Introduction
Epithelioid angiomyolipoma (EAML) is an independent
subtype of tumor within the family of perivascular epithelioid cell
tumors (PEComas) (1). EAML is a rare
variant of renal AML with malignant potential, and is characterized
by a predominance of human melanoma black (HMB)-45+
epithelioid cells and absence of adipocytes (2). Malignant EAML has been recently
described as a rare tumor of the kidney, although its existence had
been previously questioned (3).
Several cases of EAML metastasized to the liver, lung and bone have
been reported in the literature (4,5). In the
present report, the case of a malignant renal EAML is described.
The diagnosis was established by histological findings, and
confirmed by the presence of multiple metastases. The diagnosis of
EAML may be challenging, due to the similarity of its epithelioid
morphology with that of renal cell carcinoma (RCC) (6). Therefore, an awareness of this entity
and its characteristic features, including immunoreactivity with
HMB-45, may aid its identification. Furthermore, the classification
criterion for this malignancy proposed in the present study may
contribute to understanding the pathological findings and clinical
behavior of malignant renal EAML. The family of the patient
provided written informed consent.
Case report
A 48-year-old woman with a history of flank pain in
the right-side for ~10 days presented to the Department of Urology
of Tianjin Baodi Hospital of Tianjin Medical University (Tianjin,
China). Physical examination identified a palpable tender mass in
the right flank. The patient did not present gross hematuria. No
history of tuberous sclerosis syndrome (TSC) was recorded for the
patient or her family, and the past medical history of the patient
was not contributory. The results of routine laboratory tests,
including kidney function, were normal, with the exception of
macroscopic hematuria. Ultrasound scan revealed a mass arising from
the lower pole of the right kidney, which did not display a typical
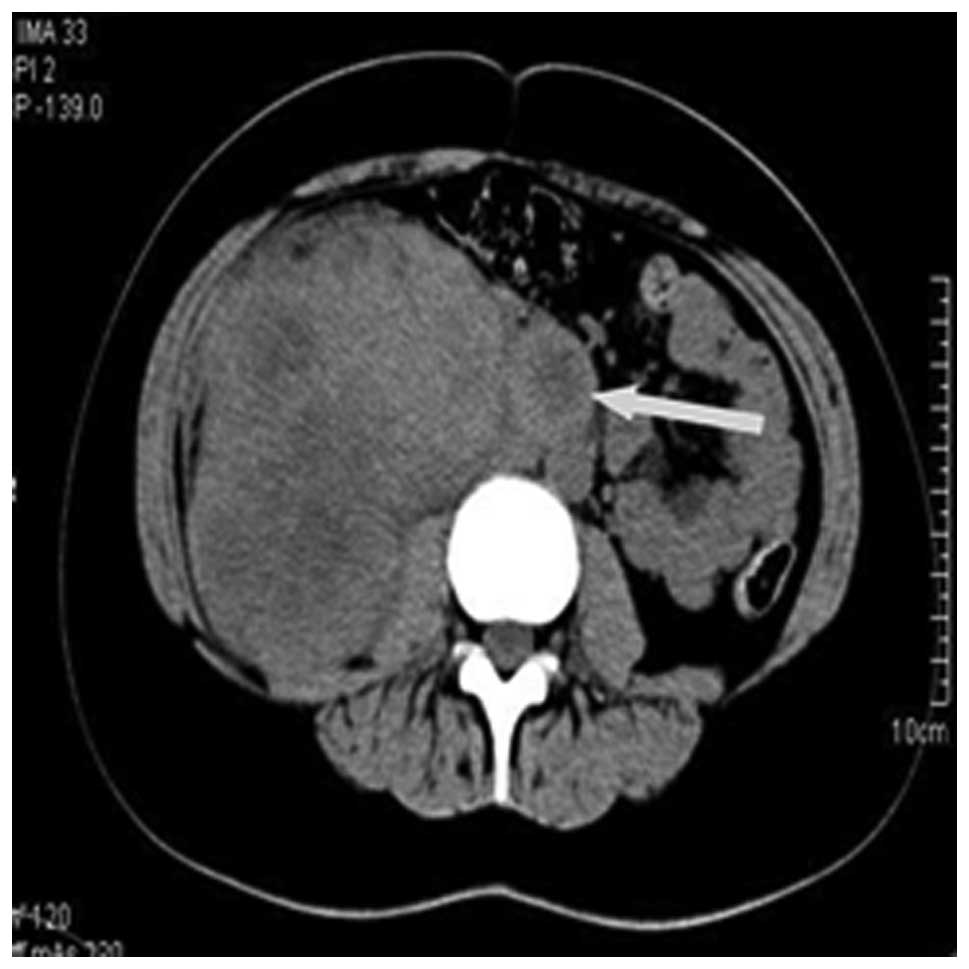
adipose ultrasonographic echo. Computed tomography (CT) was
performed using a SOMATOM Definition double-source helical scanner
CT (Siemens, Medical Systems, Germany) and detected a soft tissue
mass of heterogeneous density, which measured ~13×12×11 cm and
occupied the majority of the right kidney. In addition, several
enlarged lymph nodes were noticed in the retroperitoneal space,
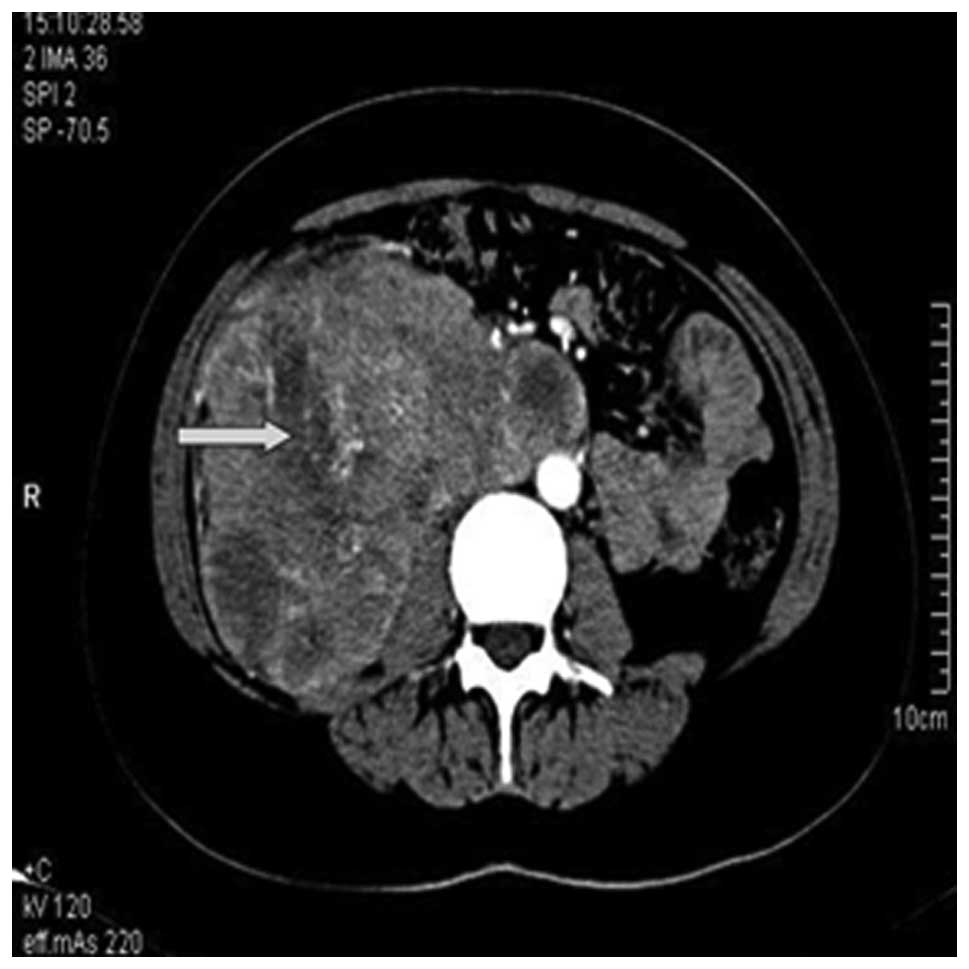
with the biggest node measuring ~3 cm in diameter (Fig. 1). The majority of the right renal
pelvis and normal renal parenchyma structures were destroyed, and
no obvious adipose tissues were detected. Scattered necrosis and
calcification were occasionally observed, and the lesion exhibited
moderate heterogeneous enhancement during enhanced scanning
(Fig. 2). Radiographically, the mass
was considered to be RCC. During surgery, several enlarged lymph
nodes were identified, in addition to a large mass in the right
kidney with extension to the posterior peritoneum. The mass was
contiguous with the mid-lower pole of the left kidney, without
distinct surgical plane. The patient successfully underwent radical
right nephrectomy with retroperitoneal lymphadenectomy, and
experienced an uneventful recovery.
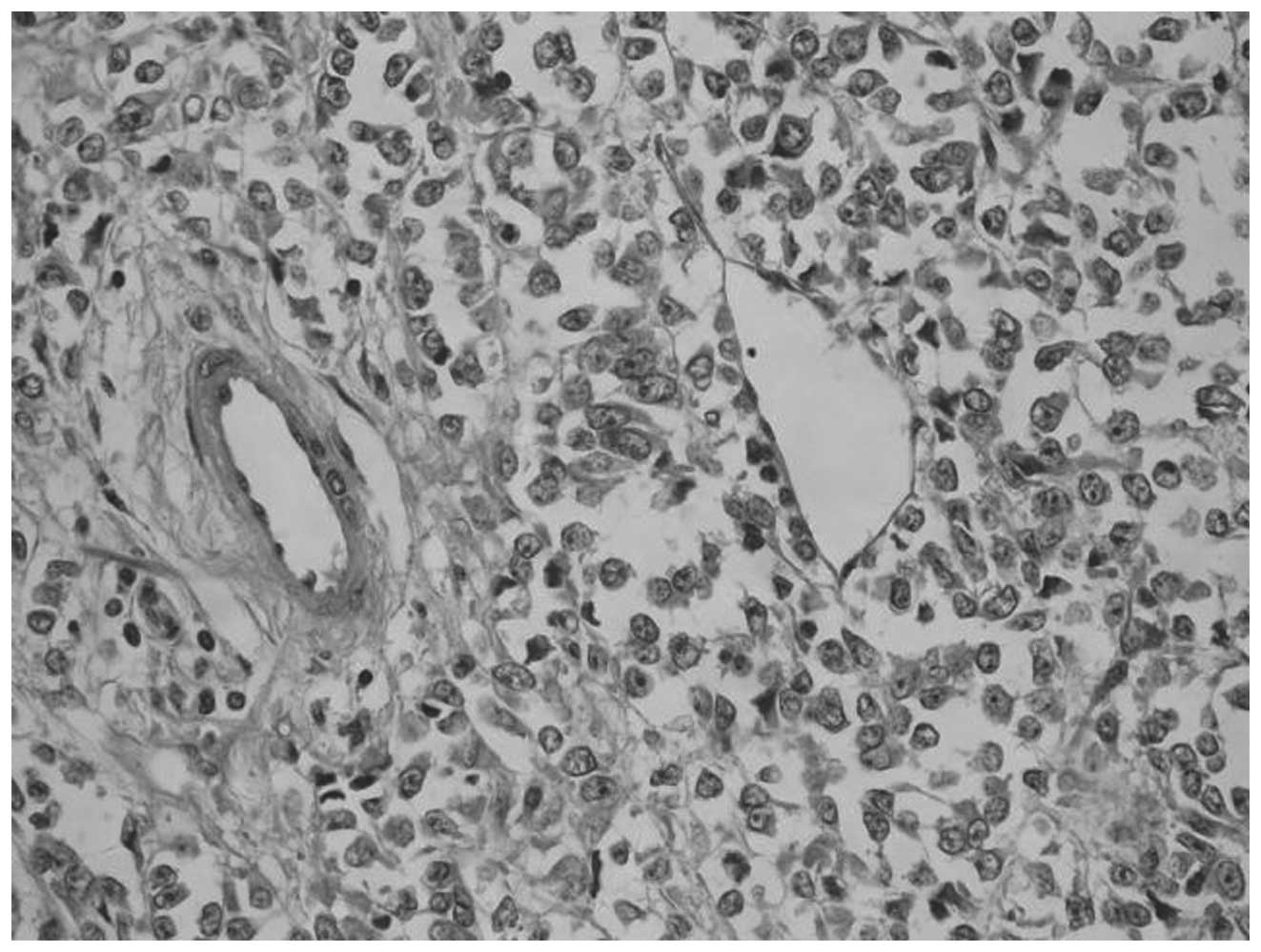
On histological examination, the specimen was
brownish, and necrosis was observed. The tumor was composed of
large polygonal epithelioid cells with abundant eosinophilic
cytoplasm and markedly bizarre atypical nuclei, which were
different from conventional AML (Fig.
3). While adipose tissue was scarcely observed, mitotic figures
were often encountered, and atypical mitoses were also detected.
Identical tumor cells were observed in the metastatic lymph nodes
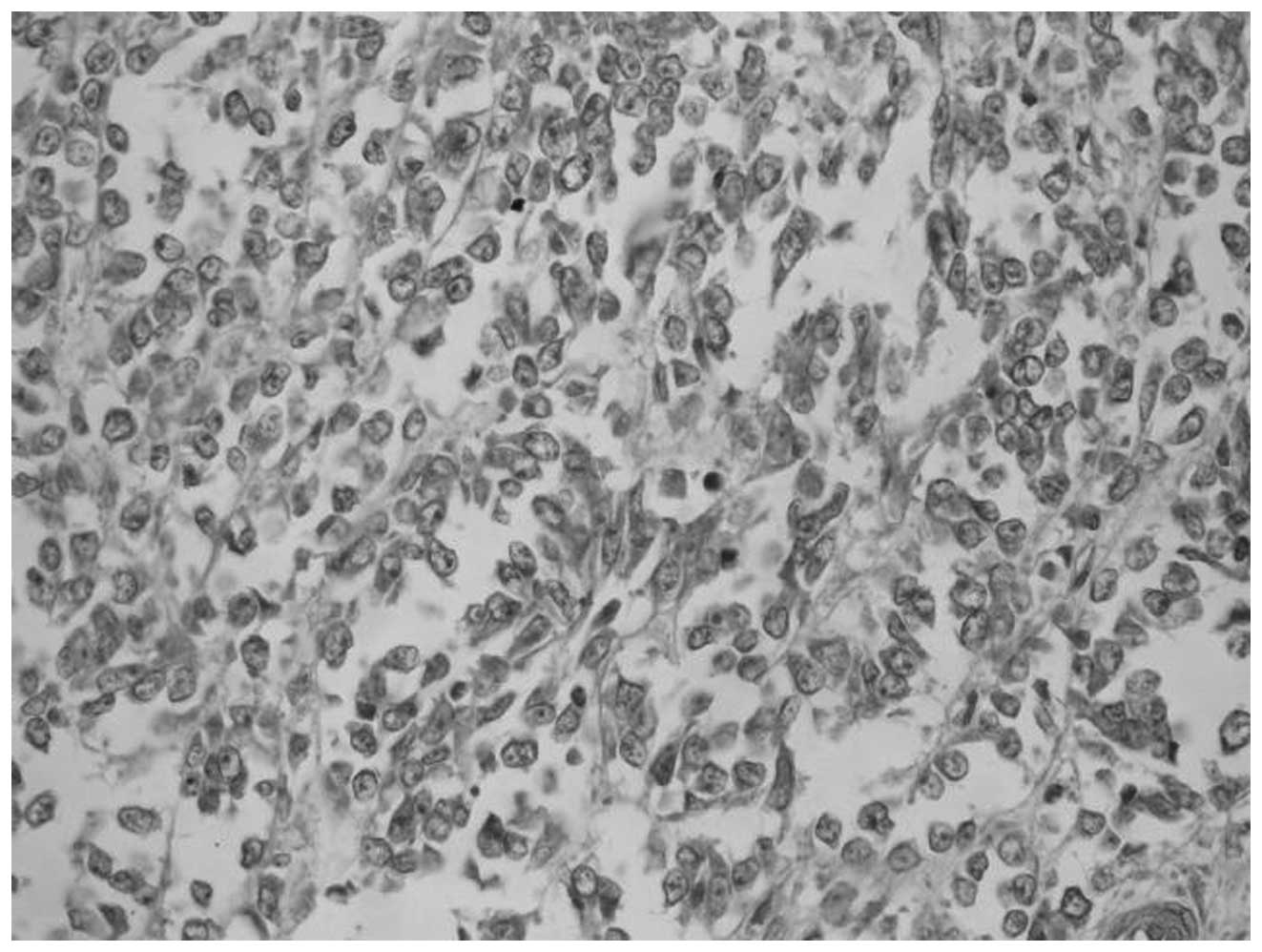
lesions and renal veins. The sections were immunostained using
monoclonal anti-HMB-45 (no. SIG-3116; Covance, Inc., Princeton, NJ,
USA), anti-desmin (no. ab919901; Abcam, Cambridge, UK) and
anti-melan-A (ab187369; Abcam) and counterstained with hematoxylin
and eosin (Abcam). Immunohistochemical staining confirmed that the
epithelioid cells focally expressed HMB-45 (Fig. 4), and were moderately positive for
melan-A and desmin. Thus, the pathological diagnosis was EAML with
malignant tendency. Postoperative abdominal magnetic resonance
imaging and chest X-ray scan conducted at 16 months of follow-up
identified multiple liver and lung metastases. A fine-needle
aspiration of the liver demonstrated the presence of EAML, which
was morphologically and immunohistochemically identical to the
primary renal tumor, thus confirming the existence of malignant
EAML. In consequence, the patient was subjected to chemotherapy.
However, no reduction in the size of the tumors was observed
following two cycles of chemotherapy with doxorubicin and
cisplatinum. The patient was then advised to participate in a
clinical trial (enrolment no. 33567; 2013-12-8) studying the
effects of sorafenib in the treatment of renal malignant tumors.
The patient received two doses of 400 mg sorafenib for two months.
However, the treatment was not effective, and the metastatic
lesions became more aggressive, extending to the liver, lungs and
bones. The patient succumbed to neoplastic progression of the
disease six months later.
Discussion
EAML has been recognized as a mesenchymal tumor in
the 2004 World Health Organization classification of renal tumors
(7), and a member of the family of
PEComas (8), which may occur
sporadically or in association with TSC (9). EAML is considered a potentially
malignant neoplasm, since ~a third of the reported cases of EAML
developed metastatic lesions (10).
Radiologically, the diagnosis of malignant EAML is difficult. While
renal AML may be detected by CT, due to its adipose content,
malignant EAML may be difficult to diagnose, due to the low
abundance of adipocytes in this tumor (11). Upon review of the current literature,
a limited number of imaging studies on malignant EAML were
identified (12,13). A previous study reported the diagnosis
of a case of AML without fat density on CT (14). Therefore, fat density does not appear
to be crucial for distinguishing malignant EAML from AML. In the
present case, CT identified a renal mass that exhibited central low
attenuation consistent with necrosis, in addition to multiple
enlarged retroperitoneal lymph nodes. This CT appearance was
similar to typical RCC (15),
therefore raising the suspicion of malignancy. Malignant tumors
often share certain common features, including relatively large
size, heterogeneous attenuation, irregular contour, necrosis and
multiple metastases (11).
Multicentric EAML may be difficult to differentiate from metastasis
in the presence of tumor thrombus in the inferior vena cava or in
the adjacent organs, or when invasion of lymph nodes or blood
vessels exists (16). The imaging
features of the tumor in the present case included large size with
necrosis on non-contrast CT, markedly heterogeneous enhancement,
and regional lymph node metastases. Radiologically, the diagnosis
suggested the possibility of malignancy. Therefore, awareness of
these radiological findings may facilitate the detection of
malignant EAML. Further studies on the imaging features of EAML
will be required in the future.
The pathogenesis and mechanisms of the malignant
transformation of EAML remain unclear. The optimal criteria for the
diagnosis of malignant EAML may require to be reassessed, since
necrosis, hemorrhage, nuclear atypia and mitotic activity are
considered to indicate a potentially malignant tumor. However,
there are no histological criteria for malignant EAML, with the
exception of distant metastases, which are accepted to be a
definite sign of malignancy. In the present case, the tumor was
demonstrated to be malignant due to the occurrence of distant
metastases. Histologically, EAML is characterized by the presence
of predominantly polygonal epithelioid cells with atypical nuclei,
mitotic figures, necrosis, marked atypical large cells with
abundant eosinophilic cytoplasm that stain strongly for HMB-45, and
low number of adipose cells (17).
Therefore, malignant EAML should be carefully differentiated from
RCC, and confirmed by pathology and immunohistochemistry.
Additionally, a previous study has indicated that Ki-67 may be a
useful marker in the diagnosis of malignant EAML (18).
Malignant EAML is aggressive and may be
life-threatening (19). Therefore,
the clinicians should be aware of it, and consider EAML as a
potential malignant disease. Currently, there is no known effective
therapy for malignant EAML other than surgery (20). Although nephron sparing surgery is an
alternative treatment for malignant renal EAML, local recurrence
and metastasis have been reported following surgery (10). Surgical removal of metastases often
contributes to good prognosis (20).
Due to the difficulty in differentiating malignant EAML from RCC,
nephrectomy is a common procedure for large EAMLs. However,
nephrectomy alone may be inadequate in certain cases, and adjuvant
therapy should be considered (21).
Chemotherapy for malignant EAML is still under
debate, although a number of patients with EAML have been reported
to respond to doxorubicin (10).
However, the efficacy of this treatment is not clear at present,
despite the fact that certain cases exhibited good response at the
beginning of the treatment. In addition the long-term effects
associated with doxorubicin have not been determined thus far. In a
recent study, Kenerson et al (22) reported an EAML mass that uniformly
exhibited activation of the mechanistic target of rapamycin (mTOR)
cascade, which suggests that mTOR inhibitors may provide a
therapeutic benefit in the treatment of EAML. Multimodal treatments
for malignant EAML, which consist of chemotherapeutic and molecular
targeted agents, have been proposed (23). However, this type of approach was not
successful in the present case, since the patient did not respond
to chemotherapy in combination with sorafenib.
Malignant EAML presents a relatively favorable
prognosis without relapse or metastasis following surgery. However,
patients with remote organ metastases, mainly in the lungs and
liver, present relatively poor prognosis, and require a closer
follow-up of these tumors.
References
|
1
|
Thway K and Fisher C: PEComa: Morphology
and genetics of a complex tumor family. Ann Diagn Pathol.
19:359–368. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Konosu-Fukaya S, Nakamura Y, Fujishima F,
et al: Renal epithelioid angiomyolipoma with malignant features:
Histological evaluation and novel immunohistochemical findings.
Pathol Int. 64:133–141. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mahdi Y, Znati K, Iken A, et al: Malignant
renal epithelioid angiomyolipoma associated with abdominopelvic
hydatid cysts: A case report. J Med Case Rep. 10:802015. View Article : Google Scholar
|
|
4
|
Huang KH, Huang CY, Chung SD, Pu YS, Shun
CT and Chen J: Malignant epithelioid angiomyolipoma of the kidney.
J Formos Med Assoc. 106(Suppl): S51–S54. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lau SK, Marchevsky AM, McKenna RJ Jr and
Luthringer DJ: Malignant monotypic epithelioid angiomyolipoma of
the retroperitoneum. Int J Surg Pathol. 11:223–228. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Svec A and Velenská Z: Renal epithelioid
angiomyolipoma - a close mimic of renal cell carcinoma. Report of a
case and review of the literature. Pathol Res Pract. 200:851–856.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lopez-Beltran A, Scarpelli M, Montironi R
and Kirkali Z: 2004 WHO classification of the renal tumors of the
adults. Eur Urol. 49:798–805. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Martignoni G, Pea M, Reghellin D, Zamboni
G and Bonetti F: PEComas: The past, the present and the future.
Virchows Arch. 452:119–132. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Aydin H, Magi-Galluzzi C, Lane BR, Sercia
L, Lopez JI, Rini BI and Zhou M: Renal angiomyolipoma:
Clinicopathologic study of 194 cases with emphasis on the
epithelioid histology and tuberous sclerosis association. Am J Surg
Pathol. 33:289–297. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cibas ES, Goss GA, Kulke MH, Demetri GD
and Fletcher CD: Malignant epithelioid angiomyolipoma (‘sarcoma ex
angiomyolipoma’) of the kidney: A case report and review of the
literature. Am J Surg Pathol. 25:121–126. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Cui L, Hu XY, Gong SC, Fang XM, Lerner A
and Zhou ZY: A massive renal epithelioid angiomyolipoma with
multiple metastatic lymph nodes. Clin Imaging. 35:320–323. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Radin R and Ma Y: Malignant epithelioid
renal angiomyolipoma in a patient with tuberous sclerosis. J Comput
Assist Tomogr. 25:873–875. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
El Jack AK, Tomaszewski JE, Haller DG and
Siegelman ES: Metastatic PEComa arising from renal angiomyolipoma:
MRI findings. J Magn Reson Imaging. 26:159–161. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Nepple KG, Bockholt NA, Dahmoush L and
Williams RD: Giant renal angiomyolipoma without fat density on CT
scan: Case report and review of the literature.
ScientificWorldJournal. 10:1334–1338. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Tsai CC, Wu WJ, Li CC, Wang CJ, Wu CH and
Wu CC: Epithelioid angiomyolipoma of the kidney mimicking renal
cell carcinoma: A clinicopathologic analysis of cases and
literature review. Kaohsiung J Med Sci. 25:133–140. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Inci O, Kaplan M, Yalcin O, Atakan IH and
Kubat H: Renal angiomyolipoma with malignant transformation,
simultaneous occurrence with malignity and other complex clinical
situations. Int Urol Nephrol. 38:417–426. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Tan G, Liu L, Qiu M, Chen L, Cao J and Liu
J: Clinicopathologic features of renal epithelioid angiomyolipoma:
Report of one case and review of literatures. Int J Clin Exp
Pathol. 8:1077–1080. 2015.PubMed/NCBI
|
|
18
|
Ooi SM, Vivian JB and Cohen RJ: The use of
the Ki-67 marker in the pathological diagnosis of the epithelioid
variant of renal angiomyolipoma. Int Urol Nephrol. 41:559–565.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Luo J, Liu B, Wang Y, Li J, Wang P, Chen J
and Wang C: Comprehensive clinical and pathological analysis of
aggressive renal epithelioid angiomyolipoma: report of three cases.
Onco Targets Ther. 27:823–827. 2014.
|
|
20
|
Vicens RA, Jensen CT, Korivi BR and
Bhosale PR: Malignant renal epithelioid angiomyolipoma with liver
metastasis after resection: a case report with multimodality
imaging and review of the literature. J Comput Assist Tomogr.
38:574–577. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Varma S, Gupta S, Talwar J, Forte F and
Dhar M: Renal epithelioid angiomyolipoma: A malignant disease. J
Nephrol. 24:18–22. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kenerson H, Folpe AL, Takayama TK and
Yeung RS: Activation of the mTOR pathway in sporadic
angiomyolipomas and other perivascular epithelioid cell neoplasms.
Hum Pathol. 38:1361–1371. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Allegra A, Coppolino G, Bolignano D,
Giacobbe MS, Alonci A, D'Angelo A, Bellomo G, Teti D, Loddo S,
Musolino C and Buemi M: Endothelial progenitor cells: Pathogenetic
role and therapeutic perspectives. J Nephrol. 22:463–475.
2009.PubMed/NCBI
|