Introduction
Kidney cancer accounts for 2–3% of all malignant
tumors in adults, with renal cell carcinoma (RCC) accounting for
85–90% of kidney cancers (1).
According to the World Health Organization classification criteria
for renal cancer, published in 2004 (2), RCC with Xp11.2 translocation/TFE3 gene
fusion is classified as a distinct type of RCC. RCC with Xp11.2
translocation/TFE3 gene fusion primarily occurs in adolescents, and
demonstrates no significant gender variation (2). The malignancy of RCC with Xp11.2
translocation/TFE3 gene fusion is considered to be relatively low.
Therefore, few cases of advanced tumors have been previously
reported (2).
RCC is capable of invading the renal vein and
inferior vena cava to form a tumor thrombus; in China, this occurs
in 7–10% of RCC cases (3). It is
widely accepted that tumor thrombus of the inferior vena cava is
not a decisive indicator for determination of the prognosis of
patients with RCC (4).
Surgery is typically the first choice of treatment
for RCC, due to its insensitivity to chemotherapy and radiotherapy.
Clinical studies have demonstrated a certain efficacy of
multi-kinase inhibitors, such as sunitinib, sorafenib and mTOR/MET
kinase inhibitor, in treating rapidly progressive metastatic Xp11.2
RCC in adult patients (5,6). However, the optimal treatment approach
for Xp11.2 RCC remains to be determined.
The current study presents the case of a patient
with Xp11.2 translocation/TFE3 gene fusion RCC, who underwent
radical resection of a renal tumor and removal of the tumor
thrombus, assisted by cardiopulmonary bypass.
Case report
The current report presents the case of a
46-year-old male, who was admitted to the Nanjing Drum Tower
Hospital (Nanjing, China) in September 2013, due to right abdominal
pain. Renal magnetic resonance imaging (MRI) results suggested a
diagnosis of RCC with hemorrhage, accompanied by an inferior vena
cava tumor thrombus and enlarged retroperitoneal lymph nodes.
Vascular ultrasound examination indicated that a tumor thrombus had
formed within the inferior vena cava, and that it extended to the
level of the diaphragm. Following the exclusion of surgical
contraindications, radical resection of the right kidney, and
removal of the tumor thrombus within the inferior vena cava under
cardiopulmonary bypass, were performed. Briefly, following exposure
of the right kidney and inferior vena cava, cardiopulmonary bypass
was established via intubation of the ascending aorta, inferior
vena cava and right atrium. The tumor thrombus was removed by
dissecting the vena cava following relocation of the tumor thrombus
from the superior vena cava to the inferior vena cava. Heparin (400
U/kg) and low-dose protamine (2 mg/kg; for the reversal of heparin)
were administered during and following the cardiopulmonary bypass.
Subsequently, the right kidney was resected.
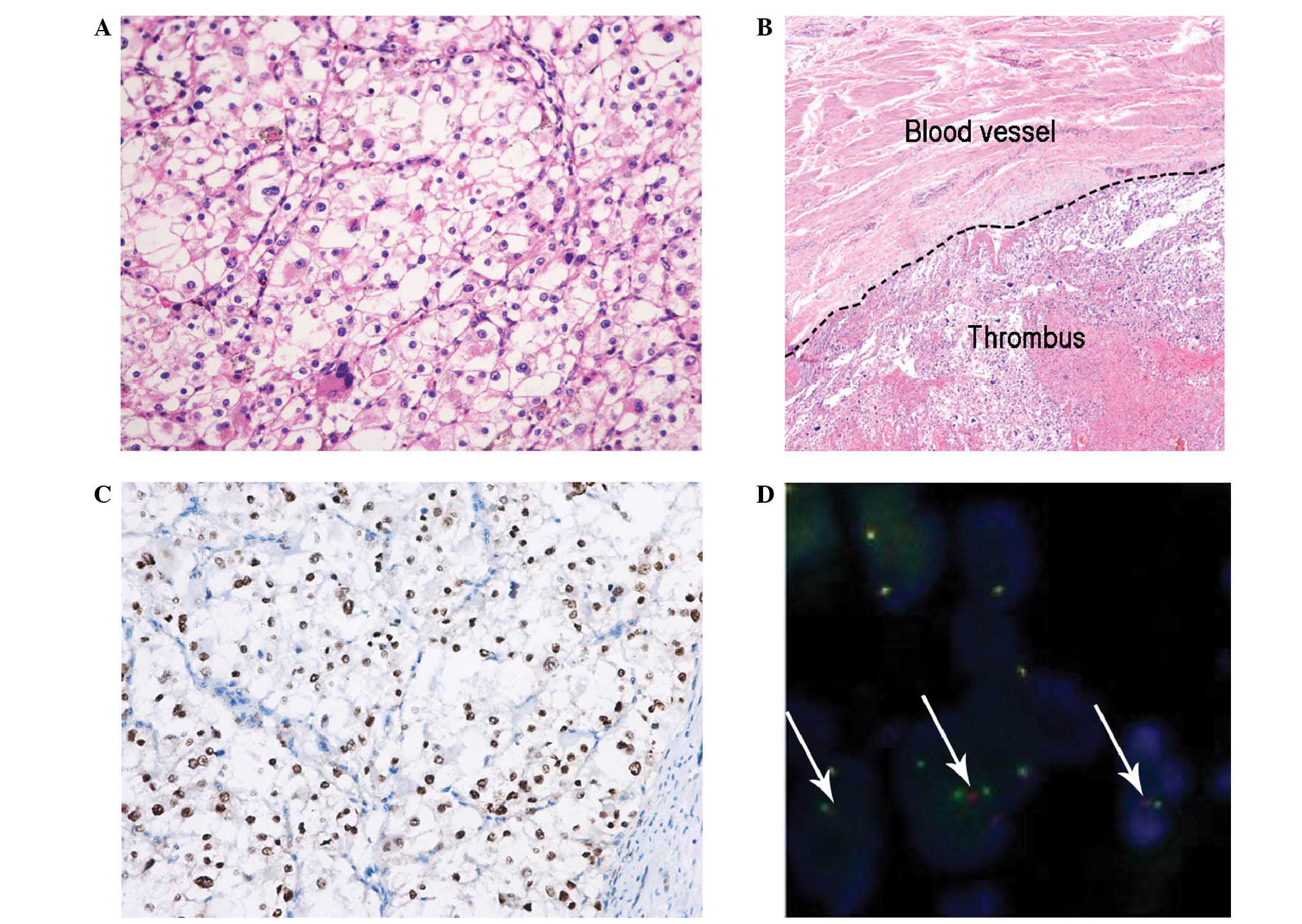
Combined with the results of TFE3 gene fusion
protein immunohistochemistry and fluorescent in situ
hybridization (FISH), a diagnosis of Xp11.2 translocation/TFE3 gene
fusion-related RCC was considered (Fig.
1A–D). The patient was discharged two weeks subsequent to
surgery. Chemotherapy was administered following discharge of the
patient from hospital; the patient was initially started on oral
sorafenib (400 mg, twice daily), and 6 months later was switched to
oral sunitinib (50 mg/day) for 4 weeks on and 2 weeks off.
The patient was followed up for 12 months subsequent
to treatment. The patient's renal function remained within the
normal range, while computed tomography examination revealed no
evidence of disease recurrence or metastases. Therefore, the
possibility of recurrence during this follow-up period was ruled
out. However, determining the long-term prognosis of patient still
requires long-term follow-up.
Discussion
According to the tumor thrombus classification
devised by Neves and Zincke (7),
based on the extent of dissection, the tumor thrombus in the
present case was defined within the third classification, and
described as a tumor thrombus within the inferior vena cava,
extending to the level below the diaphragm. MRI, which demonstrates
advantages for the detection of vena cava tumor thrombi, was
utilized in the present case to detect and evaluate the vena cava
tumor thrombus (8). Following
exclusion of the presence of distant metastasis, surgery was
performed.
It has been accepted that surgical removal of the
tumor and thrombus is the typical first choice treatment strategy
for non-metastatic RCC, even with the co-occurrence of an inferior
vena cava thrombus (9). In the
present case, cardiopulmonary bypass was utilized to assist with
the removal of the tumor thrombus within the inferior vena cava
(Fig. 1B). Cardiopulmonary bypass may
be able to extend operating times and surgical space for surgeons
(10). In addition, cardiopulmonary
bypass markedly reduces the potential risk of bleeding during
surgery on large blood vessels, simplifying the surgical resection
of tumor thrombi within the inferior vena cava, and those located
within the right atrium (9). It is
widely accepted that immunohistochemical staining of certain
proteins specifically expressed in Xp11.2 translocation/TFE3 gene
fusion RCC, including TFE3 gene fusion-associated protein, is the
primary method for diagnosis of this type of tumor (11,12).
Argani et al (13) reported
that the sensitivity and specificity of immunohistochemistry in the
diagnosis of tumors with Xp11.2 translocation/TFE3 gene fusion in
the urinary system, and additional systems, was 99.6 and 97.5%,
respectively. In the present case, the tumor weakly expressed
P504S, while strongly expressing CD117, human melanoma black 45 and
TFE3 (Fig. 1C).
To date, eight specific genotypes have been reported
in Xp11.2 translocation/TFE3 gene fusion RCC, and in three of these
the site of gene fusion cannot be clearly identified. Xp11.2
translocation/TFE3 gene fusion RCC accounts for ~1% of RCC
diagnoses in adult patients (14).
FISH with polyclonal break-apart probes, has been used as a rapid
and accurate diagnostic method for detecting TFE3 gene fracture in
tumor tissue. This is due to this method's specific ability to bind
with each end of fragments of TFE3 DNA (15,16). In
the present case, FISH was used to confirm the diagnosis of Xp11.2
translocation/TFE3 gene fusion RCC. As indicated in Fig. 1D, tumor cells demonstrated a fusion
signal (yellow) and a pair of red and green split signals,
representing TFE3 gene translocations in the X chromosome. This
result confirmed that FISH may be useful as an alternative,
effective method for the diagnosis of Xp11.2 translocation/TFE3
gene fusion RCC.
Follow-up of the current patient is ongoing. To the
best of our knowledge, the present case is the first to report the
successful surgical treatment of Xp11.2 translocation/TFE3 gene
fusion RCC with inferior vena cava tumor thrombus surgery, using
cardiopulmonary bypass. The present report may provide a reference
for the development of guidelines for the diagnosis and treatment
of Xp11.2 translocation/TFE3 gene fusion RCC.
References
|
1
|
Kabala JE: The kidneys and ureters.
Textbook of Radiology and Imaging. Sutton D: (London). Churchill
Livingstone. 9532003.
|
|
2
|
Lopez-Beltran A, Scarpelli M, Montironi R
and Kirkali Z: 2004 WHO classification of the renal tumors of the
adults. Eur Urol. 49:798–805. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Li XF, Zhou FJ, Qiu SP, et al: Diagnosis
and treatment of renal cell carcinoma with vena cava tumor thrombi.
Ai Zheng. 23:1074–1067. 2004.(In Chinese). PubMed/NCBI
|
|
4
|
Cost NG, Delacroix SE Jr, Sleeper JP,
Smith PJ, Youssef RF, Chapin BF, Karam JA, Culp S, Abel EJ,
Brugarolas J, et al: The impact of targeted molecular therapies on
the level of renal cell carcinoma vena caval tumor thrombus. Eur
Urol. 59:912–918. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Choueiri TK, Mosquera JM and Hirsch MS: A
case of adult metastatic Xp11 translocation renal cell carcinoma
treated successfully with sunitinib. Clin Genitourin Cancer.
7:E93–94. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Malouf GG, Camparo P, Oudard S, et al:
Targeted agents in metastatic Xp11 translocation/TFE3 gene fusion
renal cell carcinoma (RCC): A report from the Juvenile RCC Network.
Ann Oncol. 21:1834–1838. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Neves RJ and Zincke H: Surgical treatment
of renal cancer with vena cava extension. Br J Urol. 59:390–395.
1987. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Guo HF, Song Y and Na YQ: Value of
abdominal ultrasound scan, CT and MRI for diagnosing inferior vena
cava tumour thrombus in renal cell carcinoma. Chin Med J (Engl).
122:2299–2302. 2009.PubMed/NCBI
|
|
9
|
Chiappini B, Savini C, Marinelli G, Suarez
SM, Di Eusanio M, Fiorani V and Pierangeli A: Cavoatrial tumor
thrombus: Single-stage surgical approach with profound hypothermia
and circulatory arrest, including a review of the literature. J
Thorac Cardiovasc Surg. 124:684–688. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Paul JG, Rhodes MB and Skow JR: Renal cell
carcinoma presenting as right atrial tumor with successful removal
using cardiopulmonary bypass. Ann Surg. 181:471–473. 1975.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Argani P, Hicks J, De Marzo AM, Albadine
R, Illei PB, Ladanyi M, Reuter VE and Netto GJ: Xp11 translocation
renal cell carcinoma (RCC): Extended immunohistochemical profile
emphasizing novel RCC markers. Am J Surg Pathol. 34:1295–1303.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Argani P and Ladanyi M: The evolving story
of renal translocation carcinomas. Am J Clin Pathol. 126:332–334.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Argani P, Lal P, Hutchinson B, Lui LY,
Reuter VE and Ladanyi M: Aberrant nuclear immunoreactivity for TFE3
in neoplasms with TFE3 gene fusions: A sensitive and specific
immunohistochemical assay. Am J Surg Pathol. 27:750–761. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Liu Y, Xu B and Chen F: Recent advances in
renal cell carcinoma associated with Xp11.2 translocations/TFE gene
fusions. N Am J Med Sci. 5:43–47. 2012. View Article : Google Scholar
|
|
15
|
Klatte T, Streubel B, Wrba F, Remzi M,
Krammer B, de Martino M, Waldert M, Marberger M, Susani M and
Haitel A: Renal cell carcinoma associated with transcription factor
E3 expression and Xp11.2 translocation: Incidence, characteristics,
and prognosis. Am J Clin Pathol. 137:761–768. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kuroda N, Katto K, Tanaka Y, Yamaguchi T,
Inoue K, Ohara M, Mizuno K, Hes O, Michal M and Lee GH: Diagnostic
pitfall on the histological spectrum of adult-onset renal carcinoma
associated with Xp11.2 translocations/TFE3 gene fusions. Med Mol
Morphol. 43:86–90. 2010. View Article : Google Scholar : PubMed/NCBI
|