
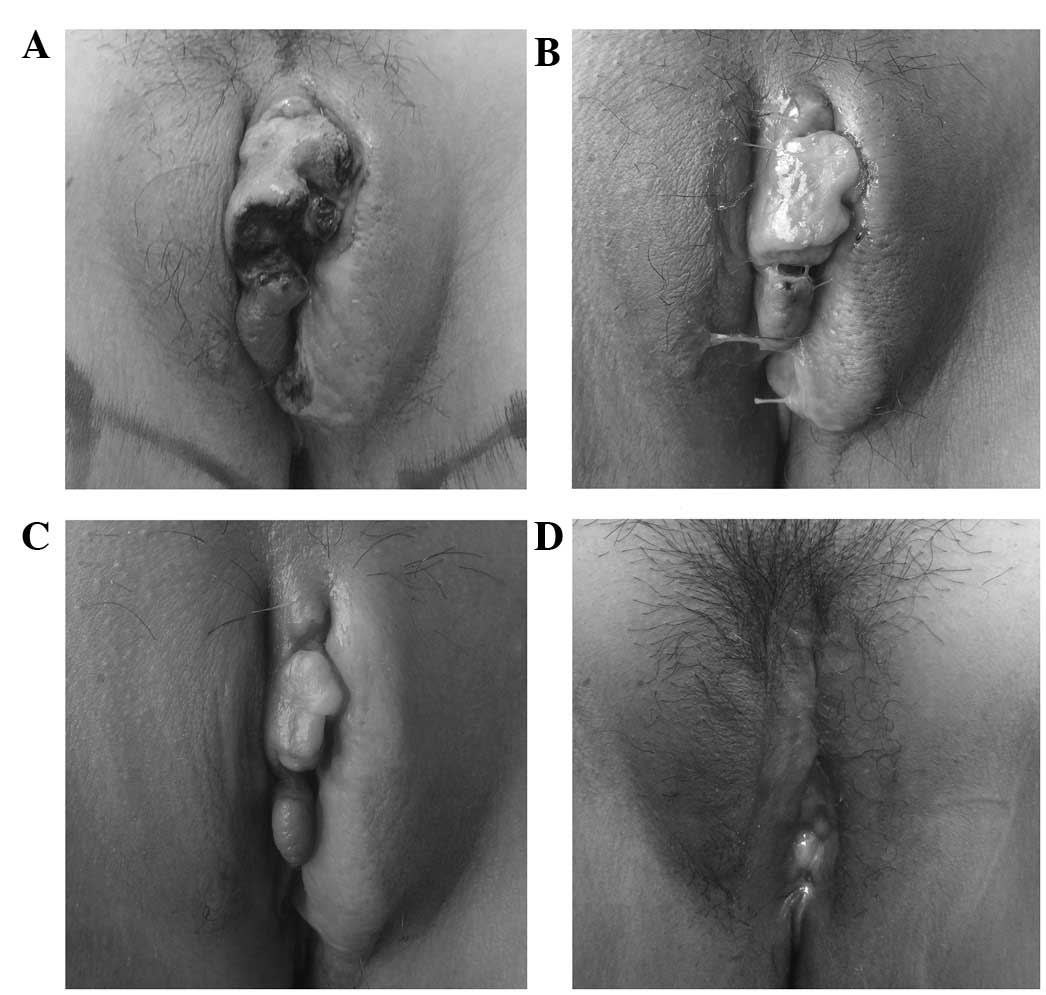
presentation (Fig. 4A), the tumor was
satisfactorily reduced in size (Fig.
4B).
 | Figure 4.Vulvar appearances prior to, during
and following treatment. (A) 3 days prior to radiotherapy, an
irregular mass ~7×4×2 cm in size was present in the swollen left
labia majora, with blood scabs and a purulent exudate. (B) 1 day
after radiotherapy, the mass had been reduced in volume by
two-thirds, but more exudate was present. (C) 41 days after
radiotherapy and 2 days prior to surgery, the mass had been further
reduced in size, and only two nodules, ~2×1×1 and 1×0.5×0.5 cm in
size, remained. The acute edema had disappeared. (D) 2 months after
surgery, the vulvar appearance had returned basically to
normal. |
Subsequently, 40 days later, the mass had further
decreased in size and only two small nodules existed (Fig. 4C). The mass was reevaluated and the
surgical timing was appropriate. An extended local excision and
anaplasty of the vulva was performed. As the post-operative
pathology confirmed that no tumor cells were present,
post-operative boost irradiation was not performed. The
post-operative course was uneventful (Fig. 4D) and the patient was advised to
attend regular follow-ups every 3 months. At 9 months post-surgery,
there was no evidence of local recurrence, distant metastasis or
progression to MM. The patient has continued to maintain a
satisfactory sexual life.
Discussion
EMP of the labia majora is extremely rare. The
current study presents, to the best of our knowledge, the first
documented case of human EMP involving the labia majora and the
first such case presenting during pregnancy. A thorough literature
search in Pubmed found only one study reporting a case of
simultaneous EMPs of the vagina and right labia minora, with a
literature review of four cases invading the vagina and with a
mention of three vulvar plasmacytomas (20). However, the present case is reported
not only for its uncommon location, but also for its tortuous
diagnosis, treatment strategy and close follow-up.
The differential diagnosis should be kept in mind
and rare diseases should be considered when diagnosing all masses.
Due to the rare occurance and variety of clinical manifestations of
EMP, an accurate diagnosis is often delayed. In the present case,
the patient was initially misdiagnosed with a vulvar ulcer in a
local hospital. In fact, the main feature of the disease was the
progressively enlarging mass, while the ulceration was only an
accompanying symptom. When treatment effectiveness cannot be
achieved, rare diseases should be considered. Pathological biopsy,
a golden criteria of diagnosis, is essential for improving
diagnostic accuracy.
An EMP was proposed on the basis of diffuse
monoclonal plasma cell infiltration in the biopsy tissue of the
present patient. Once EMP is proposed by pathology, a medical
workup should be arranged to exclude existence of MM. The
recommended diagnostic criteria for EMP are: i) A single
extramedullary mass of clonal plasma cells; ii) histologically
normal bone marrow aspirate and trephine; iii) normal results on
skeletal survey, including radiology of the long bones; iv) no
anemia, hypercalcaemia or renal impairment due to plasma cell
dyscrasia; and v) an absent or low serum or urinary level of
monoclonal Ig (22). In the present
case, all relevant tests had been conducted to exclude coexistence
with MM.
Due to the small number of patients and lack of
randomized controlled trials, there are no established criteria for
the treatment of EMP. However, radiotherapy is considered as the
mainstay due to the high radiosensitivity of EMP, particularly in
the head and neck area where resection is limited by the anatomical
complexity. Several series have reported 80–100% local control
rates (4,5,19,23–27). The
optimal radiation dose recommended by the United Kingdom Myeloma
Forum is in the range of 40–50 Gy (22,25). A
dose of 40 Gy in 20 fractions can confer an excellent chance of
local control in tumors that are ≤5 cm in diameter, whereas a
higher dose of ~50 Gy in 25 fractions is required in tumors >5
cm due to a higher risk of local failure (27,28). The
necessity of prophylactic irradiation of local lymph nodes is
unclear, as excellent results could be achieved with elective
inclusion of the draining lymph nodes (26) and inclusion of them only when
clinically involved (27,29). Complete surgical excision can be
considered at other sites outside the head and neck area if
feasible. A combination of radiotherapy with surgery has been
demonstrated to be less invasive and to produce better overall
survival (30). The role of adjuvant
chemotherapy is inconclusive and additional use of it may bring
certain benefits to patients with large masses and high-grade
histology (22).
For the present patient, radiotherapy dominated the
treatment not only due to its effectiveness, but also due to the
advantage of function preservation. If surgery had been adopted
first, the destruction of the vulvar appearance or even function
may have caused major psychosexual problems in this patient of
reproductive age. A moderate dose of 4,500 cGy was considered
enough due to its predetermined combination with the subsequent
radical surgery. The inguinal lymph node region was
prophylactically irradiated for safety. It is noteworthy that the
temporary adjustment to 500 cGy irradiation for the third fraction
contributed greatly to the pain relief without injury to the
urethra. The external location of the tumor made direct
observation, without the requirement for CT or MRI, easy.
Therefore, the change in tumor size and appearance demonstrated
vividly the radiosensitivity of EMP, which has been rarely reported
in other cases. Surgical timing was determined to be appropriate ~1
month after radiotherapy to avoid acute edema immediately after
radiotherapy and to make best use of the late effect of
radiotherapy. Overall, as indicated in the present case, the
primary treatment for the majority of patients will be
radiotherapy, but surgery may also be required. Close communication
between the hematologist, radiotherapist and surgeon is therefore
vital for providing optimum care.
EMP has the best prognosis of all plasma cell
tumors. The 5-year overall survival rate varies between 31 and 82%
(5,25,29,31,32).
However, unlike other tumors in which attention is focused more on
relapse and distant metastasis during follow-up, EMP requires extra
attention with regard to progression to MM, as the majority of
mortalities associated with EMP are due to this conversion.
Compared with SPB, progression of EMP to MM occurs less frequently.
Approximately 60% of patients with SPB develop MM (27,28,33) while
EMP progresses to MM in 5–44% of cases (3,5,23,28,29,33,34).
Although progression to MM usually occurs within 2 years of the
initial diagnosis, conversion has occurred up to 15 years later
(3,5,19,23,30).
Therefore, the long-term regular evaluation of patients with EMP is
strongly recommended. A physical examination, imaging of the
primary site, bone marrow aspiration and biopsy, radiographic
studies of the skeleton, serum protein electrophoresis, free light
chain assays and laboratory tests, including a complete blood
count, renal function tests, and analyses of blood calcium, serum
albumin and Ig levels, are required during follow-ups.
In conclusion, the present study, for the first
time, reports a case of EMP involving the left labia majora in a
pregnant woman. The combination of irradiation and surgery leads to
excellent tumor control and function preservation. Regular
follow-ups should be performed in such patients in case of relapse,
metastasis or progression to MM.
References
|
1
|
Galieni P, Cavo M, Avvisati G, Pulsoni A,
Falbo R, Bonelli MA, Russo D, Petrucci MT, Bucalossi A and Tura S:
Solitary plasmacytoma of bone and extramedullary plasmacytoma: Two
different entities? Ann Oncol. 6:687–691. 1995.PubMed/NCBI
|
|
2
|
Perez CA: Unusual nonepithelial tumors of
the head and neck. Principles and Practice of Radiation Oncology.
Perez CA and Brady LW: (3rd). Lippincott Raven Publishers.
(Philadelphia). 1116–1117. 1997.
|
|
3
|
Alexiou C, Kau RJ, Dietzfelbinger H,
Kremer M, Spiess JC, Schratzenstaller B and Arnold W:
Extramedullary plasmacytoma: Tumor occurrence and therapeutic
concepts. Cancer. 85:2305–2314. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Chao MW, Gibbs P, Wirth A, Quong G, Guiney
MJ and Liew KH: Radiotherapy in the management of solitary
extramedullary plasmacytoma. Intern Med J. 35:211–215. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Liebross RH, Ha CS, Cox JD, Weber D,
Delasalle K and Alexanian R: Clinical course of solitary
extramedullary plasmacytoma. Radiother Oncol. 52:245–249. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Galieni P, Cavo M, Pulsoni A, Avvisati G,
Bigazzi C, Neri S, Caliceti U, Benni M, Ronconi S and Lauria F:
Clinical outcome of extramedullary plasmacytoma. Haematologica.
85:47–51. 2000.PubMed/NCBI
|
|
7
|
Manabe M, Kanashima H, Yoshii Y, Mukai S,
Sakamoto E, Iwai Y, Kubo Y, Fukushima H, Inoue T and Teshima H:
Extramedullary plasmacytoma of the dura mimicking meningioma. Int J
Hematol. 91:731–732. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Duletic-Nacinovic A, Stifter S, Marijic B,
Miletic D, Loncarek K, Manestar D and Jonjic N: Dacryocystitis
provoked by recurrence of extramedullary plasmacytoma of the orbit:
A case report. Tumori. 96:164–167. 2010.PubMed/NCBI
|
|
9
|
Puliga G, Olla L, Bellisano G, Di Naro N,
Ganau M, Lai ML, Faa G and Tolu GA: Solitary extramedullary
plasmacytoma of the thyroid gland associated with multinodular
goiter: Case report and review of the literature. Pathologica.
103:61–63. 2011.PubMed/NCBI
|
|
10
|
De Chiara A, Losito S, Terracciano L, Di
Giacomo R, Iaccarino G and Rubolotta MR: Primary plasmacytoma of
the breast. Arch Pathol Lab Med. 125:1078–1080. 2001.PubMed/NCBI
|
|
11
|
Ujiie H, Okada D, Nakajima Y, Yoshino N
and Akiyama H: A case of primary solitary pulmonary plasmacytoma.
Ann Thorac Cardiovasc Surg. 18:239–242. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Feng PH, Huang CC, Wang CW, Wu YK and Tsai
YH: Solitary pleural plasmacytomas manifested as a massive pleural
effusion without evidence of monoclonal gammopathy. Respirology.
13:751–753. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zhang SQ, Dong P, Zhang ZL, Wu S, Guo SJ,
Yao K, Li YH, Liu ZW, Han H, Qin ZK, et al: Renal plasmacytoma:
Report of a rare case and review of the literature. Oncol Lett.
5:1839–1843. 2013.PubMed/NCBI
|
|
14
|
Khaliq W, Uzoaru I, Konchanin RP, Sapiente
RA and Egner JR: Solitary extramedullary plasmacytoma of the
bladder: A case report and literature. Oncology (Williston Park).
24:832–835. 2010.PubMed/NCBI
|
|
15
|
Klein T, Holz A, Neid M, Hinkel A and
Noldus J: The first description of an extramedullary plasmacytoma
of the ureter. Urol Int. 84:122–124. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Emery JD, Kennedy AW, Tubbs RR, Castellani
WJ and Hussein MA: Plasmacytoma of the ovary: A case report and
literature review. Gynecol Oncol. 73:151–154. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Iizumi T, Shinohara S, Amemiya H, Tomomasa
H, Yazaki T, Umeda T, Tanaka F and Imamura T: Plasmacytoma of the
testis. Urol Int. 55:218–221. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Koletsa T, Patsatsi A, Kostopoulos I,
Kartsios C, Korantzis I and Sotiriadis D: A case of a primary
cutaneous plasmacytoma presenting in adolescence. Am J
Dermatopathol. 34:537–540. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Bachar G, Goldstein D, Brown D, Tsang R,
Lockwood G, Perez-Ordonez B and Irish J: Solitary extramedullary
plasmacytoma of the head and neck-long-term outcome analysis of 68
cases. Head Neck. 30:1012–1019. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Doss LL: Simultaneous extramedullary
plasmacytomas of the vagina and vulva: A case report and review of
the literature. Cancer. 41:2468–2474. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Breivik H, Borchgrevink PC, Allen SM,
Rosseland LA, Romundstad L, Hals EK, Kvarstein G and Stubhaug A:
Assessment of pain. Br J Anaesth. 101:17–24. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Soutar R, Lucraft H, Jackson G, Reece A,
Bird J, Low E and Samson D: Guidelines Working Group of the UK
Myeloma Forum; British Committee for Standards in Haematology;
British Society for Haematology: Guidelines on the diagnosis and
management of solitary plasmacytoma of bone and solitary
extramedullary plasmacytoma. Br J Haematol. 124:717–726. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Michalaki VJ, Hall J, Henk JM, Nutting CM
and Harrington KJ: Definitive radiotherapy for extramedullary
plasmacytomas of the head and neck. Br J Radiol. 76:738–741. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Creach KM, Foote RL, Neben-Wittich MA and
Kyle RA: Radiotherapy for extramedullary plasmacytoma of the head
and neck. Int J Radiat Oncol Biol Phys. 73:789–794. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Tournier-Rangeard L, Lapeyre M,
Graff-Caillaud P, Mege A, Dolivet G, Toussaint B, Charra-Brunaud C,
Hoffstetter S, Marchal C and Peiffert D: Radiotherapy for solitary
extramedullary plasmacytoma in the head-and-neck region: A dose
greater than 45 Gy to the target volume improves the local control.
Int J Radiat Oncol Biol Phys. 64:1013–1017. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Bolek TW, Marcus RB Jr and Mendenhall NP:
Solitary plasmacytoma of bone and soft tissue. Int J Radiat Oncol
Biol Phys. 36:329–333. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Tsang RW, Gospodarowicz MK, Pintilie M,
Bezjak A, Wells W, Hodgson DC and Stewart AK: Solitary plasmacytoma
treated with radiotherapy: Impact of tumor size on outcome. Int J
Radiat Oncol Biol Phys. 50:113–120. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Holland J, Trenkner DA, Wasserman TH and
Fineberg B: Plasmacytoma. Treatment results and conversion to
myeloma. Cancer. 69:1513–1517. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Susnerwala SS, Shanks JH, Banerjee SS,
Scarffe JH, Farrington WT and Slevin NJ: Extramedullary
plasmacytoma of the head and neck region: Clinicopathological
correlation in 25 cases. Br J Cancer. 75:921–927. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Sasaki R, Yasuda K, Abe E, Uchida N,
Kawashima M, Uno T, Fujiwara M, Shioyama Y, Kagami Y, Shibamoto Y,
et al: Multi-institutional analysis of solitary extramedullary
plasmacytoma of the head and neck treated with curative
radiotherapy. Int J Radiat Oncol Biol Phys. 82:626–634. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Kapadia SB, Desai U and Cheng VS:
Extramedullary plasmacytoma of the head and neck. A
clinicopathologic study of 20 cases. Medicine (Baltimore).
61:317–329. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Miller FR, Lavertu P, Wanamaker JR,
Bonafede J and Wood BG: Plasmacytomas of the head and neck.
Otolaryngol Head Neck Surg. 119:614–618. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Mayr NA, Wen BC, Hussey DH, Burns CP,
Staples JJ, Doornbos JF and Vigliotti AP: The role of radiation
therapy in the treatment of solitary plasmacytomas. Radiother
Oncol. 17:293–303. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Katodritou E, Terpos E, Symeonidis AS,
Pouli A, Kelaidi C, Kyrtsonis MC, Kotsopoulou M, Delimpasi S,
Christoforidou A, Giannakoulas N, et al: Clinical features, outcome
and prognostic factors for survival and evolution to multiple
myeloma of solitary plasmacytomas: A report of the Greek myeloma
study group in 97 patients. Am J Hematol. 89:803–808. 2014.
View Article : Google Scholar : PubMed/NCBI
|