Introduction
Primary angiosarcoma of the spleen is an extremely
rare, highly malignant neoplasm, the pathogenesis of which is
unknown, with early systemic metastatic spread and a dismal
prognosis, regardless of the treatment regimen (1). The disease is one of the least common
types of cancer, with a reported incidence of 0.14–0.25 cases per
million individuals (2,3). The majority of cases have median
survival rates ranging between 4 and 18 months (1,4). Splenic
angiosarcoma was first described by Langhans in 1879 (5) and to date, ~300 cases have been reported
worldwide (6). Early metastasis is
common and the most common sites include the liver, lungs, lymph
nodes and gastrointestinal tract (7).
The clinical presentation of splenic angiosarcoma is usually
unspecific; symptoms of abdominal pain and anaemia are commonly
reported (8). Forming a diagnosis may
be difficult due to the atypical presentation of the tumor. A
diagnosis of splenic angiosarcoma should be considered in patients
with splenomegaly and anemia of unknown etiology (9). Primary splenic angiosarcoma is usually
treated surgically and splenectomy is the mainstay of treatment, as
the lesion is highly refractory to adjuvant treatment with
radiation and chemotherapy (10).
Emergency splenectomy is the standard treatment for cases
exhibiting ruptured splenic angiosarcoma (8). Splenic rupture is a serious complication
of the disease, which is frequently observed in patients, that
results in mortality in a significant proportion of cases (7). The prognosis of primary angiosarcoma of
the spleen remains poor as liver, lung and bone metastases are
common (8). The current study
presents a case of spontaneous splenic rupture in a 77-year-old
female who was treated by laparotomy and splenectomy. Written
informed consent was obtained from the patient's family.
Case report
In June 2014, a 77-year-old female was admitted to
the Department of General Surgery, First Affiliated Hospital of
Wenzhou Medical University (Wenzhou, Zhejiang, China) with diffuse
abdominal pain and distension that had been apparent for 6 days. A
physical examination revealed abdominal distension and a palpable
abdominal mass in the left upper abdominal quadrant. An initial
laboratory test revealed thrombocytopenia (platelet count,
7.0×1010/l) and anemia (hemoglobin level, 7.0 g/dl).
Results of other laboratory examinations were not reported prior to
surgery. Abdominal ultrasonography showed a large amount of
intraperitoneal free fluid and an enlarged spleen filled with
irregular nodules. These findings were confirmed by an abdominal
computed tomography (CT) scan (Fig.
1). CT revealed a large intraperitoneal hematoma in the left
upper quadrant.
Laparotomy revealed a huge, actively bleeding spleen
and an abnormal liver, with several metastatic foci. Blood (2 l)
filled the intraperitoneum. A crack was observed in the spleen,
measuring 4×4 cm in depth, in the upper pole. A splenectomy was
performed. During the surgical procedure, the patient received 2
units of concentrated red blood cells and 2 units of fresh frozen
plasma.
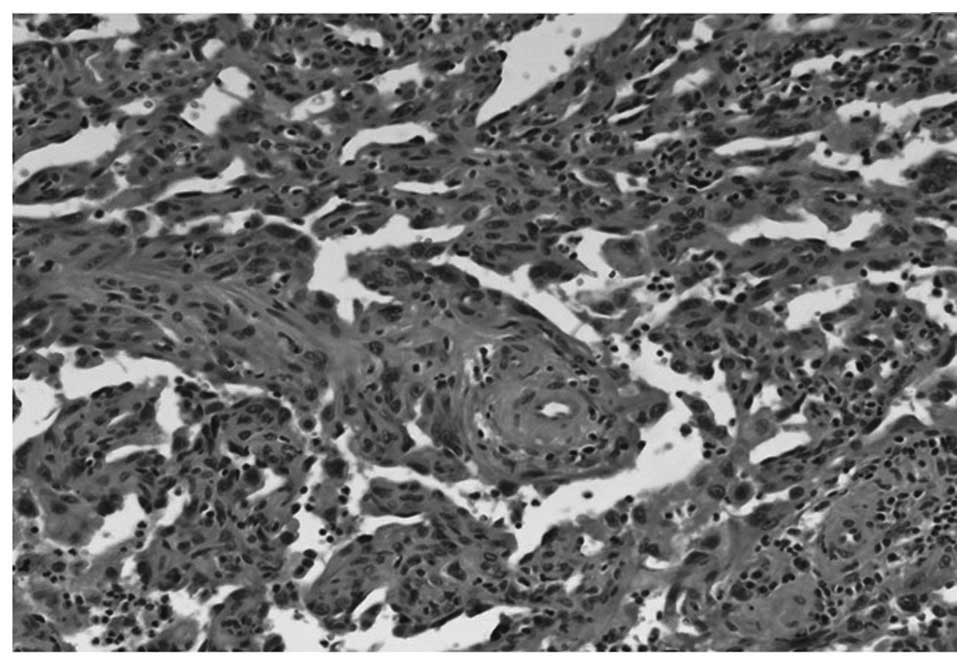
The spleen was 1,550 g in weight and 19×16×11 cm in
size, with a nodular appearance and bleeding. The pathological
examination confirmed that the excised spleen was an angiosarcoma,
presumably of splenic origin (Fig.
2); the spleen was composed of spindle tumor cells and the
ecstatic vascular spaces were lined with hypertrophied endothelial
cells. Immunohistochemical examination demonstrated positive
immunostaining for cluster of differentiation (CD)31 and CD34.
The patient refused any further treatment and two
weeks after surgery, the patient succumbed to the disease due to
hemorrhagic shock and lung metastases.
Discussion
Primary angiosarcoma of the spleen is an uncommon
and aggressive malignant neoplasm that is derived from the splenic
vascular endothelium and elongated endothelial cells of mesenchymal
origin that line the spongy network of sinusoids within the spleen
(9). In general, angiosarcomas are
rapid proliferating, highly infiltrating anaplastic tumors that
tend to recur locally, be widely disseminated, and have an
increased rate of lymph node and systemic metastases (11,12). The
primary histological feature of an angiosarcoma is the formation of
vascular channels with a sarcomatous stroma and papillary
appearance due to endothelial cell proliferation, although another
common finding is an undifferentiated neoplasm (7).
The etiology of primary splenic angiosarcoma remains
unknown. Causes of this disease have been reported as exposure to
ionizing radiation or chemotherapy for lymphoma. Besides that,
exposure to certain chemical agents, such as vinyl chloride,
thorium dioxide and arsenic have been indicated due to their
association with hepatic angiosarcomas (13).
The clinical manifestations of primary splenic
angiosarcoma are rather variable, including abdominal pain,
splenomegaly, anemia, fatigue, generalized weakness, fever, weight
loss and even life-threatening hemorrhage resulting from rupture of
the spleen. Left upper abdominal pain is the most common symptom.
Constitutional symptoms common in malignancy, such as fever,
fatigue and weight loss, have also been observed but are the
initial symptoms <10% of the time. The most common physical
examination is splenomegaly. Splenic rupture is the most serious
manifestation, which often leads to fatal hemorrhage (7).
Laboratory tests can reveal pancytopenia,
leukocytosis, thrombocytosis and an elevated erythrocyte
sedimentation rate prior to diagnosis (7). Anemia is the most common laboratory
abnormality, being found in 75–81% of cases, although 10–40% of
patients exhibit thrombocytopenia; leukocytosis is also often noted
(9). One of the serious complications
that is frequently observed in patients with splenic angiosarcoma
is splenic rupture, leading to a fatal outcome in a significant
percentage of cases (6,7).
Imaging modalities are invaluable for the
differential diagnosis from other benign and malignant splenic
tumors, although diagnostic accuracy is lacking. CT scans may
reveal splenic enlargement with hypo- or hyper-attenuating areas
(7). On contrast-enhanced CT scans,
the tumors may show peripheral or heterogeneous contrast
enhancement similar to that of hepatic cavernous hemangiomas.
However, the clinical features and radiological appearance of the
majority of cases are quite varied and non-specific, and may be
easily associated with other pathological conditions, which makes
early diagnosis and treatment difficult (6).
The usual therapy for ruptured splenic angiosarcoma
is an emergency splenectomy. At present, there is no convincing
evidence to suggest a clinical benefit of chemotherapy in the
treatment of splenic angiosarcoma. When considering early
hematogenous micrometastasis, systemic chemotherapy following
surgery may be theoretically beneficial (6). Although there is no standard treatment
regimen, certain drugs, including cyclophosphamide, doxorubicin,
epirubicin, ifosfamide, daunorubicin, vincristine, actinomycin D,
steroids and Taxol, which have shown efficacy for treating
angiosarcoma in other anatomical sites or other types of
soft-tissue sarcomas, have been empirically proposed to be
effective for primary splenic angiosarcoma (14).
The prognosis of patients with primary splenic
angiosarcoma is quite poor. The majority of patients succumb to
systemic metastases within 1–2 years of diagnosis, even when the
primary tumor has been removed (15).
Long-term survival has only previously been reported in patients
who presented without metastases (6,16).
However, certain studies have considered splenic rupture to be the
worst prognostic factor, as this places patients at a high risk of
peritoneal or vascular dissemination (7). This finding is confirmed by the fact
that early splenectomy prior to rupture of the organ is accompanied
by better survival rates (6).
In conclusion, primary splenic angiosarcoma is an
extremely rare and aggressive soft-tissue sarcoma due to the
presence of early systemic metastases and life-threatening
hemorrhage from the rupture of the spleen. The pathogenesis of the
disease remains unclear, and the clinical and radiological
diagnoses are challenging. The diagnosis of primary splenic
angiosarcoma should be suspected in any patient with splenomegaly
and anemia of unknown etiology. Radiation and chemotherapy have
historically been unsuccessful in improving outcomes in this
patient population. Further evaluation of these options will be
required due to the limited experience to date. The best chance for
survival follows an early diagnosis and a prompt splenectomy prior
to splenic rupture.
References
|
1
|
Duan YF, Jiang Y, Wu CX and Zhu F:
Spontaneous rupture of primary splenic angiosarcoma: A case report
and literature review. World J Surg Oncol. 11:532013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Falk S, Krishnan J and Meis JM: Primary
angiosarcoma of the spleen. A clinicopathologic study of 40 cases.
Am J Surg Pathol. 17:959–970. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Neuhauser TS, Derringer GA, Thompson LD,
Fanburg-Smith JC, Miettinen M, Saaristo A and Abbondanzo SL:
Splenic angiosarcoma: A clinicopathologic and immunophenotypic
study of 28 cases. Mod Pathol. 13:978–987. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Buckner JW III, Porterfield G and Williams
GR: Spontaneous splenic rupture secondary to angiosarcoma. J Okla
State Med Assoc. 83:211–213. 1990.PubMed/NCBI
|
|
5
|
Langhans T: Pulsating cavernous neoplasm
of the spleen with metastatic nodules to the liver. Vichows Arch
Pathol Anat. 75:273–291. 1879. View Article : Google Scholar
|
|
6
|
Liu Z, Du X, Li H, Wang Z, Shen Z, Yao Y
and Zhao H: Primary splenic angiosarcoma. Vasa. 41:57–62. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Manouras A, Giannopoulos P, Toufektzian L,
Markogiannakis H, Lagoudianakis EE, Papadima A, Papanikolaou D,
Filis K and Kekis P: Splenic rupture as the presenting
manifestation of primary splenic angiosarcoma in a teenage woman: A
case report. J Med Case Rep. 2:1332008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Alexandrino H, Julião MJ, Tralhão JG and
Sousa FC: Rupture of splenic angiosarcoma: A rare cause of
spontaneous haemoperitoneum. BMJ Case Rep. 24:20132013.
|
|
9
|
Kamran S, Rodriguez JA and Lairmore TC:
Primary splenic angiosarcoma. JSLS. 14:431–435. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Despoina M, Dionysios D, Georgios A,
Konstantinos S, Efstratios K and Adamantia ZS: Primary angiosarcoma
of the spleen: An oncological enigma. Case Rep Oncol Med.
2014:1930362014.PubMed/NCBI
|
|
11
|
Abbott RM, Levy AD, Aguilera NS, Gorospe L
and Thompson WM: From the archives of the AFIP: Primary vascular
neoplasms of the spleen: Radiologic-pathologic correlation.
Radiographics. 24:1137–1163. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Thompson WM, Levy AD, Aguilera NS, Gorospe
L and Abbott RM: Angiosarcoma of the spleen: Imaging
characteristics in 12 patients. Radiology. 235:106–115. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
den Hoed ID, Granzen B, Granzen B, Aronson
DC, Pauwels P, de Kraker J and van Heurn LW: Metastasized
angiosarcoma of the spleen in a 2-year-old girl. Pediatr Hematol
Oncol. 22:387–390. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ferreira BP, Rodler ET, Loggers ET,
Pollack SM and Jones RL: Systemic therapy in primary angiosarcoma
of the spleen. Rare Tumors. 4:e552012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kren L, Kaur P, Goncharuk VN, Dolezel Z
and Krenova Z: Primary angiosarcoma of the spleen in a child. Med
Pediatr Oncol. 40:411–412. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hsu JT, Ueng SH, Hwang TL, Chen HM, Jan YY
and Chen MF: Primary angiosarcoma of the spleen in a child with
long-term survival. Pediatr Surg Int. 23:807–810. 2007. View Article : Google Scholar : PubMed/NCBI
|