Introduction
Globally, ~500,000 cases of cervical cancer are
diagnosed per year, which accounts for 5% of all cases of cancer
diagnosed worldwide. The majority of these cases (>80%) occur in
developing countries (1,2). Direct invasion is the main method for
the diffusion of cervical cancer, followed by lymphatic metastasis,
whereas hematogenous diffusion rarely occurs (3). Tumor cell hematogenous diffusion is a
typical symptom of terminal cervical cancer. Common sites of such
diffusion are the lungs, bones, aorta, and the celiac and
supraclavicular lymph nodes, whereas kidney metastases are rare
(4). To the best of our knowledge, 9
cases of renal metastasis originating from cervical carcinoma have
been reported thus far (5–13), and 5 of these were initially
misdiagnosed as other kidney-associated diseases (6,8,10–12).
Currently, no general treatment consensus exists for the treatment
of renal metastases originating from cervical carcinoma. In the
present study, the case of a 51-year-old female with a metastatic
renal tumor originating from cervical carcinoma is described, and
the existing strategies for the treatment of this condition are
discussed. Written informed consent was obtained from the patient's
husband for publication of the present study.
Case report
In February 2011, a 48-year-old female who was
diagnosed with stage IIB cervical squamous-cell carcinoma underwent
chemoradiotherapy (pelvic radiation, 24 fractions at 200
cGy/fraction; intraoperative radiotherapy, 7 fractions at 600
cGy/fraction; and chemotherapy, 60 mg docetaxel twice/week) in the
Department of Gynecology, Hunan Provincial Tumor Hospital (The
Affiliated Tumor Hospital of Xiangya Medical College, Central South
University, Changsha, Hunan, China).
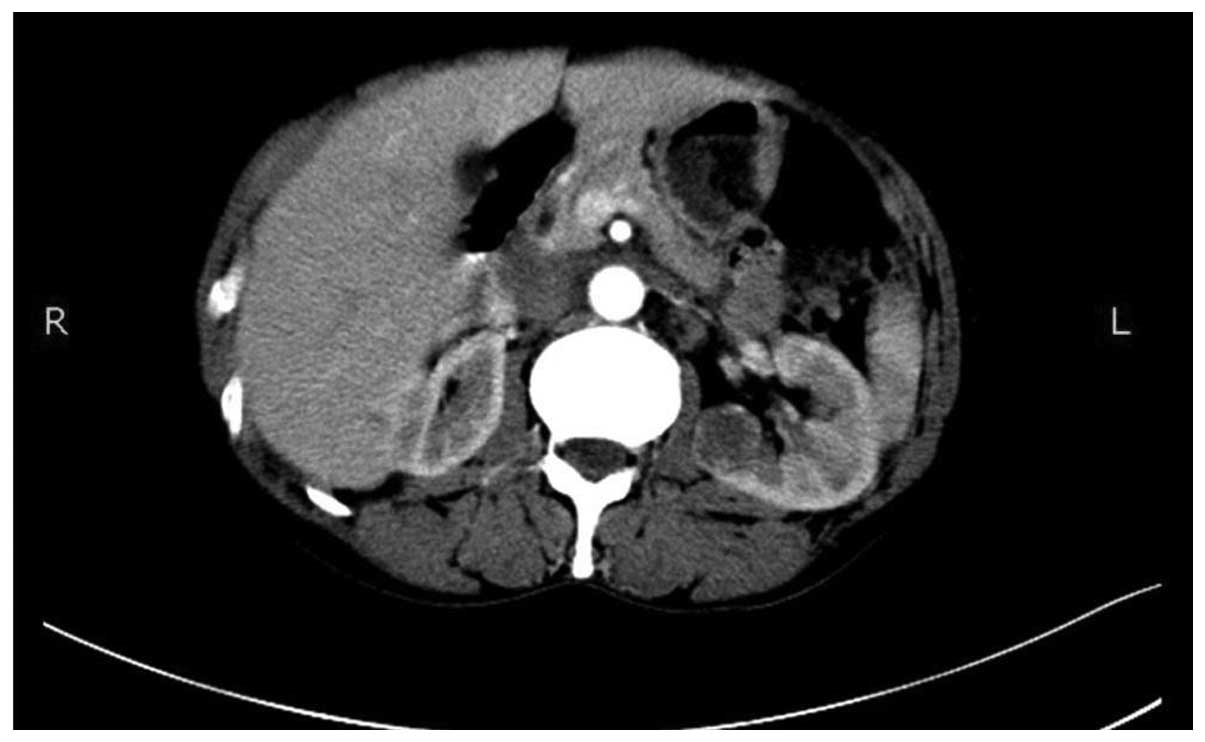
On June 19th, 2013, during follow-up abdominal
computed tomography (CT) examination, a low-density cystic mass
with homogenous density and clear borders was identified
post-operatively in the left kidney, which was interpreted as a
renal cyst (Fig. 1).
On July 22nd, 2014, the patient consulted the Hunan
Provincial Tumor Hospital due to gross hematuria, a fever of
unknown origin (FUO) and left abdominal pain. The findings at the
time of admission were as follows: Axillary temperature, 38.8°C
(normal, 36.0–37.0°C); heart rate, 84 beats/min (normal, 60–100
beats/min); and blood pressure, 103/73 mmHg (normal, 120/90–90/60
mmHg). Laboratory studies revealed the following results: A
decreased red blood cell count of 2.93×1012 cells/l
(normal, 3.5–4.5×1012 cells/l), a decreased level of
hemoglobin level of 97 g/l (normal, 110–150 g/l), tumor-specific
growth factor (normal, 0–64 µmol/l), carcinoembryonic antigen
(normal, ≤5.00 ng/ml), α-fetoprotein (normal, 0–20 ng/l) and human
chorionic gonadotropin (normal, <3.00 mIU/l) levels of 60.60
µmol/l, 0.92 mg/l, 1.36 ng/ml and 0.35 mIU/l, respectively, and
high levels of high-sensitivity C-reactive protein at 41.77 mg/l
(normal, <6.00 mg/l)..
Intravenous pyelogram demonstrated distortion and
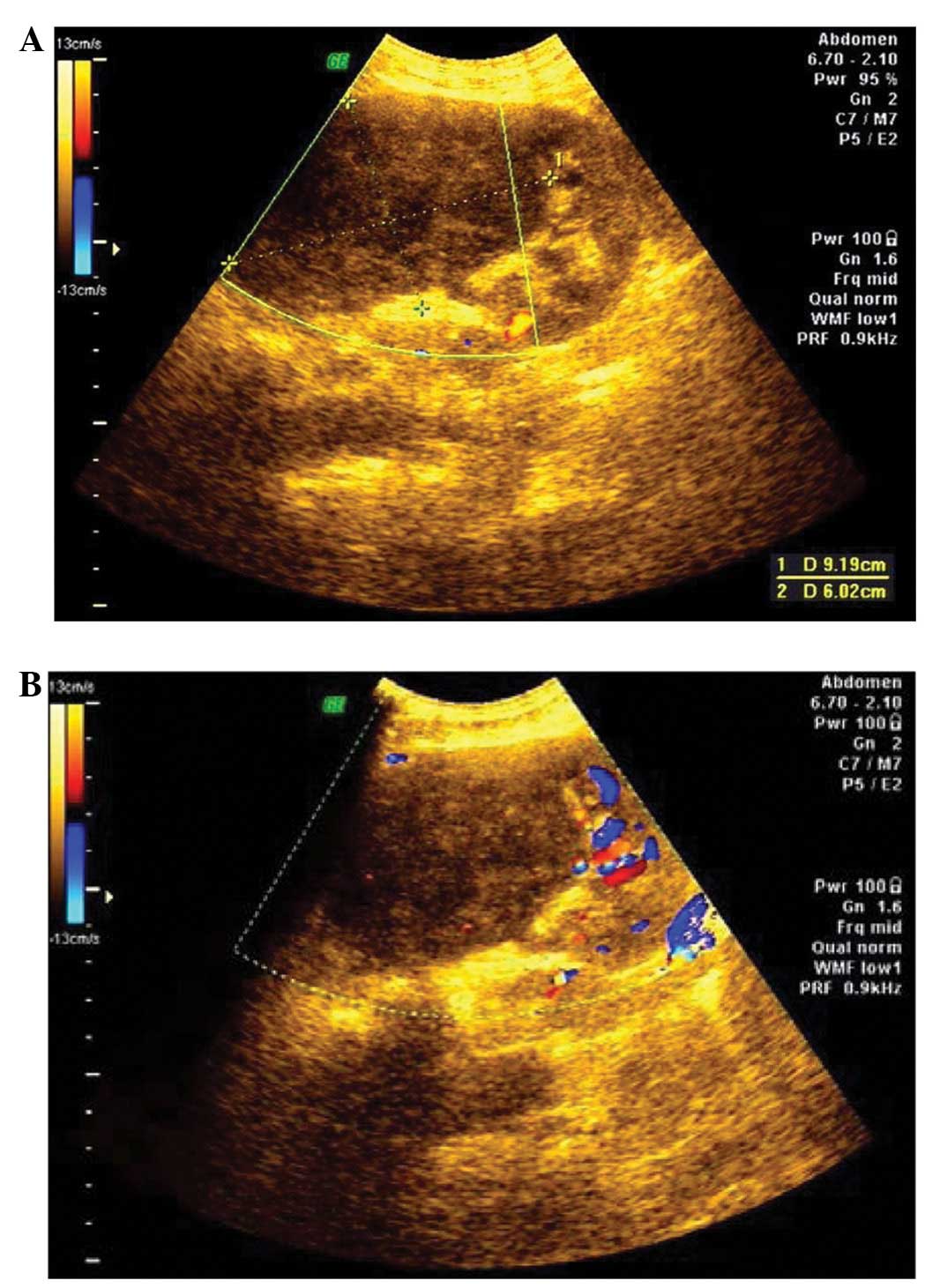
compression of the upper pole of the left kidney (Fig. 2). Abdominal ultrasound identified a
90×60-mm space-occupying lesion in the upper pole of the left
kidney. Signals of intratumoral blood flow were detected by color
Doppler ultrasound (Fig. 3).
Abdominal CT detected irregular low-density nodules in the left
kidney and heterogeneous enhancement on enhanced CT (Fig. 4). Additionally, the results of X-ray
analysis were negative, the Eastern Cooperative Oncology Group
performance status was 1 point (14)
and the right renal function was adequate.
A left renal nephrectomy was performed 9 days after
the admission date. The size of the phyma was 80×60×80 mm.
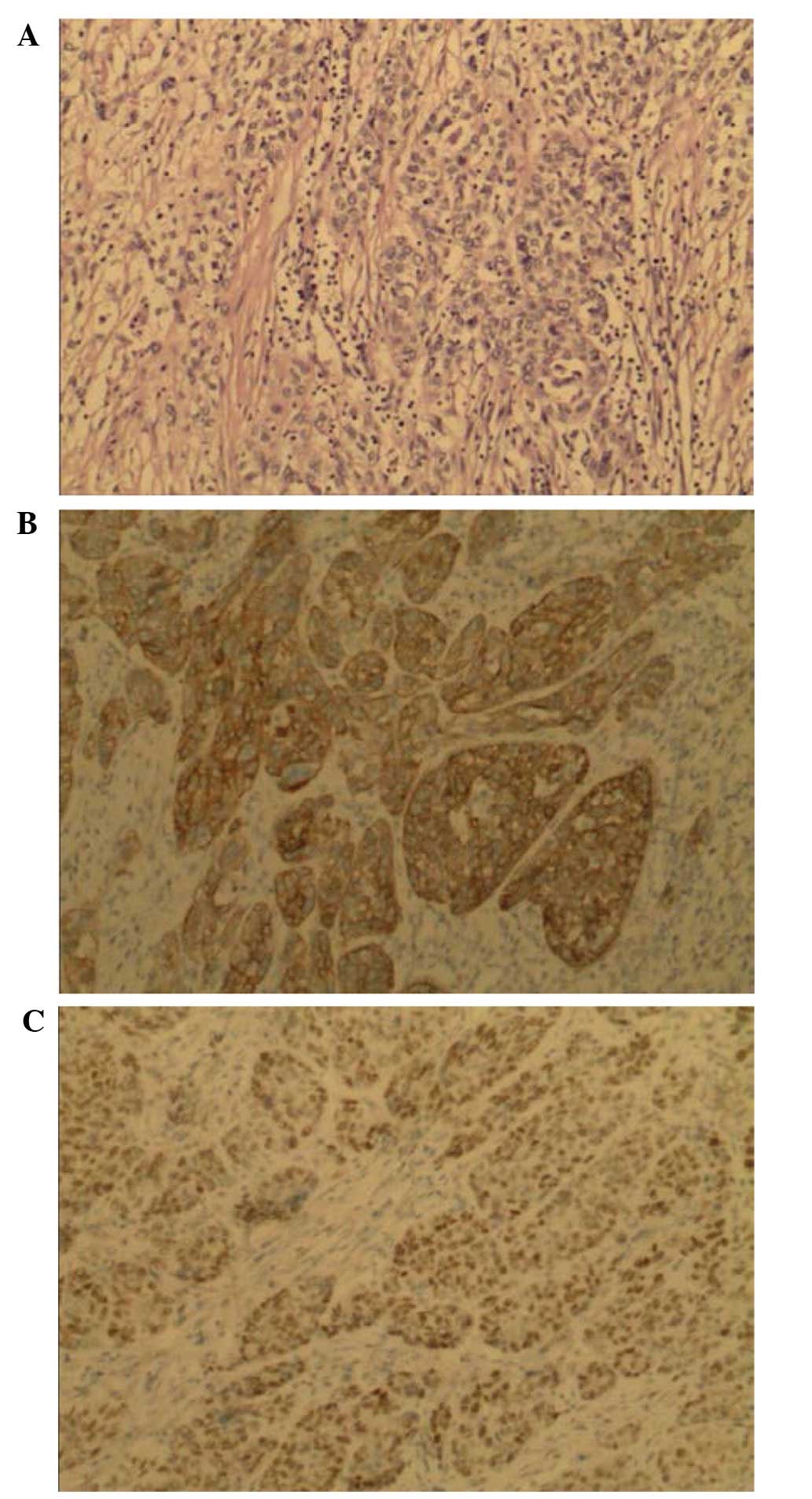
Pathological analysis showed that the sections of kidney were
predominately composed of squamous cells that were similar to the
pattern of the original cervical carcinoma (Fig. 5A). Immunohistochemical analysis
indicated that the squamous cell components were positive for
cytokeratin 5/6 (Fig. 5B) and p63
(Fig. 5C). Thus, pathological and
immunohistochemical examination confirmed a diagnosis of metastatic
squamous cell carcinoma, which was histologically consistent with
the original cervical carcinoma experienced by the patient 3 years
prior.
On November 21st, 2014, the imaging results were
positive for the disease in the lungs and multiple retroperitoneal
lymph nodes. The patient consequently refused to continue with the
treatment and was discharged from the hospital.
Discussion
Metastatic renal tumors are rare, and are mainly
detected at autopsy. Klinger (15)
reviewed 5,000 autopsies and identified 118 cases of kidney tumor
metastases, of which, 2 cases (1.69%) were secondary to cervical
cancer. Similar findings were reported in the study by Wagle et
al (16), which identified a rate
of 2.5% for kidney metastases originating from cervical carcinoma
from 4,413 autopsies.
Kidney tumor metastases are rare, and only 9 cases
have been reported to originate from cervical carcinoma to date;
the most recent case dating from 2013 (13). Differences exist among primary renal
cell carcinomas and kidney metastases. Metastatic renal tumors
generally present with diameters of <4 cm, and the majority are
bilateral multiple lumps. Of the 9 cases reported thus far, 4 have
been bilateral kidney tumors, and 5 unilateral. The majority of
these cases (13) occurred within a
15-month period after diagnosis and primary treatment, with the
longest period lasting 118 months (12).
In the present case, the patient experienced
recurrence within 42 months of the initial diagnosis. Initially, a
left renal cyst was suspected, based on the results of the CT
examinations conducted 1 year after the primary treatment. However,
the patient returned to the Hunan Provincial Tumor Hospital 1 year
later, presenting with gross hematuria, FUO and left abdominal
pain. Based on the clinical symptoms and diagnostic imaging at the
time of admission, a metastatic renal tumor was suspected. The
patient was then subjected to nephrectomy, and the subsequent
pathological and immunohistochemical examinations confirmed
squamous cell carcinoma.
Diagnoses of metastatic renal tumors mostly rely on
the findings from radiographic examinations and the clinical
history of the patient (17).
Metastatic renal masses are not always easily characterized by CT,
therefore potentially leading to misdiagnosis. Out of the 9 cases
of metastatic renal tumors originating from cervical carcinoma that
have been reported thus far (5–13), 5 were
initially misdiagnosed as renal abscesses due to the symptoms
displayed by the patients (6,8,10–12), including fever (37.5–41.0°C),
abdominal pain and alterations in the levels of certain biochemical
indicators. Lin et al (12)
highlighted the difficulty in diagnosing renal metastases by
radiographic examination, stating that the patients often
experience FUO, pain and biochemical abnormalities, which may
easily lead to misdiagnosis. Therefore, if a patient with FUO
presents with a history of a primary neoplasm, a secondary renal
tumor should be considered in the differential diagnosis of the
renal mass lesion. For those patients in good condition, a renal
biopsy is required in order to confirm the diagnosis of renal
metastasis. Compared with the 9 previous cases reported in the
literature, the patient in the present study exhibited a single
lesion with a large volume (80×60×80 mm). The abdominal CT
examination conducted on June 2013 identified a low-density nodule
in the left kidney. However, the clinical symptoms were
insignificant at the time, and the nodule was misdiagnosed as a
renal cyst. Notably, the patient experienced recurrence 13 months
later, and exhibited significant clinical symptoms, including pain,
fever and hematuria.
In patients with advanced cervical cancer,
chemoradiotherapy and surgery plus chemotherapy are the main
treatment options (18). However,
patients with metastases derived from cervical carcinoma present
with a poor prognosis despite chemoradiation and surgical
treatment. The overall survival was <12 months for the
previously reported 9 patients who underwent chemoradiotherapy or
surgery for the treatment of renal metastases derived from cervical
carcinoma. Ishihara et al (19) proposed that a kidney resection was
more effective than antitumor therapy for the treatment of renal
metastases originating from cervical carcinoma, since a kidney
resection may reduce the symptoms of pain and improve the quality
of life in these patients. Ogose et al (20) proposed a similar approach for the
treatment of kidney metastases derived from osteosarcoma. However,
surgery was unable to improve the survival rates of these patients.
In the present study, the symptoms of the patient, including
hematuria, fever and abdominal pain, were significantly relieved
following nephrectomy. Furthermore, positive images of multiple
organs without serious complications were observed 4 months after
nephrectomy.
In conclusion, nephrectomy should be the preferred
method for the treatment of kidney metastases derived from cervical
carcinoma if the metastatic lesion is located unilaterally in the
kidney. However, this treatment may only relieve the clinical
symptoms of the patient. Conservative treatments, such as
chemoradiation, may be an option in cases of bilateral metastatic
renal tumors or in those presenting with other widespread lesions.
In the present case study, the patient presented with cervical
carcinoma and metastasis to the left kidney, which was initially
misdiagnosed as a renal cyst. However, the cyst was subsequently
confirmed to be a renal metastasis originating from cervical
carcinoma.
Acknowledgements
The present study was supported by the Fundamental
Research Funds for the Central Universities of Central South
University (grant no. 2177/72150050625).
References
|
1
|
Jin XW, Sikon A and Yen-Lieberman B:
Cervical cancer screening: Less testing, smarter testing. Cleve
Clin J Med. 78:737–747. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Benedetti-Panici P, Maneschi F, D'Andrea
G, Cutillo G, Rabitti C, Congiu M, Coronetta F and Capelli A: Early
cervical carcinoma. Cancer. 88:2267–2274. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Massad LS, Einstein MH, Huh WK, Katki HA,
Kinney WK, Schiffman M, Solomon D, Wentzensen N and Lawson HW: 2012
ASCCP Consensus Guidelines Conference: 2012 updated consensus
guide-lines for the management of abnormal cervical cancer
screening tests and cancer precursors. Obstet Gynecol. 121:829–846.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Roy JB and Walton KN: Secondary tumors of
the kidney. J Urol. 103:411–413. 1970.PubMed/NCBI
|
|
6
|
Reznicek SB and Fallon B: Metastatic
cervical carcinoma masquerading as bilateral renal abscesses.
Urology. 25:174–175. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Nagaoka S, Yamasaki A, Fuziwara E, Hayashi
M, Nakano H and Nihira H: A case of bilateral metastatic renal
tumor originating in a cervical carcinoma. Urol Int. 41:219–221.
1986. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Vilain C, Chaubard T, Gauthier JR, Adoue D
and Le Tallec Y: Febrile secondary cancer of the kidney. Uncommon
manifestation of isolated metastasis of epithelioma of the uterine
cervix without pelvic recurrence. Ann Med Interne (Paris).
139:440–442. 1988.(In French). PubMed/NCBI
|
|
9
|
Koike H, Okamoto T, Tanji S, Fujioka T,
Kubo T and Ohhori T: Two cases of metastatic renal tumor. Acta
Urologica Japonica. 35:475–479. 1989.PubMed/NCBI
|
|
10
|
de La Taille A, Bertrand P, Lemaitre L,
Rigot JM and Mazeman E: Bilateral secondary renal neoplasm
mimicking renal abscesses. Eur Urol. 31:249–250. 1997.PubMed/NCBI
|
|
11
|
Takahashi A, Adachi H, Iwasawa A, Hirose
T, Tsukamoto T, Hata E and Nomura Y: Metastatic cervical carcinoma
mimicking kidney abscess. Int J Urol. 5:377–378. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lin CM, Sun GH, Lee SS, Yu DS, Chang SY
and Wu ST: Remote metastatic cervical carcinoma to kidneys
mimicking bilateral renal abscesses. Eur J Cancer Care (Engl).
16:526–528. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Jeon SW, Kim SH and Kwon SY: Renal
metastasis from primary cervical cancer: A case report. J Korean
Soc Radiol. 68:483–487. 2013. View Article : Google Scholar
|
|
14
|
Oken MM, Creech RH, Tormey DC, Horton J,
Davis TE, McFadden ET and Carbone PP: Toxicity and response
criteria of the Eastern Cooperative Oncology Group. Am J Clin
Oncol. 5:649–655. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Klinger ME: Secondary tumors of the
genito-urinary tract. J Urol. 65:144–153. 1951.PubMed/NCBI
|
|
16
|
Wagle DG, Moore RH and Murphy GP:
Secondary carcinomas of the kidney. J Urol. 114:30–32.
1975.PubMed/NCBI
|
|
17
|
Ferrozzi F, Bova D, De Chiara F, Garlaschi
G and Bassi P: CT of renal metastatic disease. A pictorial essay.
Clin Imaging. 19:60–64. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Benedetti-Panici P, Greggi S, Colombo A,
Amoroso M, Smaniotto D, Giannarelli D, Amunni G, Raspagliesi F,
Zola P, Mangioni C and Landoni F: Neoadjuvant chemotherapy and
radical surgery versus exclusive radiotherapy in locally advanced
squamous cell cervical cancer: Results from the Italian multicenter
randomized study. J Clin Oncol. 20:179–188. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ishihara S, Kobayashi S, Yamaha M,
Takeuchi T, Kuriyama M, Ban Y, Kawada Y, Takahashi Y, Horie M and
Isogai K: Metastatic renal tumor from the lung with regional lymph
node involvement: A case report. Hinyokika Kiyo. 36:51–54.
1990.PubMed/NCBI
|
|
20
|
Ogose A, Morita T, Emura I, Nemoto K and
Hirata Y: Osteosarcoma metastatic to the kidneys without lung
involvement. Jpn J Clin Oncol. 29:395–398. 1999. View Article : Google Scholar : PubMed/NCBI
|