Introduction
Giant cell tumor of the tendon sheath (GCTTS) is
also known as giant-cell synovioma and localized nodular
tenosynovitis. GCTTS is most commonly attached to the tendons of
the fingers, hands, and wrists, and affects both males and females
between the ages of 20 and 50 (1). It
is a common treatment to remove the tumor by the surgery, after
which it has a high recurrence (2).
GCTTS with bone destruction occurs rarely and is hard to remove
completely (3). Previous case studies
have shown that traditional surgical methods impact joint function
and that the tumors easily recur (3–5). The
present study reports the case of a young patient with a GCTTS who
underwent an artificial finger joint replacement; the tumor was
excised completely and the function of the joints was
recovered.
Case report
A 25-year-old male was admitted to The First
Affiliated Hospital, College of Meicine, ZheJiang University
(Hangzhou, Zhejiang, China) with tumor recurrence of the proximal
phalange of the ring finger on the right hand 4 years after partial
tumor resection surgery. The patient had no history of trauma or
infection and was previously healthy. A physical examination
revealed swelling of the proximal phalange of the finger without
clear cause, multiple nodules in the local areas of the proximal
interphalangeal point (PIP) without marked pain, and a lack of
phalangeal paresthesia, a blood circulation disorder or a finger
movement disorder. An X-ray of the right hand showed that the
distal bone of the proximal phalange of the ring finger on the
right hand had been destroyed. Although the diagnosis was
unfavorable, a local resection of the extra-articular joint was
performed to remove the tumor mass. The surgical pathology report
confirmed GCTSS. The tumor recurred after 1 year, with multiple
nodules found in the proximal phalange. According to the physical
examination, the soft tissue in the PIP of the finger was swollen,
but no skin redness was found. Multiple nodules could be locally
palpated with mild tenderness. The blood supply to the fingertip
was good, and the range of motion of the PIP was satisfactory. An
X-ray of the right hand showed distal bone destruction of the
proximal phalange of the ring finger on the right hand and swelling
of the soft tissue. Magnetic resonance image of the finger
(Fig. 1) showed that the distal bone
of the proximal phalange of the finger was structurally destroyed,
and the adjacent PIP capsule and periarticular soft tissue were
markedly swollen. Slightly elongated T1- and T2-weighted signals
were abnormal. The joint space remained. A giant cell tumor of the
bone was subsequently diagnosed (Figs.
2 and 3).
Resection of the tumor of the distal phalange was
performed under general anesthesia. Local swelling was found around
the PIP of the ring finger. Following incision of the skin and
subcutaneous tissue of the dorsal digit, the bulk of the tumor was
observed to be derived from the extensor tendon, with infiltration
into the PIP capsule and ligament. The local soft tissue was
severely damaged. The tumor mass was yellow-brown in color.
Subsequent to removal of the tumor and involved soft tissue, and
opening of the joint capsule, it was found that the tumor had
infiltrated into the joint and destroyed the bone. Part of the
tumor reached the joint, causing severe local damage of the bone.
No indication of a simple tumor resection was found. Subsequently,
an osteotomy was performed in the segment 0.5 cm from the proximal
and distal regions of the joint to completely remove the tumor
tissue. No significant tumor infiltration was found in the palmar
tendon or soft tissue. A drill was used to expand the space to
encompass nearly the entire bone marrow cavity of the intermediate
phalange, and a Swanson #2 artificial silicone joint (Wright
Medical Technology, Inc., Memphis, TN, USA) was placed inside the
joint space. The residual dorsal capsule and ligaments on either
side were sutured to strengthen and protect the joint. The wound
was repeatedly washed. The local soft tissue and skin were sutured
and wrapped with aseptic dressing. The treated finger was fixed in
a dorsiflexion position with an external plaster support.
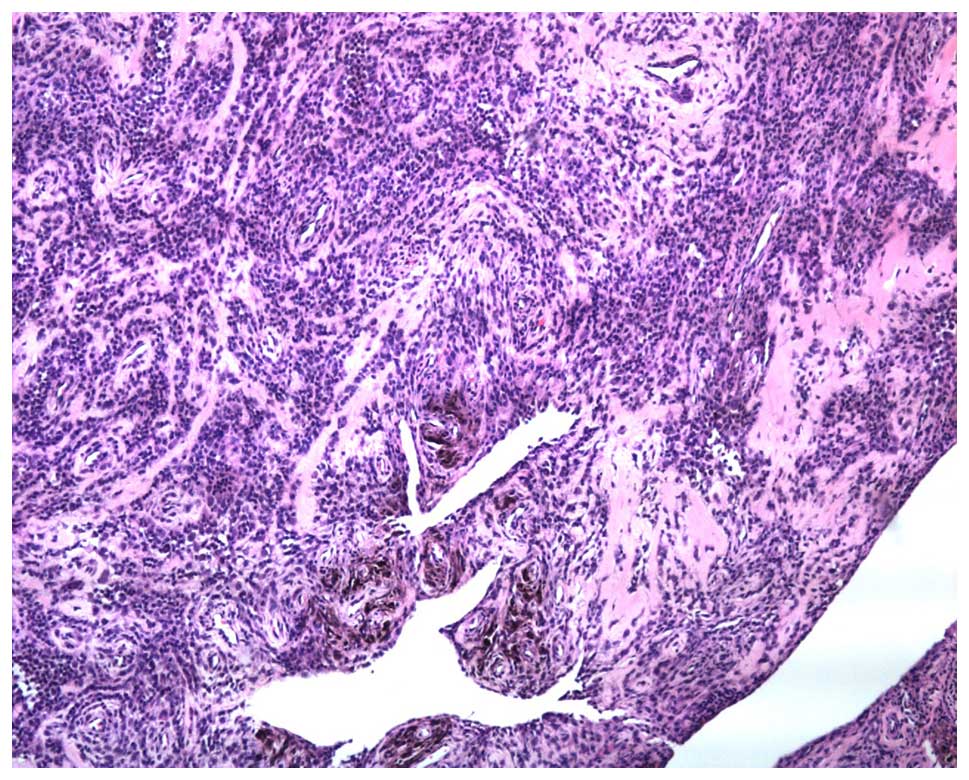
Irregular tissue measuring 2×1.2×0.2 cm was
submitted for examination. Upon magnification, the tumor was found
to be composed of a large number of round and synovial cells and a
few multinucleated giant cells. The tumor was lamellar in
arrangement, and a large amount of hemosiderin deposition was
found. These findings were indicative of a GCTTS (Fig. 4).
At 3–5 days post-surgery, the external plaster was
removed and functional exercises were begun. Orderly and gradual
exercise of the passive joint was conducted early during recovery,
with three groups of exercises being performed every day, and each
group being performed 10 times, while avoiding joint dislocation
and tendon rupture. Once the patient's pain and local inflammatory
edema subsided, active motion of the joint was gradually conducted.
A quantitative exercise program was begun based on the use of a
hand continuous passive motion machine. At discharge, the patient's
PIP motion had recovered to the pre-operative level (Fig. 5), with pre-operative and
post-operative disabilities of the arm, at shoulder and hand, and
total activity measurement values of 1.67 and 3.33, and 255 and
243°, respectively. Complications such as tumor recurrence, joint
dislocation and the requirement for prosthetic training were not
observed during a 5-year follow-up period.
Discussion
GCTTS is a common benign tumor arising in the tendon
sheath GCTTS occurs most often in the hands and feet (6). Pigmented villonodular synovitis (PVNS)
is a rare, idiopathic proliferative disorder of the synovium
(7). It usually affects the hip or
keen, but also occurs in hand or foot and the joint becomes
swollen. Therefore, PVNS is often confused with GCTTS. The use of
MRI may show a combination of synovial proliferation and soft
tissue masses, together with deposits of hemosiderin and bone
erosion, is highly diagnostic for PVNS, may also adequately
displays the location and extent of the lesion and its internal
structure (8).
Studies on GCTTS with bone destruction are
inconsistent. In a report by Moore et al, no bone
destruction was found among 115 cases of GCTTS (9). Bone destruction was detected in only 1
out of 51 cases of GCTTS reported by Fyfe and MacFarlane (10). Jones et al (11) studied 91 cases of GCTTS in the hand,
among which 11 cases showed evidence of cortical bone erosion
without bone destruction. However, certain studies have suggested
that GCTTS with bone destruction is not uncommon. According to a
study by Pan et al (12),
among 98 cases, the bone was normal in 55 cases, the tumor
infiltrated into the bone surface in 16 cases and the bone was
destroyed in 27 cases. In a study by Uriburu and Levy (13), 23.3% of 133 total cases showed tumor
intruding onto the bone surface and 11.3% exhibited bone
destruction. Additionally, in another study, X-ray analysis showed
lucent areas in single locular or multilocular cysts (14). On magnetic resonance imaging a further
study showed that the tumor grew along the sheath, revealing a low
signal intensity on T1-weighted images, but a high signal intensity
on T2-weighted images. After joint intrusion by GCTTS with bone
destruction, the occurrence rate of degenerative arthritis is 45%
(11).
During treatment, elimination of the tumor lesions,
including the soft tissue and bone, is favored. Recurrence is
associated with the use of a surgical resection. In the present
study, the previous tumor resection was performed at the expense of
PIP function and appearance. Taking into account the patient's age,
amputation was not an acceptable treatment. Complete resection of
the tumor is critical to curing the disease. Due to the invasive
properties of the tumor, joint stability must be considered if the
joint is to be retained. The tumor cannot be completely resected,
and thus the recurrence rate is high. The use of an artificial
joint as a treatment for PVNS can achieve complete tumor resection,
good functional recovery after surgery and reduce the likelihood of
relapse (15).
Cases of GCTTS on the hand that infringes the
joints, the tumor requires complete excision including the affected
articular surface and joint capsule in order to have a lower rate
of recurrence. The function of joints following reconstruction is a
problem after the surgery. Artificial joint replacement may excise
the tumor completely and also reconstruct the function of the
finger joint and it is therefore a good choice for the clinic.
Artificial joint replacement surgery of the GCTTS
that intruded into the distal region of the proximal phalange was
successfully performed in the present case. Lesions were removed
and PIP function was reconstructed.
References
|
1
|
Scott SJ and Jenkinson MD: Giant-cell
tumour of the tendon sheath. J Bone Joint Surg Br.
82:12062000.PubMed/NCBI
|
|
2
|
Garg B and Kotwal PP: Giant cell tumour of
the tendon sheath of the hand. J Orthop Surg (Hong Kong).
19:218–220. 2011.PubMed/NCBI
|
|
3
|
Athanasou NA, Quinn J, Ferguson DJ and
McGee JO: Bone resorption by macrophage polykaryons of giant cell
tumour of tendon sheath. Br J Cancer. 63:527–533. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Relwani J, Factor D, Khan F and Dutta A:
Giant cell tumour of the patellar tendon sheath - an unusual cause
of anterior knee pain: A case report. Knee. 10:145–148. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kitagawa Y, Ito H, Yokoyama M, Sawaizumi T
and Maeda S: The effect of cellular proliferative activity on
recurrence and local tumour extent of localized giant cell tumour
of tendon sheath. J Hand Surg Br. 29:604–607. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Demouy EH, Kaneko K, Bear HM and Rodriguez
RP: Giant cell tumor of the plantar tendon sheath: Role of MR
imaging in diagnosis. Case report. Clin Imaging. 17:153–155. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kanagawa H, Niki Y, Matsumoto H, Kosaki N,
Enomoto H, Morioka H, Toyama Y and Suda Y: Localized pigmented
villonodular synovitis presenting as a loose body following minor
trauma in the knee: A case report. Knee. 14:395–397. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Cheng XG, You YH, Liu W, Zhao T and Qu H:
MRI features of pigmented villonodular synovitis (PVNS). Clinical
rheumatology. 23:31–34. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Moore JR, Weiland AJ and Curtis RM:
Localized nodular tenosynovitis: Experience with 115 cases. J hand
surg Am. 9:412–417. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Fyfe IS and MacFarlane AU: Pigmented
villonodular synovitis of the hand. Hand. 12:179–188. 1980.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Jones FE, Soule EH and Conventry MB:
Fibrous xanthoma of synovium (giant cell tumor of tendon sheath,
pigmented nodular synovitis). A study of one hundred and eighteen
cases. J Bone Joint Surg Am. 51:76–86. 1969.PubMed/NCBI
|
|
12
|
Pan YW, Tian GL, Rong GW, Li C, Wang ZZ
and Tian W: Giant cell tumor of tendon sheath in hand combined with
bone invasion. Zhonghua Shou Wai Ke Za Zhi. 20:152–154. 2004.(In
Chinese).
|
|
13
|
Uriburu IJ and Levy VD: Intraosseous
growth of giant cell tumors of the tendon sheath (localized nodular
tenosynovitis) of the digits: Report of 15 cases. J hand surg Am.
23:732–736. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Midletton WD, Patel V, Teefey SA and Boyer
MI: Giant cell tumor of the tendon sheath: Analysis of scanographic
finding. AJR Am J Roentgenol. 183:337–339. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lang L and Guo W: Treatment of diffused
giant cell tumors of tendon sheath by rotation hinge prosthesis.
Zhongguo Gu Yu Yuan Jie Za Zhi. 5:83–86. 2006.(In Chinese).
|