Introduction
Synovial chondromatosis (SC) has a benign clinical
course characterized by cartilaginous metaplasia within the
synovial membrane, resulting in the formation of multiple
cartilaginous nodules within the synovium (1,2). These
nodules can then ossify or calcify leading to extrusion from the
synovium leaving osteochondral loose bodies within the joint space
or extra-articular soft tissues, but bony erosion is rare (3). SC usually has intra-articular
involvement of the joints, including the hip, knee, ankle, elbow,
wrist and shoulder joints (4).
Extra-articular involvement is rare and mainly observed in a
synovial sheath or bursa of the hand and foot (5). The current study presents a case of
synovial osteochondromatosis of the left proximal thigh muscle gap
in a 46-year-old female. This study was approved by the Ethical
Review Committee of The First Affiliated Hospital of Nanchang
University Medical School (Nanchang, Jiangxi, China), and informed
consent was obtained from the patient.
Case report
A 46-year-old female presented to the Department of
Orthopedics, The First Affiliated Hospital of Nanchang University
(Nanchang, China) on June 24, 2014, with the chief complaint of
painful swelling of the left proximal thigh. The swelling had first
appeared 3 years previously and had become aggravated during the
last 6 months. The patient had no history of injury, past medical
illnesses or family history that were associated. In the general
physical examination, limited motion in the left hip was observed,
with paresthesia in the left lower extremity.
In a further examination, a well-defined, lobular,
tender and firm soft-tissue mass was found over the left proximal
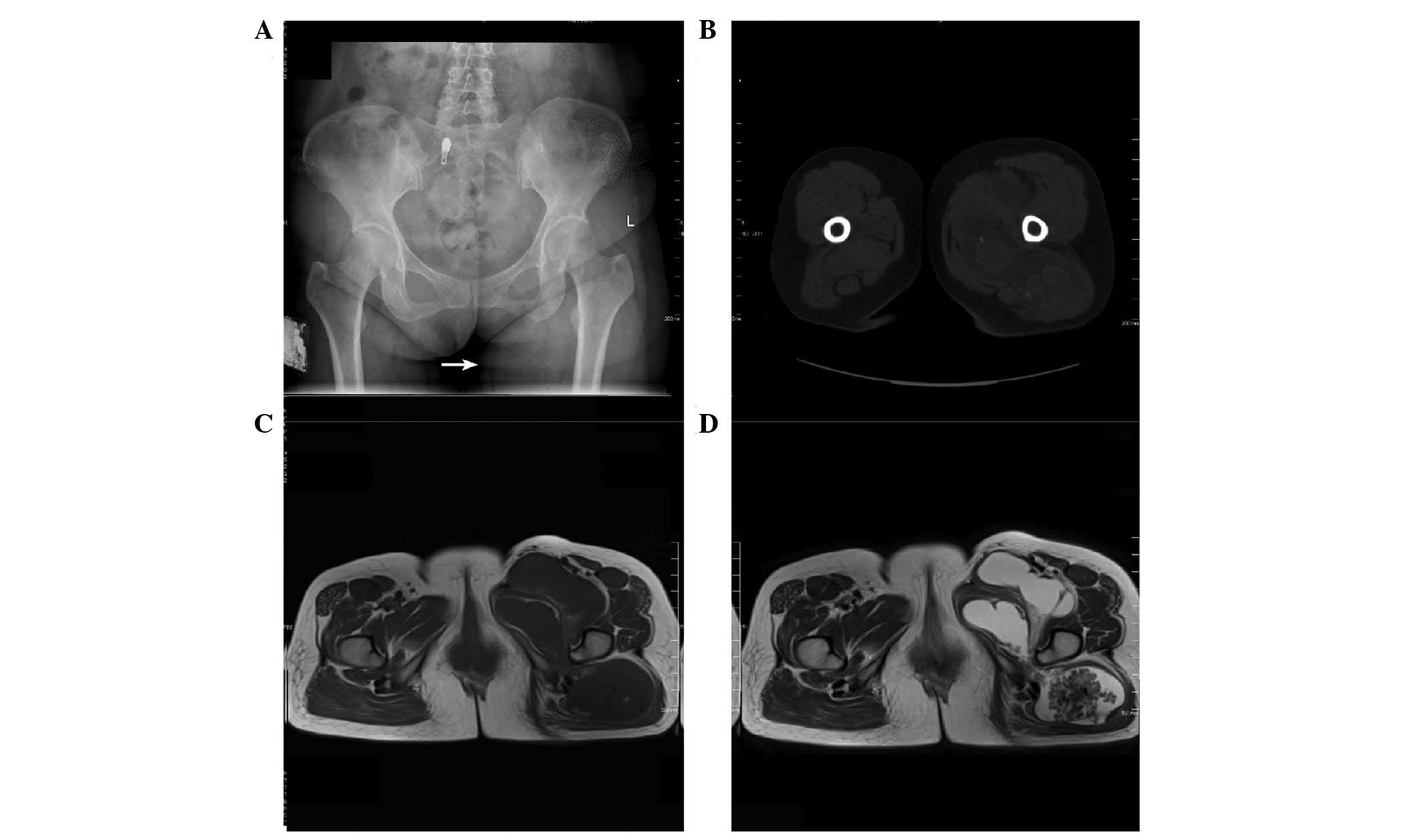
inner thigh, and the test for hip instability was negative. Plain
radiographs indicated a huge mass shadow medial to the left
proximal thigh, which contained multiple radiopaque calcified
bodies. No visible destruction of the surrounding bone was shown
(Fig. 1A). Computed tomography (CT)
revealed an irregular mixed density mass shadow containing a
certain degree of punctate calcification in the gap between the
anterior and posterior muscles of the left proximal inner thigh
(Fig. 1B). However, the articular
surface of the hip joint was intact and these small calcified
bodies did not migrate into the hip joint cavity. Enhanced CT
showed slight peripheral enhancement of the mass. In addition, no
distant metastases were observed. Furthermore, magnetic resonance
imaging (MRI) was performed to evaluate the giant mass. Axial
T1-weighted images showed a low-signal intensity and axial
T2-weighted images showed a high-signal intensity containing
certain areas of punctate low-signal intensity (Fig. 1C and D). T2-weighted imaging with fat
suppression also showed high-signal intensity. Based on this
information, SC was considered with regard to the diagnosis of the
patient.
Based on the exclusion of surgical
contraindications, orthopedic tumor surgeons performed surgery to
resect the tumor. The patient was placed in a floating supine
position with disinfected and paved sterile drapes arranged
routinely around the left proximal thigh to expose the surgical
field following successful epidural anesthesia. First, surgery via
a medial approach to the hip joint was performed, with a ~15-cm
long incision. Furthermore, the subcutaneous tissue, superficial
fascia, deep fascia and adductor group of muscles were separated
layer by layer until the femoral artery, femoral vein and femoral
nerve were observed. The nerve and vessel above were compressed
slightly by the huge tumor, but appeared to be intact. The tumor
was milk white, located from the front to the back of the left
proximal inner thigh, and included several cauliflower-like, firm,
cartilaginous nodules. The anterior region of the tumor was excised
completely. In order to excise the posterior region of the tumor, a
posterior approach to the hip joint was applied. The tumor was
observed near the ischiadic nerve, which was intact. Through
separation of the subcutaneous issue, superficial fascia and
gluteal fascia, the tumor was more specifically located in the gap
between the gluteus maximus and medius. The posterior region of the
tumor was excised completely. Intraoperative tissues were extracted
to perform a pathological examination. A wound drainage tube was
placed and each layer of tissue was sutured strictly after complete
hemostasis. In addition, the estimated blood loss volume was 300 ml
and there was no blood transfusion in the whole treatment
process.
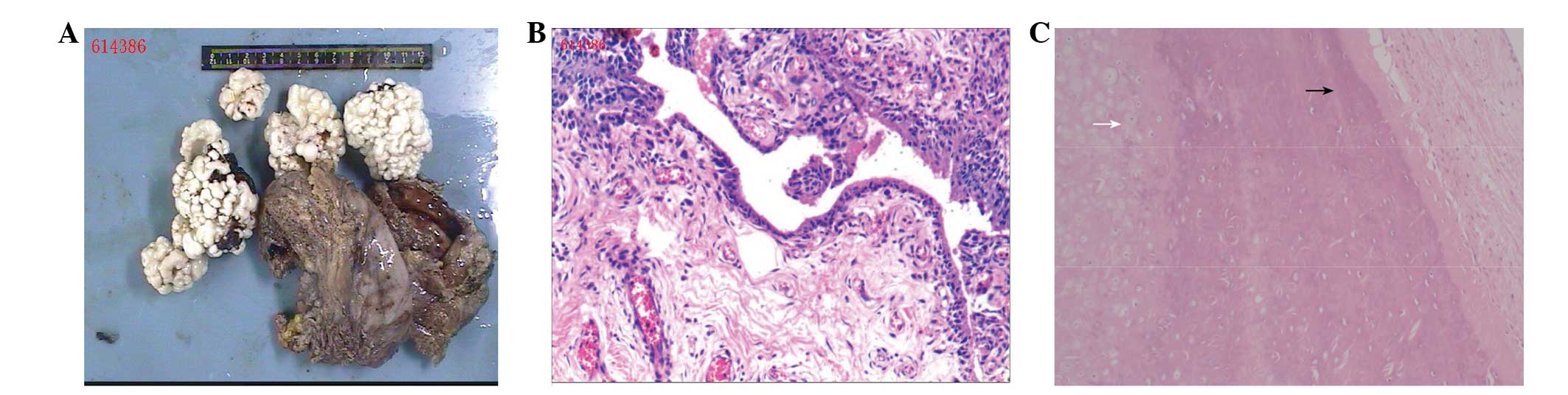
The gross pathological examination revealed large,
smooth-surfaced, dark-brown membrane-like manifestations and
several loose bodies. The irregular tissue was ~15×14×5
cm3 in size (Fig. 2A).
Upon hematoxylin and eosin staining, the membrane-like
manifestations were revealed to be mature synovial tissue (Fig. 2B). The histopathological findings of
loose bodies ultimately revealed mature cartilaginous tissue with
calcification. The chondrocyte nuclei were normal without atypical
changes. There were no definite binucleate cells and no mitotic
chondrocytes observed. No necrosis or bone destruction was found
(Fig. 2C). The diagnosis of primary
SC was confirmed on the basis of these findings. There was no
evidence of chondrosarcomatous transformation.
The patient was discharged without any complications
1 week after the total excision surgery. At the time of the 3-month
follow up, the patient was completely free from pain during daily
activities and a normal range of motion was present in the left hip
joint. No evidence of recurrence was noted during the 3 months
after surgery.
Discussion
SC is a benign condition that usually occurs among
individuals >40 years old, with a predilection for males. Among
the population of SC patients, the ratio of males to females is 2:1
(6,7).
SC is characterized by metaplasia and formation of multiple
cartilaginous nodules in the synovial membrane of the joints,
tendons and bursae (1,2,7).
Typically, it usually involves the large joints. The knees are most
commonly involved and account for 60–70% of cases, with the elbows,
hips and shoulders as the other common sites (5,8). Although
the etiology is thus far unknown, certain data has suggested a
neoplastic origin with chromosome 6 abnormalities (9). There is an extraordinarily low risk of
malignancy with SC, however, a case study has confirmed the
coexistence of chondrosarcoma with SC (10).
SC can be classified into primary and secondary
forms. Primary SC is associated with the benign reactive metaplasia
of the synovial membrane (11,12).
Milgram divided this into three phases. Phase one encompasses
active synovial disease without joint loose bodies. Phase two
involves a transitional phase with osteochondral nodules in the
synovial membrane and free floating in the joint space. Phase three
reveals several free osteochondral bodies with intrasynovial
disease (13). Secondary SC is
associated with the setting of pre-existing joint pathology, such
as trauma, osteonecrosis, tuberculosis, rheumatoid arthritis,
synovitis, osteoarthritis, osteochondritis dissecans and
neuropathic arthropathy (11,12). The two forms of SC have typical
histopathological differences. In primary lesions, cartilage
nodules and loose bodies manifest as irregular nests, usually with
binucleated cells formed by sporadic diffuse calcification and
metaplastic cartilage. By contrast, in secondary lesions,
calcifications are band-like with uniform, evenly distributed
chondrocytes; furthermore, fragments of subchondral bone or
articular cartilage may be present at the center of loose bodies
(14,15).
The disease process includes the synovium of a
joint, bursa or tendon sheath undergoing metaplasia, nodular
proliferation, hyperplasia, hyaline or myxoid changes and
fragmentation. These fragments may break off from the synovial
surface into the joint, and will continually grow, calcify or
ossify when loose bodies have formed, subsequently starting to lock
or irritate the joint. Other fragments may embed within the
proliferating synovium or extend into the surrounding soft tissues
(7,13). Multiple intra-articular loose bodies
can result in degenerative osteoarthritis of the joint; this may
cause the mechanical destruction of the articular cartilage
(7). Clinically, these patients
present with progressively painful, swollen and growing palpable
masses on affected joints. Limitations in movement and locking of
the joints can also be caused (16).
Although the large soft-tissue mass was located in the muscle gap
in the present study, the patient presented with limited movement
of the left hip, swelling and progressively worsening pain around
the left proximal thigh. This may have been a result of extrusion
of the periphery of normal tissue.
Extra-articular synovial osteochondroma is difficult
to detect during the early stages (17). The radiological appearance is
dependent on the disease stage and the extent of cartilaginous
nodule calcification.
If the extra-articular fragments are adequately
calcified, a diagnosis is easily made according to plain
radiographic examination and CT scan, as shown in the present
patient (Fig. 1). With non-calcified
fragments, MRI scans are required. MRI is useful in the early phase
of SC, as radiography is only able to reveal a soft-tissue density
mass prior to the occurrence of calcification or ossification
(5). In the present patient, MRI was
performed to evaluate the status of the ligaments and adjacent
articular cartilage around the left hip joint.
Surgical excision has been considered as the
preferential treatment to relieve pain, limit osteoarthritis
development and histologically confirm the diagnosis (18). The treatment of choice involves the
excision of loose bodies and an extensive synovectomy regardless of
whether the synovial osteochondroma is intra- or extra-articular
(19,20). In the present case, mass excision with
extensive synovectomy was performed due to the large size of the
mass and the irritation to the hip joint.
Following surgical treatment, the patient was
symptom-free at the 3-month follow-up. Although the condition is
benign and recurrence is not usually observed, we suggest that the
follow-up of such patients should be performed for observation of
any malignant changes.
References
|
1
|
Nakashima H, Sugiura H, Nishida Y, Yamada
Y and Ishiguro N: Synovial osteochondromatosis of the
carpometacarpal joint. Am J Orthop (Belle Mead NJ). 36:E151–E152.
2007.PubMed/NCBI
|
|
2
|
Burrafato V, Campanacci DA, Franchi A and
Capanna R: Synovial chondromatosis in a lumbar apophyseal joint.
Skeletal Radiol. 27:385–387. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Birchall D, Khangure MS and Spagnolo DV:
Vertebral synovial osteochondromatosis with compressive myelopathy.
Spine (Phila Pa 1976). 24:921–923. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lohmann CH, Köster G, Klinger HM and Kunze
E: Giant synovial osteochondromatosis of the acromio-clavicular
joint in a child. A case report and review of the literature. J
Pediatr Orthop B. 14:126–128. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Doral MN, Uzumcugil A, Bozkurt M, Atay OA,
Cil A, Leblebicioglu G and Tetik O: Arthroscopic treatment of
synovial chondromatosis of the ankle. J Foot Ankle Surg.
46:192–195. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Maier D, Izadpanah K, Jaeger M, Ogon P and
Südkamp NP: Biceps tenoscopy in arthroscopic treatment of primary
synovial chondromatosis of the shoulder. Arthrosc Tech.
3:e539–e545. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lim SJ, Chung HW, Choi YL, Moon YW, Seo JG
and Park YS: Operative treatment of primary synovial
osteochondromatosis of the hip. J Bone Joint Surg Am. 88:2456–2464.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Davis RI, Hamilton A and Biggart JD:
Primary synovial chondromatosis: A clinicopathologic review and
assessment of malignant potential. Hum Pathol. 29:683–688. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Buddingh EP, Krallman P, Neff JR, Nelson
M, Liu J and Bridge JA: Chromosome 6 abnormalities are recurrent in
synovial chondromatosis. Cancer Genet Cytogene. 140:18–22. 2003.
View Article : Google Scholar
|
|
10
|
Hermann G, Abdelwahab IF, Klein M, Kenan S
and Lewis M: Synovial chondromatosis. Skeletal Radiol. 24:298–300.
1995. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kumar A, Aggarwal A and Sahni VK: Primary
synovial osteochondroma of a subdeltoid bursa. Indian J Orthop.
44:104–107. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Villacin AB, Brigham LN and Bullough PG:
Primary and secondary synovial chondrometaplasia: Histopathologic
and clinicoradiologic differences. Hum Pathol. 10:439–451. 1979.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Milgram JW: Synovial osteochondromatosis:
A histopathological study of thirty cases. J Bone Joint Surg Am.
59:792–801. 1977.PubMed/NCBI
|
|
14
|
Chen A, Shih SL, Chen BF and Sheu CY:
Primary synovial osteochondromatosis of the first
metatarsophalangeal joint. Skeletal Radiol. 31:122–124. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Khan Z, Yousri T, Chakrabarti D, Awasthi R
and Ashok N: Primary synovial osteochondromatosis of the first
metatarsophalangeal joint, literature review of a rare presentation
and a case report. Foot Ankle Surg. 16:e1–e3. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Knoeller SM: Synovial osteochondromatosis
of the hip joint. Etiology, diagnostic investigation and therapy.
Acta Orthop Belg. 67:201–210. 2001.PubMed/NCBI
|
|
17
|
Kim SH, Hong SJ, Park JS, Cho JM, Kim EY,
Ahn JM and Park YS: Idiopathic synovial osteochondromatosis of the
hip: Radiographic and MR appearances in 15 patients. Korean J
Radiol. 3:254–259. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hamada J, Tamai K and Saotome K: Secondary
osteochondromatosis in the subacromial bursa: A report of two cases
and review of the literature. J Orthop Sci. 9:317–322. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Galat DD, Ackerman DB, Spoon D, Turner NS
and Shives TC: Synovial chondromatosis of the foot and ankle. Foot
Ankle Int. 29:312–317. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kim SR, Shin SJ, Seo KB, Teong CT and Hyun
CL: Giant extra-articular synovial osteochondromatosis of the sinus
tarsi: A case report. J Foot Ankle Surg. 52:227–230. 2013.
View Article : Google Scholar : PubMed/NCBI
|