Introduction
Parathyroid carcinoma (PC) is an extremely rare
endocrine malignancy, accounting for an estimated 0.005% of all
cancers (1). PC was first described
in 1904 by de Quevain (2) in a
patient who presented with a non-functioning lesion with normal
parathyroid function, and since then, studies on PC have been
published successively in the literature worldwide. Although the
majority of patients with PC present functioning lesions with
hyperparathyroidism, including extremely high levels of parathyroid
hormone (PTH) and serum calcium (3–5), it be
difficult to arrive at a diagnosis of PC pre-operatively or even
intraoperatively, for the reason that benign parathyroid tumors can
also present with hyperparathyroidism and occasionally the PC is
non-functioning (6). In addition, the
pathological diagnosis of malignancy is challenging. Due to its low
frequency, there is a lack of understanding with regard to this
endocrine malignancy, and its diagnosis and treatment therefore
present formidable challenges. The majority of the pathological
features of parathyroid carcinoma are not specific, and the
diagnosis may depend on demonstration of local invasion of adjacent
structures, despite the absence of metastasis. A previous study
reported that the diagnosis of PC is usually based on a combination
of clinical, histological signs and radiological in a context of
atypical presentation of PC (7). At
present, en bloc surgical resection remains the only curative
treatment, and a trend towards aggressive surgical management has
improved outcomes (8). Furthermore,
mortality is always associated with generalized metastases and
severe hypercalcemia, but due to its low frequency, the mortality
rate is unknown.
In the present study, the clinical presentation,
laboratory and imaging findings, surgical treatment and prognosis
of six cases of PC diagnosed in the Department of Pathology,
Zhejiang Province Cancer Hospital (Hangzhou, Zhejiang, China) are
presented, along with a brief review of literature.
Cases report
Patients
All cases of PC were diagnosed during a period of 13
years, between February 1999 and January 2012, in the Department of
Head and Neck Surgery of Zhejiang Province Cancer Hospital
(Hangzhou, China). None of the patients had a history of familiar
hyperparathyroidism. In all cases, the diagnosis of PC was
established by operative and pathological findings, combined with
the clinical presentation, such as elevated serum calcium and PTH
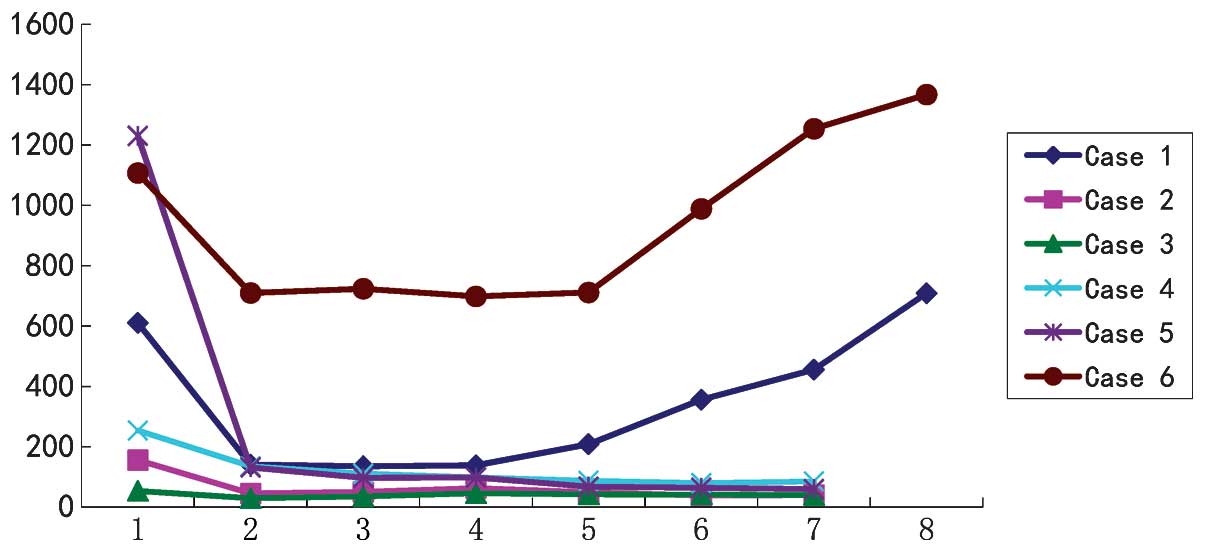
levels (Fig. 1). The experience
gained in the management of this tumor is presented. All patients
were followed up every 6 months (Table
I).
 | Table I.Clinical and surgical details of the 6
cases. |
Table I.
Clinical and surgical details of the 6
cases.
| Case no. | Age,
years/gender | Clinical
features | Location | Size, cm | Surgery | Other treatments | Follow-up |
|---|
| 1 | 48/F | Nausea, vomiting,
fatigue, polydipsia and polyuria for 2 years; weight loss and
trouble walking for 1 year | Left Upper | 3.5×3 | En bloc resection
with the ipsilateral lobe | NA | Succumbed at 24
months |
| 2 | 72/M | Dizziness and anxiety
for 6 months | Right Lower | 3×2.5 | En bloc resection
with the ipsilateral lobe | NA | NED at 36 months |
| 3 | 44/M | NA | Left Upper | 1×1 | En bloc resection
with near-total thyroidectomy | NA | NED at 48 months |
| 4 | 30/F | Hoarseness for 3
months | Left Lower | 2.5×2 | En bloc resection
with near-total thyroidectomy | NA | NED at 30 months |
| 5 | 69/F | Low limb pain for 2
years | Left Lower | 3×3 | En bloc resection
with the ipsilateral lobe | NA | NED at 24 months |
| 6 | 39/F | Painful joints and
bones, and lower back pain for 1 year | Left Lower | 6×5×4 | En bloc resection
with near-total thyroidectomy | Radiotherapy | Succumbed at 3
months |
Case 1
A 48-year-old female was admitted to the Department
of Head and Neck Surgery in September 2008, with a diagnosis of
nodular goiter and diabetes. The patient reported nausea, vomiting,
polydipsia, polyuria and fatigue for at least 2 years and also had
experienced trouble walking for the last year. Surgery for
nephrolithiasis was performed 20 years previously, however,
episodes of renal colic and hematuria occurred thereafter, which
the patient did not seek treatment for. During this hospitalization
period, laboratory tests found a normal blood sugar level, but a
high serum level of calcium (3 mmol/l; normal range, 2–2.6 mmol/l).
Ultrasound (US) scans revealed a multinodular goiter of the thyroid
gland. During exploratory surgery of the neck, a large 3.5-cm tumor
of the left upper parathyroid gland was found, firmly adhered to
the left lobe of the thyroid gland. An en bloc resection of the
parathyroid mass with near-total thyroidectomy was performed. The
histological diagnosis showed a PC that was 3.8 cm in maximum
diameter, with capsular and vessel invasion. However, the serum
calcium and PTH levels did not return to normal after the surgery.
After 3 months, computed tomography (CT) of the neck revealed a
2.5-cm mass in the suprasternal fossa, and the tumor was resected
en bloc with the ipsilateral neck lymph nodes in a second
procedure. The pathological examination revealed PC metastasis. Due
to economic reasons, the patient terminated therapy and was
discharged from hospital. According to the patient's relatives, the
patient succumbed due to generalized metastases and severe
debilitating hypercalcemia 2 years after the second surgery.
Case 2
A 72-year-old male who had been diagnosed with
nodular goiter was admitted to the Department of Head and Neck
Surgery of Zhejiang Province Cancer Hospital in August 2011, for
surgical management. The patient reported dizziness and anxiety
that had persisted for almost half a year. US demonstrated a
multinodular goiter and a 3×2.5-cm mass in contact with the lower
pole of the right lobe of the thyroid gland. The laboratory tests
revealed that the serum calcium level was mildly elevated (2.87
mmol/l), as well as the plasma PTH level (155.9 ng/l; normal range,
15–65 ng/l). The patient also underwent a pre-operative FNA biopsy,
but no evidence of PC was found. The patient underwent a palliative
near-total right thyroidectomy with en bloc resection of the
enlarged parathyroid mass and VI lymphadenectomy. The pathology
revealed PC and thyroid tissue with nodular hyperplasia. Serum
calcium and PTH levels returned to normal on the first
post-operative day. The patient remains alive and free of disease 3
years after the surgery.
Case 3
A 44-year-old male with a thyroid nodule that had
been physically apparent for a week presented to the Department of
Head and Neck Surgery of Zhejiang Province Cancer Hospital in April
2010. Upon physical examination, a palpable irregular mass was
discovered at the left upper pole of the thyroid gland. However,
the patient exhibited normal serum calcium and PTH levels, and did
not present with symptoms of hypercalcemia. An US scan revealed a
mass in the middle of the left thyroid gland, which raised the
suspicion of thyroid carcinoma. During surgery, a firm, 1×1-cm mass
was found at the left upper pole of the thyroid gland. A near-total
thyroidectomy with en bloc resection of the mass was performed. The
margins were found to be negative for neoplasm and the central neck
dissection demonstrated no positive lymph nodes. The pathology
revealed low-grade PC, with small nests of carcinoma cells present
in the surrounding thyroid tissue. The follow-up at 4 years
revealed normal serum calcium and PTH levels. The patient has been
free of recurrence since then.
Case 4
A 30-year-old female was admitted to the Department
of General Surgery of Shaoxing People's Hospital (Shaoxing, China)
in March 2005 and underwent en bloc resection of the left
parathyroid with the diagnosis of primary hyperparathyroidism
(PHPT). Following the surgery, the patient presented at the
Department of General Surgery at Peking University Shenzen Hospital
(Shenzen, China) in September 2011, with long-standing left-sided
true vocal fold paralysis and subsequently underwent a workup by an
otolaryngologist, which consisted of a thyroid US that demonstrated
a left-sided thyroid nodule. The patient underwent a near-total
thyroidectomy and the pathology indicated PC. However, the
patient's hoarseness persisted and positron emission tomography-CT
(PET-CT) imaging was performed, which showed recurrence of the
right neck mass, within 4 months of the initial thyroidectomy.
Calcium and PTH levels were beyond normal limits (serum calcium,
3.01 mmol/l; and serum PTH, 254.1 ng/l) at the time of the PET-CT.
The patient was then referred to the Department of Head and Neck
Surgery of Zhejiang Province Cancer Hospital in January 2012, for
evaluation of the recurrent right neck mass. According to the
previous examination, it was decided to excise the mass with a
central neck dissection to achieve a pathological diagnosis and
disease control. During surgery, a hard, 0.8-cm mass was found near
to the right recurrent laryngeal nerve. The tumor was resected en
bloc with a number of the left cervical lymph nodes. The
histological diagnosis showed no evidence of metastasis, but the
serum calcium and PTH levels remained high after the surgery. At a
follow-up at 2.5 years post-surgery, the patient was free of
recurrence.
Case 5
A 69-year-old female was admitted to the Department
of General Surgery of Zheijiang Province People's Hospital
(Hangzhou, China) in November 2011. The patient underwent
traditional high ligation and stripping of the great saphenous
vein, for the presence of varicosis of 3 years previously.
Following the surgery, the clinical symptoms improved. However, 2
months ago, the symptoms relapsed and the patient was admitted to
the Department of Head and Neck Surgery of Zhejiang Province Cancer
Hospital in February 1992, and on physical examination, a palpable
irregular mass was found at the left lower pole of the thyroid
gland. Laboratory tests established the diagnosis of PHPT. The
patient's serum calcium and PTH levels were 3.44 mmol/l and 131.6
ng/l, respectively, at the time of surgery. During the surgery, a
hard 3×3-cm mass was discovered in the back of the left lobe of the
thyroid gland. The mass was resected en bloc with the ipsilateral
thyroid lobe. The calcium and PTH levels returned to normal
immediately. The histological diagnosis showed PC with incipient
capsular invasion. The patient is currently alive and free of
disease 2 years after the surgery.
Case 6
A 39-year-old female patient with the diagnosis of
thyroid carcinoma was transferred to the Department of Head and
Neck Surgery of Zhejiang Province Cancer Hospital in February 1999.
The patient reported bone pain that had persisted for almost for a
year, mostly in the lower extremities and the lower back. A month
ago, these symptoms became worse, and the patient was unable to
walk or even stand. X-ray scanning of the lower limbs revealed
areas of osteolysis consistent with metastases. US revealed a
6×5×4-cm mass in contact with the lower pole of the left lobe of
the thyroid gland. Computed tomography scan of the thorax showed a
solitary pulmonary nodule in the left lung consistent with
metastasis. During surgery, the tumor behind the left lobe of the
thyroid gland was resected en bloc with the ipsilateral thyroid
lobe. The pathology revealed PC, and capsular invasion was
apparent. Pre-operative calcium levels were elevated (2.7–3.3
mmol/l); however, normocalcemia was achieved immediately. The
patient also underwent postoperative radiotherapy: The conventional
fractionation of 1.8 Gy per fraction and 5 fractions/week for 5
weeks (total dose, 45 gy). However, 3 months later, the patient's
clinical condition deteriorated due to generalized metastases and
the patient succumbed to cachexia.
Discussion
PC has, until recently, been regarded as an
exceedingly rare malignancy that is mostly observed in patients
treated for PHPT or thyroid tumors. The tumors occur equally in men
and women, in contrast to benign PHPT, which affects more women
than men. PC is a slow-growing tumor of low malignant potential,
but is a serious and frustrating clinical problem. PC is generally
associated with high calcium and extremely high PTH levels.
Patients are more likely to be symptomatic at the time of
presentation, and usually present with the symptoms of excessive
PTH excretion, including renal colic, painful joints and bones or
lower back pain, nocturia, thirst, polydipsia, anorexia,
gastrointestinal disturbances, abdominal pain, weight loss and
neuromuscular complaints, such as weakness and fatigue (9). The majority of these tumors are
functioning, however, they can also occur as a non-functioning PC.
The current study presents an even rarer case of PC with normal
serum calcium and PTH levels, no symptoms of hypercalcemia, and PC
identified during thyroidectomy. Few cases of incidental
non-functioning PC have been described in the last 100 years (20
cases since 1929) (10).
Non-functioning PC is usually clinically silent until it presents
with signs and symptoms of local growth and invasion (e.g.,
hoarseness, a neck mass and dysphagia).
No single laboratory finding is diagnostic of PC;
similar to benign PHPT, levels of serum calcium and PTH are
elevated in functioning PC. However, hypercalcemia in PC is usually
more profound, with a serum calcium level that is >3.0 mmol/l
and PTH levels as much as 1,230 ng/l above the upper limit of
normal (Fig. 1). These levels are
mildly elevated or near the upper limit of normal in the majority
of benign PHPT cases. In a study by Schaapveld et al
(11), it was demonstrated that a PTH
level 10 times the upper limit of the normal range had a positive
predictive value of 81% for PC. Furthermore, as shown in Fig. 1 of the present study, a post-operative
PTH level that did not decrease often indicated a poor prognosis or
the presence of other metastases. In addition, serum levels of
alkaline phosphatase, hypophsphatemia and hyperchloremic metabolic
acidosis are also raised in certain patients with PC (12). Recently, elevated plasma human
chorionic gonadotropin levels were documented in certain patients
with PC, but were normal in benign disease (13).
The commonly used imaging modalities include US, CT,
magnetic resonance imaging (MRI), PET and sestamibi scans (14–17). These
imaging studies are not very effective in determining the size and
location of abnormal parathyroid glands. However, the sensitivity
and specificity of these imaging modalities are increased when they
are used in combination. Ultrasonography is the most widely used
tool to localize primary and locally recurrent disease. Typical
features of PCs are lobulated, hypoechoic and relatively larger
parathyroid glands with ill-defined borders compared with adenomas
(14). Reeder et al (15) found that US has 100% accuracy in
detecting parathyroid lesions of ≥1 cm. In the present study cases,
US revealed a parathyroid neoplasm in one case only, where the size
of the neoplasm was 6 cm, and probably due to the coexistence of
multinodular goiter in the remaining 5 cases, as it was also proven
intraoperatively. Similar to US, sestamibi scanning has gained wide
acceptance as a precise method of assessing parathyroid lesions,
and it was performed in 3 of these cases (cases 1,4 and 6),
demonstrating the localization of the parathyroid adenomas.
However, sestamibi scans provide little benefit in differentiating
benign from malignant parathyroid lesions (16). Other diagnostic techniques, such as
CT, MRI and PET, may be useful when other imaging modalities fail
to localize the parathyroid neoplasm, and they are essential in the
identification of metastases and recurrent disease once the
diagnosis has been made (17).
The pre-operative diagnosis of PC can be extremely
challenging. In the present study, no patient was diagnosed with PC
prior to surgery (4 patients were suspected to have thyroid tumors
and 2 were suspected to have parathyroid adenomas). The diagnosis
becomes evident only after cytological and/or histological
analysis. However, fine-needle aspiration (FNA) biopsy should be
avoided when PC is suspected. Firstly, it is difficult to
differentiate between benign and malignant parathyroid lesions on
FNA biopsy (18). Secondly, danger of
possible procedure-related complications, such as bleeding and
tumor seeding along the needle tract has been reported (19). Only 1 patient (case 2) underwent
pre-operative FNA biopsy in the present study, but no evidence of
PC was found. Final histopathological descriptions of PC reported
in the 6 cases were varied and included capsular and vascular
invasion, sheets or lobules of tumor cells separated by dense
fibrous bands, pigmentation, necrosis and hemorrhage (Fig. 2). However, these pathological features
are not always present in PC. Furthermore, a number of these
features may also be observed in parathyroid adenomas or thyroid
tumors. Therefore, just like for other endocrine malignancies, the
diagnosis of PC is also based on the clinical presentation.
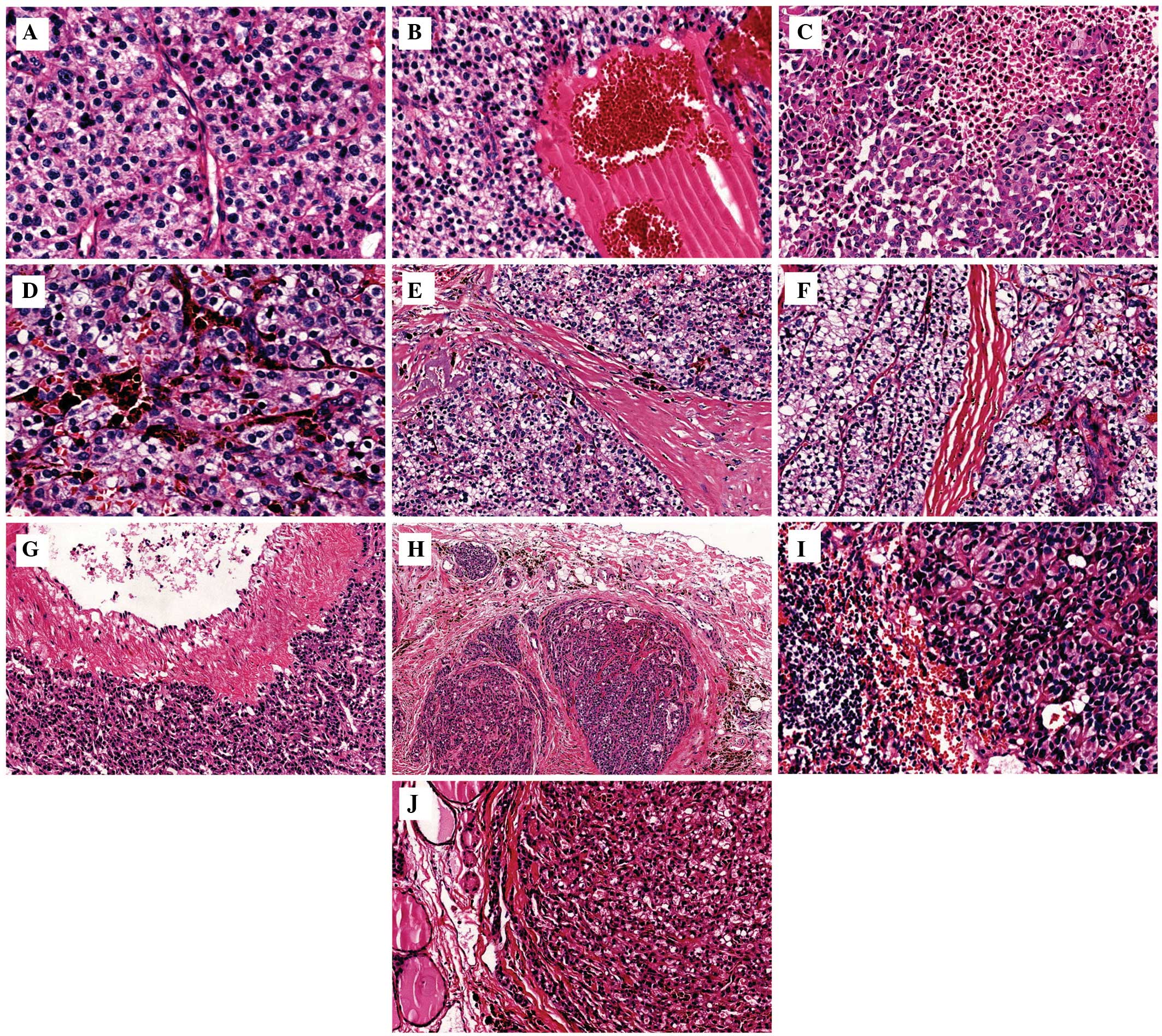 | Figure 2.Hematoxylin and eosin (HE) staining of
parathyroid carcinoma tissue. (A) Case 2, HE, ×100 magnification.
The nuclei of the tumor cells had an apparent unusual type, with
clear cytoplasm. (B) Case 6, HE, ×40 magnification. Cystic
structure containing blood. (C) Case 2, HE, ×40 magnification.
Tumor necrosis. (D) Case 2, HE, ×100 magnification. Pigmentation.
(E) Case 4, HE, ×40 magnification. Sheets or lobules of tumor cells
separated by dense fibrous bands. (F) Case 6, HE, ×40
magnification. Numerous blood vessels inside the tumor tissue. (G)
Case 1, HE, ×40 magnification. Infringement of the blood vessel
walls. (H) Case 5, HE, ×40 magnification. Capsular invasion. (I)
Case 1, HE, ×100 magnification. Lymphatic metastasis. (J) Case 3,
HE, ×40 magnification. Tumor cells invading the thyroid tissue. |
PCs are usually treated surgically, and the main
treatment goal should be the total removal of the PC with negative
margins. The majority of studies recommend en bloc resection at the
time of the initial surgery to offer the best opportunity for a
cure. Therefore, a high index of pre-operative suspicion and the
recognition of the possibility of malignancy during exploration are
extremely important. Adequate surgical excision includes en bloc
resection of the tumor together with the ipsilateral thyroid lobe,
and excision of any adjacent structures involved (9). The surgery must be performed carefully
in order to avoid rupturing the capsule of the tumor and seeding of
the surgical field, and the recurrent laryngeal nerve should be
resected only when it is involved and not functioning. Prophylactic
or radical neck resection is usually performed only if enlarged or
abnormal-appearing lymph nodes are found to be involved, as
unnecessary prophylactic radical neck dissection may increase the
risk of surgical complications (20).
In the present cases, en bloc resection of the tumor with
near-total thyroidectomy was performed. In cases 1, 5 and 6, the
ipsilateral thyroid lobe was resected en bloc due to local
infiltration, and in cases 2, 3 and 4, this was due to multinodular
goiters. The most common relapse pattern after the initial surgery
is local recurrence and distant metastases (e.g., lung, bone and
liver metastases). When technically possible, the resection of
local recurrence and metastatic lesions is recommended. Although an
absolute curative treatment is unlikely, this measure is justified
for the reduction of severe hypercalcemia, which is the main lethal
factor of advanced metastatic PC (21). Until recently, the data have been
limited for the treatment of PC with radiation therapy and
chemotherapy. PC has been traditionally considered as a
radio-resistant malignancy, with mainly disappointing results
observed in the majority of patients who are administered radiation
therapy. However, a recent retrospective study has advocated that
post-operative radiation therapy may be a strategy for optimizing
local control, which may produce a positive benefit on survival
(1). In case 6 of the present study,
radiation therapy and chemotherapy were attempted as treatment for
the bone and lung metastases, but it was not shown to be effective
in improving the survival or correcting the hypercalcemia of this
patient.
The prognosis of PC is variable. Disease recurrence
occurs in at least 50% of cases, and is usually indicated by
elevated PTH and serum calcium levels upon re-examination. In a
previously published study, the overall 5- and 10-year survival
rates ranged between <50 and 85%, and between 35 and 79%,
respectively. Early identification, appropriate initial surgery,
medical treatment for hypercalcemia and selective use of radiation
therapy offers the best prognosis (22). In the present cases, only two patients
developed recurrence within 2 years and succumbed due to
generalized metastases and severe debilitating hypercalcemia. The
remaining patients are alive and remain free of disease after their
first surgeries.
To conclude, the present case study highlighted that
more attention should be focused on patients with high levels of
PTH and serum calcium, and if there is a mass near the thyroid
gland, PC should be highly suspected. Furthermore, the information
gained may assist in the identification and treatment of the
disease in a more timely and adequate manner. Due to their rarity,
a multi-institutional pooling of cases is required for more insight
into PC in order to further understand this disease and to develop
more effective therapeutic methods.
Acknowledgements
This study was supported by the National Natural
Science Foundation of China (no. 81202127), the Natural Science
Foundation of Zhejiang Province (no. LY14H160014) and the
Traditional Chinese Medicine Science and Technology Plan of
Zhejiang Province (no. 2013ZA025).
References
|
1
|
Wei CH and Harari A: Parathyroid
carcinoma: Update and guidelines for management. Curr Treat Options
Oncol. 13:11–23. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
De Quevain F: Malignant aberrant
parathyroid. Dtsch Z Fuer Chir. 100:334–352. 1904.(In German).
|
|
3
|
Cryns VL, Rubio MP, Thor AD, Louis DN and
Arnold A: p53 abnormalities in human parathyroid carcinoma. J Clin
Endocrinol Metab. 78:1320–1324. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Meckeown PP, Mcgarity WC and Sewell CW:
Carcinoma of the parathyroid gland: Is it overdiagnosed? A report
of three cases. Am J Surg. 147:292–298. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sandelin K, Auer G, Bondeson L, Grimelius
L and Farnebo LO: Prognostic factors in parathyroid cancer: A
review of 95 cases. World J Surg. 16:724–731. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Levin KE, Galante M and Clark OH:
Parathyroid carcinoma versus parathyroid adenoma in patients with
profound hypercalcaemia. Surgery. 101:649–660. 1987.PubMed/NCBI
|
|
7
|
Rodriguez C, Naderi S, Hans C and Badoual
C: Parathyroid carcinoma: A difficult histological diagnosis. Eur
Annals Otorhinolaryngol Head Neck Dis. 129:157–159. 2012.
View Article : Google Scholar
|
|
8
|
Kassahun WT and Jonas S: Focus on
parathyroid carcinoma. Int J Surg. 9:13–19. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Abdelgadir Adam M, Untch BR and Olson JA
Jr: Parathyroid carcinoma: Current understanding and new insights
into gene expression and intraoperative parathyroid hormone
kinetics. Oncologist. 15:61–72. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Mazeh H, Prus D and Freund HR: Incidental
non-functional parathyroid carcinoma identified during
thyroidectomy. Isr Med Assoc J. 10:6592008.PubMed/NCBI
|
|
11
|
Schaapveld M, Jorna FH, Aben KK, Haak HR,
Plukker JT and Links TP: Incidence and prognosis of parathyroid
gland carcinoma: A population-based study in The Netherlands
estimating the preoperative diagnosis. Am J Surg. 202:590–597.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Haghighi P, Astarita RW, Wepsic HT and
Wolf PL: Concurrent primary parathyroid hyperplasia and parathyroid
carcinoma. Arch Pathol Lab Med. 107:349–350. 1983.PubMed/NCBI
|
|
13
|
Rubin MR, Bilezikian JP, Birken S and
Silverberg SJ: Human chorionic gonadotropin measurements in
parathyroid carcinoma. Eur J Endocrinol. 159:469–474. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Tamler R, Lewis MS, LiVolsi VA and Genden
EM: Parathyroid carcinoma: Ultrasonographic and histologic
features. Thyroid. 15:744–745. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Reeder SB, Desser TS, Weigel RJ and
Jeffrey RB: Sonography in primary hyperparathyroidism: Review with
emphasis on scanning technique. J Ultrasound Med. 21:539–552.
2002.PubMed/NCBI
|
|
16
|
Al-Sobhi S, Ashari LH and Ingemansson S:
Detection of metastatic parathyroid carcinoma with Tc-99 m
sestamibi imaging. Clin Nucl Med. 24:21–23. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sandelin K: Parathyroid carcinoma. Cancer
Treat Res. 89:183–192. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Mohebati A, Shaha A and Shah J:
Parathyroid carcinoma: Challenges in diagnosis and treatment.
Hematol Oncol Clin North Am. 26:1221–1238. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Spinelli C, Bonadio AG, Berti P, Materazzi
G and Miccoli P: Cutaneous spreading of parathyroid carcinoma after
fine needle aspiration cytology. J Endocrinol Invest. 23:255–257.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Clayman GL, Gonzalez HE, El-Naggar A and
Vassilopoulou-Sellin R: Parathyroid carcinoma: Evaluation and
interdisciplinary management. Cancer. 100:900–905. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Givi B and Shah JP: Parathyroid carcinoma.
Clin Oncol (R Coll Radiol). 22:498–507. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Harari A, Waring A, Fernandez-Ranvier G,
Hwang J, Suh I, Mitmaker E, Shen W, Gosnell J, Duh QY and Clark O:
Parathyroid carcinoma: A 43-year outcome and survival analysis. J
Clin Endocrinol Metab. 96:3679–3686. 2011. View Article : Google Scholar : PubMed/NCBI
|