Introduction
Despite being first reported by Billroth in 1879
(1), until now, the occurrence of
multiple primary malignancies in a single patient has been
relatively rare. Simultaneous detection of malignancies in the
thyroid and liver represents an uncommon event, despite the
increasing overall incidence of malignancies. Intrahepatic
cholangiocarcinoma (ICC) is a rare histopathological type of
primary liver cancer, which accounts for only 5–10% of liver cancer
(2). Common metastatic sites of ICC
are regional lymph nodes and adjacent organs, while distant bone
metastasis is rare (3). The prognosis
of ICC remains poor due to its late clinical presentation and rapid
recurrence, as well as the lack of adequate treatment strategies.
In addition to curative resection, the potential benefit of other
treatments in patient survival remains controversial (4). The present study reports a case of
double primary cancer, comprising ICC with bone metastases in
atypical locations, as well as thyroid carcinoma. The report
details the therapeutic strategy used for inoperable and bone
metastatic ICC, to provide useful information on this rare
condition. Written informed consent was obtained from the patient's
family.
Case report
A 58-year-old woman was admitted to Ling Nan
Hospital (Guangzhou, China) in January 2010 complaining of repeated
pain at the left hip for 2 months, accompanied by difficulty
walking for 1 week. Clinical examination revealed a non-tender,
palpable thyroid lump and abdominal mass at the epigastric area,
while a gynecological examination was normal. The Patrick test,
which is used to evaluate the pathology of the hip or sacroiliac
joint, was performed by flexing, abducting and externally rotating
each leg in turn. If pain is elicited on the ipsilateral side
anteriorly, it is suggestive of a hip joint disorder on the same
side. If pain is elicited on the contralateral side posteriorly
around the sacroiliac joint, it is suggestive of pain mediated by
dysfunction in that joint. In the current patient, the test was
positive on the left, but negative on the right.
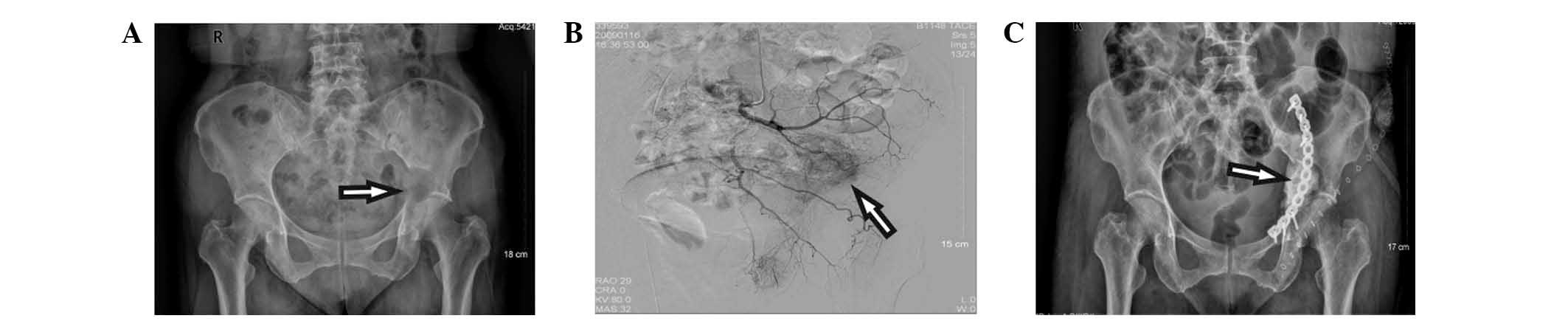
Pelvic X-ray revealed an osteolytic lesion at the
upper margin of the left acetabulum (Fig.
1A). Ultrasound showed that the thyroid lump was a carcinoma
located at the right lobe, and that there were multiple occupying
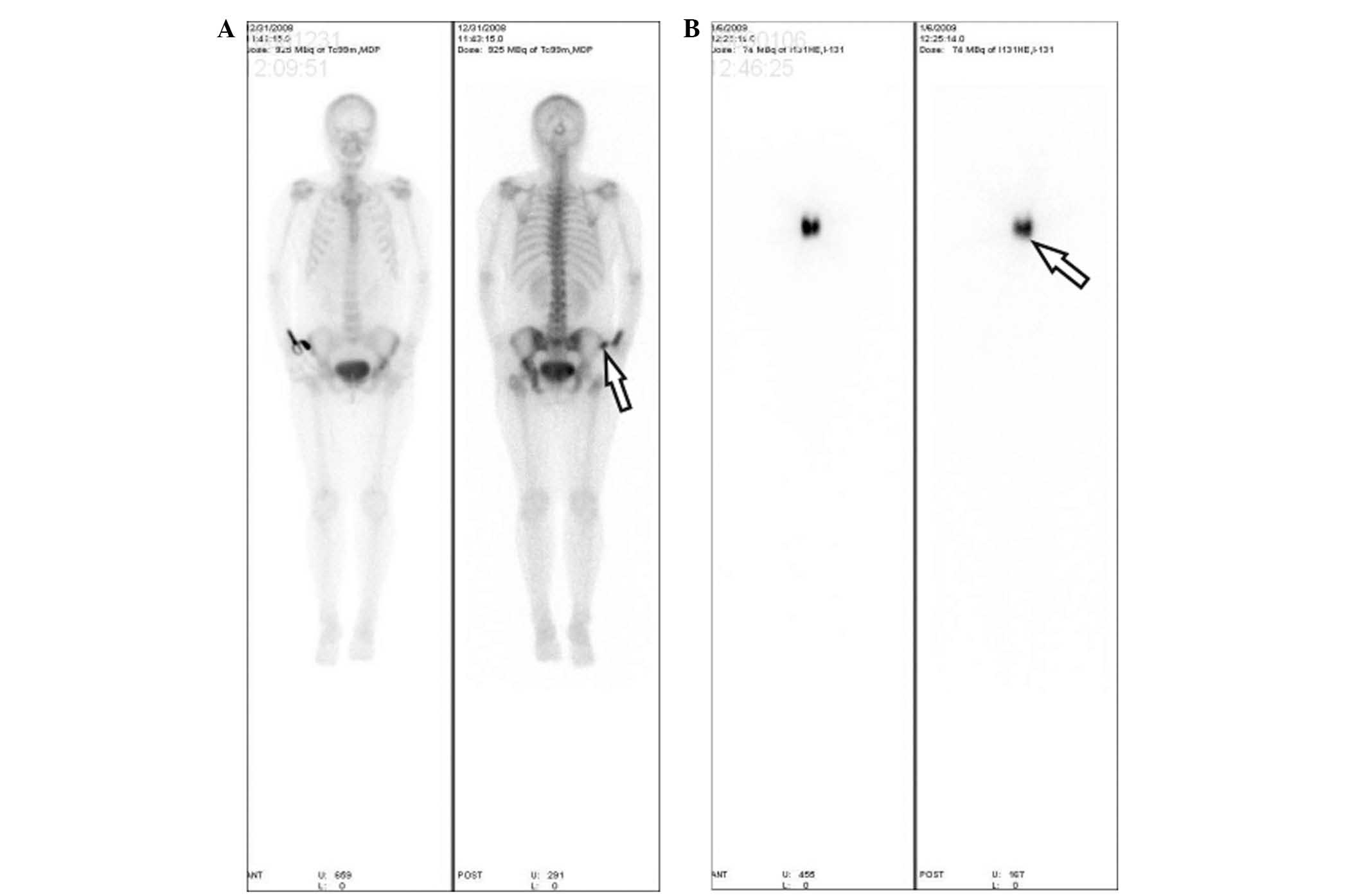
lesions in the liver. Biopsy specimens of the osteolytic lesion
identified a metastatic, moderately-differentiated adenocarcinoma
of unknown origin. Bone radionuclide scanning and an I-131 total
body scan were conducted to reach the final diagnosis (Fig. 2). Subsequently, ultrasound-guided
fine-needle aspiration and core biopsy were performed. The smears
revealed crowded clusters and sheets of malignant cells with
glandular arrangement, while immunohistochemistry revealed that the
tumor cells were positive for cytokeratin (CK) 7 and CK19, but
negative for CK20. Therefore, ICC with bone metastases was
diagnosed.
Transarterial chemoembolization (TACE) was used to
control the primary lesion, while simultaneously, internal iliac
arteriography and embolization were performed to control the
metastatic bone tumor (Fig. 1B). One
month later, the patient still experienced difficulty walking.
Therefore, an operation comprising metastatic tumor curettage,
cement infilling and internal plate fixation was performed
(Fig. 1C). Several days subsequent to
surgery, the patient was able to walk unaided, and the pain in the
left hip was alleviated. Due to the poor results of the TACE,
percutaneous port catheter system implantation via the left
subclavian artery was used for further treatment. The patient
subsequently commenced three courses of gemcitabine-based
chemotherapy. Aggressive radiotherapy or single-fraction
irradiation were not utilized for further treatment, at the request
of the patient's family. The patient succumbed 9 months following
initial diagnosis.
Discussion
Multiple primary malignancies are divided into two
categories, synchronous and metachronous malignancies, based on the
length of time between tumor diagnoses (5). Synchronous cancers are defined as those
where secondary tumors occur simultaneously or within 6 months of
diagnosis of the primary malignancy (6). Due to the increased life expectancy and
improved screening programs, the early detection ratio for multiple
primary malignancies is expected to increase (7). Among those patients with synchronous
multiple malignancies, double primary cancer was most commonly
observed, while cases of triple cancer or more occurred in <1%
of patients (8).
ICC, arising from the epithelial cells of the
intrahepatic biliary tree, is a rare type of primary liver cancer,
which has exhibited a global increasing trend in recent years
(9). The incidence of ICC increases
with age, and peaks in the sixth to seventh decade of life
(4). To date, ICC synchronous with
HCC (10), ampullary carcinoid
(11), lymphoma (12), lung squamous cell carcinoma (13,
lymphoepithelioma (14) and renal
cell carcinoma (15) have been
reported, while few cases have been reported synchronous with
thyroid carcinoma. ICC typically metastasizes to the regional lymph
nodes, liver, lungs and adjacent organs. Bone metastasis from ICC
to the acetabular is particularly rare. By contrast, bone
metastases are more commonly associated with other primary tumor
locations, for example the lung, breast and thyroid. Therefore, the
metastatic osteolytic adenocarcinoma of unknown origin was more
likely to have developed from the thyroid carcinoma than the ICC.
Unexpectedly, the metastatic lesion identified in the present case
was confirmed to have arisen from ICC, as indicated by I-131 scan
and liver lesion biopsy.
Although the mechanisms underlying the occurrence of
multiple primary cancer are yet to be fully elucidated, there are a
number of established risk factors for ICC. To the best of our
knowledge, several factors have previously been defined, including
parasitic infection, primary sclerosing cholangitis, biliary-duct
cysts and hepatolithiasis (16). In
addition, other potential risk factors include hepatitis,
cirrhosis, diabetes, inflammatory bowel disease, alcohol drinking
and tobacco smoking (17). In terms
of the present case, diabetes and chronic hepatitis B virus
infection may be responsible for the occurrence of ICC.
Currently, there is no established therapy for the
treatment of synchronous primary cancer following diagnosis.
Treatment may involve curative surgical resection of each cancer,
radiotherapy and chemotherapy, depending on the location of the
tumors. In the present case of synchronous primary cancer, due to
the advanced disease stage, the aims of palliative therapy were to
control local tumor growth and relieve symptoms, while improving
and preserving the patient's quality of life.
Previously published data have reported that there
are four categories of metastatic acetabular tumor (18). The majority of cases were detected by
painful symptoms or neurological signs resulting from structural
damage, periosteal irritation and nerve entrapment (19). For these patients, resection and
reconstruction of the metastatic lesions was able to improve
quality of life by increasing mobility and reducing pain (20). In the present case, minimally invasive
treatment failed to control the metastatic tumor, therefore
surgical intervention was utilized and achieved effective
results.
Preoperative TACE has been used to control primary
liver neoplasm (21). However, the
outcome for certain patients is unsatisfactory due to the malignant
nature of the tumor. ICC has been shown to be resistant to common
chemotherapy, with an unacceptably low response rate (22). Various chemotherapeutic agents have
been evaluated for the treatment of ICC in numerous clinical
trials, however no standard chemotherapeutic regimen has yet been
identified (23–25). Double gemcitabine and cisplatin
therapy is currently considered the first-line therapy for patients
with advanced disease (26). Although
no randomized trials have been conducted to support the use of
adjuvant treatment, gemcitabine-based chemotherapy combined with
TACE may show promising efficacy with respect to survival and
quality of life for advanced ICC with bone metastasis. Patients
with poor prognosis may potentially benefit from the shorter
treatment duration, due to their limited life expectancy.
Despite their infrequency, double primary
malignancies, for example intrahepatic cholangiocarcinoma with bone
metastases and thyroid carcinoma, should be considered seriously.
Multiplicity of primary malignancies itself is not necessarily
indicative of a poor prognosis. The results of the present case
suggest that early diagnosis, together with positive
multidisciplinary treatments, may show promising efficacy with
respect to patient survival and quality of life. A study of
patients from a large, multicenter and multigeographical cohort may
facilitate validation of these results and reach more powerful
conclusions.
References
|
1
|
Billroth T and Klinik Chirurgische Wien:
Nebst einem Gesammt-Bericht über die chirurgischen Kliniken in
Zürich und Wien während der Jahre 1860–1876. Erfahrungen auf dem
Gebiet der practischen Chirurgie (Hirschwald Berlin). 1879.(In
German).
|
|
2
|
Tsai S, Nathan H and Pawlik TM: Primary
liver cancer: Intrahepatic cholangiocarcinoma emerges from the
shadows. Updates Surg. 62:5–9. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Shirabe K, Shimada M, Harimoto N,
Sugimachi K, Yamashita Y, Tsujita E and Aishima S: Intrahepatic
cholangiocarcinoma: Its mode of spreading and therapeutic
modalities. Surgery. 131:S159–S164. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yang J and Yan LN: Current status of
intrahepatic cholangiocarcinoma. World J Gastroenterol.
14:6289–6297. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Suzuki T, Takahashi H, Yao K, Inagi K,
Nakayama M, Makoshi T, Nagai H and Okamoto M: Multiple primary
malignancies in the head and neck: A clinical review of 121
patients. Acta Otolaryngol Suppl. 547:88–92. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Moertel CG: Multiple primary malignant
neoplasms: Historical perspectives. Cancer. 40(Suppl): 1786–1792.
1977. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Moertel CG: Incidence and significance of
multiple primary malignant neoplasms. Ann NY Acad Sci.
114:2012.
|
|
8
|
Luciani A and Balducci L: Multiple primary
malignancies. Semin Oncol. 31:264–273. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Poultsides GA, Zhu AX, Choti MA and Pawlik
TM: Intrahepatic cholangiocarcinoma. Surg Clin North Am.
90:817–837. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Jung KS, Chun KH, Choi GH, Jeon HM, Shin
HS, Park YN and Park JY: Synchronous development of intrahepatic
cholangiocarcinoma and hepatocellular carcinoma in different sites
of the liver with chronic B-viral hepatitis: Two case reports. BMC
Res Notes. 6:5202013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Takeuchi Y, Nagata K, Yokota T, Handa M,
Matsunaga H, Nishio Y and Kusugami K: Von Recklinghausen disease
associated with intrahepatic cholangiocarcinoma and ampullary
carcinoid. Nihon Naika Gakkai Zasshi. 90:2467–2469. 2001.(In
Japanese). View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Fwu CW, Chien YC, You SL, Nelson KE, Kirk
GD, Kuo HS, Feinleib M and Chen CJ: Hepatitis B virus infection and
risk of intrahepatic cholangiocarcinoma and non-Hodgkin lymphoma: A
cohort study of parous women in Taiwan. Hepatology. 53:1217–1225.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Murakami T, Nishikawa H, Koshikawa Y,
Okabe Y, Wakasa T and Osaki Y: Double primary cancers: Intrahepatic
cholangiocarcinoma with myocardial metastases and lung squamous
cell carcinoma. Intern Med. 51:2329–2335. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Henderson-Jackson E, Nasir NA, Hakam A,
Nasir A and Coppola D: Primary mixed lymphoepithelioma-like
carcinoma and intra-hepatic cholangiocarcinoma: A case report and
review of literature. Int J Clin Exp Pathol. 3:736–741.
2010.PubMed/NCBI
|
|
15
|
Anthony MP, Mak H and Khong PL: An unusual
case of synchronous renal cell carcinoma in a horseshoe kidney and
intrahepatic cholangiocarcinoma. Clin Nucl Med. 34:922–923. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Palmer WC and Patel T: Are common factors
involved in the pathogenesis of primary liver cancers? A
meta-analysis of risk factors for intrahepatic cholangiocarcinoma.
J Hepatol. 57:69–76. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Tyson GL and El-Serag HB: Risk factors for
cholangiocarcinoma. Hepatology. 54:173–184. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Harrington KD: The management of
acetabular insufficiency secondary to metastatic malignant disease.
J Bone Joint Surg Am. 63:653–664. 1981.PubMed/NCBI
|
|
19
|
Shahid M, Saunders T, Jeys L and Grimer R:
The outcome of surgical treatment for peri-acetabular metastases.
Bone Joint J. 96-B:132–136. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Hoell S, Dedy N, Gosheger G, Dieckmann R,
Daniilidis K and Hardes J: The Burch-Schneider cage for
reconstruction after metastatic destruction of the acetabulum:
Outcome and complications. Arch Orthop Trauma Surg. 132:405–410.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bester L, Meteling B, Boshell D, Chua TC
and Morris DL: Transarterial chemoembolisation and
radioembolisation for the treatment of primary liver cancer and
secondary liver cancer: a review of the literature. J Med Imaging
Radiat Oncol. 58:341–352. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Furuse J, Kasuga A, Takasu A, Kitamura H
and Nagashima F: Role of chemotherapy in treatments for biliary
tract cancer. J Hepatobiliary Pancreat Sci. 19:337–341. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Valle J, Wasan H, Palmer DH, Cunningham D,
Anthoney A, Maraveyas A, Madhusudan S, Iveson T, Hughes S, Pereira
SP, et al: ABC-02 Trial Investigators: Cisplatin plus gemcitabine
versus gemcitabine for biliary tract cancer. N Engl J Med.
362:1273–1281. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Gruenberger B, Schueller J, Heubrandtner
U, Wrba F, Tamandl D, Kaczirek K, Roka R, Freimann-Pircher S and
Gruenberger T: Cetuximab, gemcitabine, and oxaliplatin in patients
with unresectable advanced or metastatic biliary tract cancer: A
phase 2 study. Lancet Oncol. 11:1142–1148. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Eckmann KR, Patel DK, Landgraf A, Slade
JH, Lin E, Kaur H, Loyer E, Weatherly JM and Javle M: Chemotherapy
outcomes for the treatment of unresectable intrahepatic and hilar
cholangiocarcinoma: A retrospective analysis. Gastrointest Cancer
Res. 4:155–160. 2011.PubMed/NCBI
|
|
26
|
Maithel SK, Gamblin TC, Kamel I,
Corona-Villalobos CP, Thomas M and Pawlik TM: Multidisciplinary
approaches to intrahepatic cholangiocarcinoma. Cancer.
119:3929–3942. 2013. View Article : Google Scholar : PubMed/NCBI
|