Introduction
Synovial sarcoma (SS) originates primarily in the
soft tissues, generally in the para-articular regions of the
extremities. These tumors can, however, involve other unusual
locations (1), such as the pleura,
lungs, mediastinum and kidneys. Primary renal SS is a rare
carcinoma that was first described by Argani et al in 1999
(2). This tumor presents a diagnostic
dilemma, as it is extremely difficult to distinguish from other
renal carcinomas, including metastatic sarcoma and renal cell
carcinoma with sarcomatoid differentiation, which may have similar
histological characteristics (3).
Iacovelli et al (4) examined
64 cases of SS and the median overall survival time was 48 months;
in addition, at the time of diagnosis, 98% of patients had clinical
symptoms, 67% had pain, and 38% had hematuria. The primary therapy
for renal synovial sarcoma is radical surgical resection. However,
no consensus has been reached on the adjuvant treatment since at
present only case reports have been published. The current study
reports a case of primary SS (PSS) of the kidney and presents a
review of the relevant literature.
Case report
A 54-year-old female presented with interrupted
right flank pain that had been apparent for 20 years, precipitating
with hematuria for 8 days. Abdominal computed tomography revealed a
heterogeneous, soft-tissue mass with unclear margins, arising in
the upper pole of the right kidney. The mass exhibited solid,
necrotic components and heterogeneous enhancement. No evidence of
renal vein, inferior vena or right atrial thrombosis was found. No
local invasion or lymphadenopathy was identified (Fig. 1). The clinical and radiological
diagnosis was consistent with renal cell carcinoma.
A right nephrectomy was subsequently performed. The
resected specimen weighed 210 g and measured 13×5×3.5 cm.
Macroscopic examination of the specimen revealed a cystic 8×8×7-cm
tumor with soft, solid growth, which was yellow-brown tan in color,
in the upper pole the kidney. Hemorrhage and necrosis were also
observed (Fig. 2).
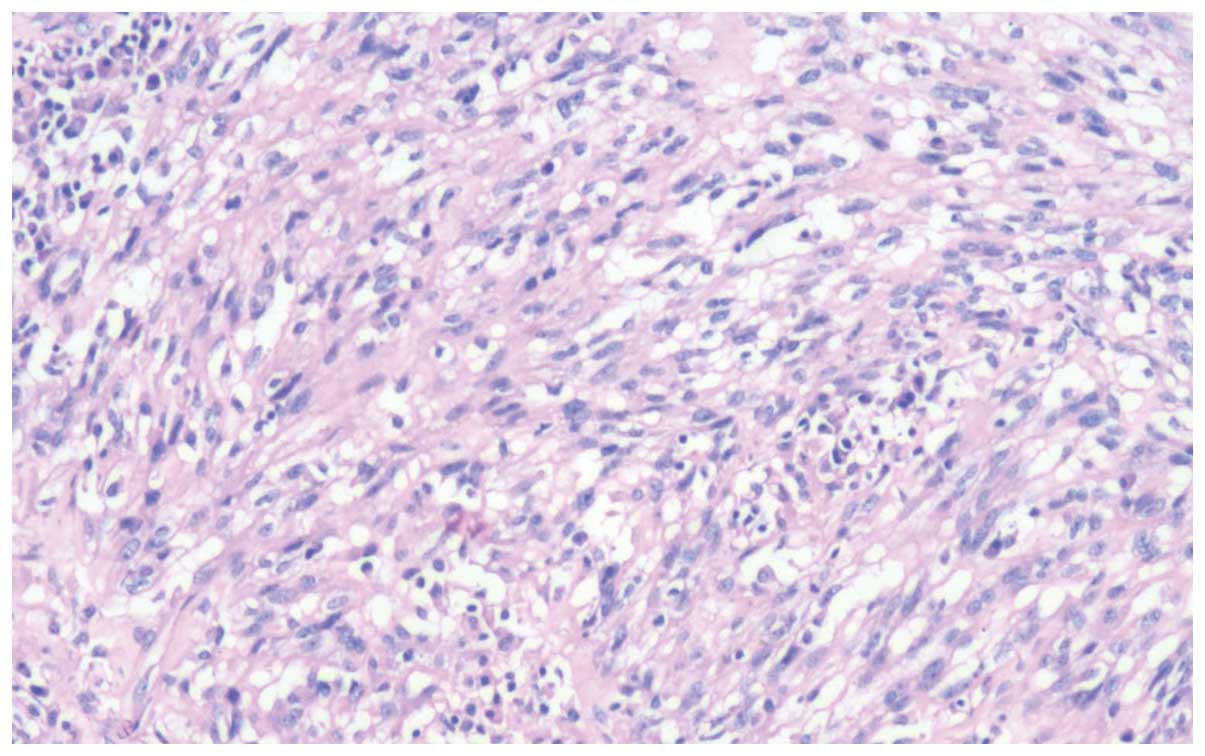
Microscopically, the tumor was composed of spindle
cells arranged in intersecting fascicles, alternating with
hypocellular areas (Fig. 3).
Immunohistochemical study showed positive staining for epithelial
membrane antigen (EMA; Fig. 4A),
cytokeratin (CK; Fig. 4B), B-cell
lymphoma 2 (Bcl-2; Fig. 4C), vimentin
(Vim) and cluster of differentiation (CD)99, and no staining for
S100, CD34, CD117, synaptophysin, mesothelial cells and calretinin,
which are both mesothelial tissue markers. Molecular analysis
demonstrated a translocation between the SYT gene on chromosome 18
and the X chromosome, which confirmed the diagnosis of SS. Reverse
transcription-polymerase chain reaction analysis also detected mRNA
expression of the SYT-SXX1 gene. According to the findings, a
diagnosis of monophasic spindle cell SS was formed. The patient is
currently free of local recurrence or metastasis at 12 months
post-surgery.
Discussion
PSS of the kidney is extremely rare and was first
described by Faria et al in 1999 (2). To the best of our knowledge, <50
cases have been reported in the English literature. There is
currently no standard treatment owing to the limited number of
reported cases. Among sarcomas of the kidney, leiomyosarcoma is the
most frequent type, comprising 40–60%, followed by
rhabdomyosarcoma, chondrosarcoma, liposarcoma, angiosarcoma,
hemangiopericytoma and osteosarcoma (3).
Generally, SS affects adolescents and young adults
between 20 to 50 years old (5). The
mean age at diagnosis is 37 years (range, 13–67 years), ~1% of
cases are located in the kidney. The mean tumor diameter is 11 cm
(range, 3–21 cm), and the rate of metastasis upon admission is
likely to be low (5).
There are no clinical or imaging features that can
indicate a diagnosis of renal SS. Thus, it is a challenge to
diagnose the tumor due to its rarity and its similar presentation
to other renal carcinomas (6,7). Furthermore, renal SS is usually confused
with other soft-tissue sarcomas under the microscope. The majority
of the tumors in the literature were initially interpreted as renal
cell carcinoma. The differential diagnosis includes adult Wilms'
tumors, transitional cell carcinoma, renal cell carcinoma,
hemangiopericytoma and primitive neuroectodermal tumors (8).
Poorly-differentiated SS is formed from sheets of
undifferentiated round cells with hyperchromatic nuclei and
frequent mitoses, and is associated with the poorest outcome
(9). A diagnosis of biphasic SS may
be formed by the presence of both epithelial and spindle cell
components, while monophasic SS is diagnosed with an epithelial or
a spindle cell component only. However, the differentiation of
monophasic SS from other spindle cell sarcomas may be difficult
(5). Immunohistochemical studies can
confirm the pathological diagnosis. SS usually stains positively
for Bcl-2, CD99/Mic2, CD56, Vim and focally for EMA, but negatively
for desmin, actin, WT-1, S-100, CD34 and CD31 (5,9). The
immunohistochemical results found in the present case were
completely positive for Bcl-2, EMA and vimentin, focally positive
for CD99, and completely negative for S-100, CD34 and CD117.
Currently, the gold standard for the diagnosis of
synovial sarcoma is the fusion of the synovial sarcoma
translocation, chromosome 18 gene (SYT; also known as SS18) on
chromosome 18 to either the synovial sarcoma, X breakpoint 1 (SSX1)
or SSX2 genes on chromosome Xp11 to form a SYT-SSX fusion (8,10).
Although no guidelines have been established with
regard to the treatment of primary renal SS due to the limited
number of cases reported, surgery is considered the first choice.
However, the prognosis is poor with the use of surgical treatment
only. Based on observations that the tumor is more sensitive to
chemotherapy than other soft-tissue sarcomas (11), chemotherapy is used in the clinic. The
clinical benefit of adjuvant chemotherapy for sarcoma remains
controversial, as there is no conclusive evidence that it confers
any survival benefits. This may be due to the different
histological subtypes that are reported in studies, as well as the
evolution in the quality of treatment and the range of criteria
that are used for the selection of patients for adjuvant systemic
therapy (12). Due to the rarity of
the tumor and the lack of any established benefits of adjuvant
therapy in the literature, the present case used follow-up
examinations only, with no adjuvant therapy. The patient is
currently free of local recurrence or metastasis at 12 months
post-surgery.
In conclusion, primary renal SS is an extremely rare
neoplasm, with histomorphological and immunohistochemical features
that may be confused with other spindle cell tumors of the kidney.
The differential diagnosis of such a tumor is therefore difficult,
and molecular or cytogenetic analysis should be used to confirm the
pathological diagnosis. Although the clinical benefit of adjuvant
chemotherapy remains uncertain, a multidisciplinary approach to
treat the disease may bring some benefits to the patient, such as
pain relief.
References
|
1
|
Divetia M, Karpate A, Basak R and Desai
SB: Synovial sarcoma of the kidney. Ann Diagn Pathol. 12:333–339.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Argani P, Faria PA, Epstein JI, et al:
Primary renal synovial sarcoma: Molecular and morphologic
delineation of an entity previously included among embryonal
sarcomas of the kidney. Am J Surg Pathol. 24:1087–1096. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Zakhary MM, Elsayes KM, Platt JF and
Francis IR: Magnetic resonance imaging features of renal synovial
sarcoma: A case report. Cancer Imaging. 8:45–47. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Iacovelli R, Altavilla A, Ciardi A, et al:
Clinical and pathological features of primary renal synovial
sarcoma: analysis of 64 cases from 11 years of medical literature.
BJU Int. 110:1449–1154. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ozkan EE, Mertsoylu H and Ozardali HI: A
case of renal synovial sarcoma treated with adjuvant ifosfamide and
doxorubicin. Intern Med. 50:1575–1580. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Dassi V, Das K, Singh BP and Swain SK:
Primary synovial sarcoma of kidney: A rare tumor with an atypical
presentation. Indian J Urol. 25:269–271. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Schaal CH, Navarro FC and Moraes Neto FA:
Primary renal sarcoma with morphologic and immunohistochemical
aspects compatible with synovial sarcoma. Int Braz J Urol.
30:210–213. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Koyama S, Morimitsu Y, Morokuma F and
Hashimoto H: Primary synovial sarcoma of the kidney: Report of a
case confirmed by molecular detection of the SYT-SSX2 fusion
transcripts. Pathol Int. 51:385–391. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Nishida T, Inamoto T, Uehara H, et al:
Monophasic primary renal synovial sarcoma accompanied with a
hemorrhagic cyst. Urol J. 8:244–247. 2011.PubMed/NCBI
|
|
10
|
Gabilondo F, Rodríguez F, Mohar A, et al:
Primary synovial sarcoma of the kidney: Corroboration with in situ
polymerase chain reaction. Ann Diagn Pathol. 12:134–137. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Karavasilis V, Seddon BM, Ashley S, et al:
Significant clinical benefit of first-line palliative chemotherapy
in advanced soft-tissue sarcoma: retrospective analysis and
identification of prognostic factors in 488 patients. Cancer.
112:1585–1591. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Blay JY and Le Cesne A: Adjuvant
chemotherapy in localized soft tissue sarcomas: Still not proven.
Oncologist. 14:1013–1020. 2009. View Article : Google Scholar : PubMed/NCBI
|