Introduction
Angiomatous meningiomas (AMs) are rare
histopathological subtypes of meningiomas, and are most commonly
observed within the cerebral convexity (1). Microscopically, the lesions have
features of typical meningiomas, with numerous vascular channels
which predominate over their meningothelial elements (2,3). AMs also
occasionally occur in the spinal canal, and account for 1% of all
intraspinal meningiomas (2). The
majority of spinal AMs are located in the intradural-extramedullary
(IDEM) space (4,5). Compared with other IDEM tumors,
intraspinal AMs have no unique clinical symptoms (2). Instead, the diagnosis depends on
pathological examination (3).
Epithelial membrane antigen (EMA) is the most reliable immunomarker
and exhibits positive immunoreactivity in all AMs (2,3). Timely en
bloc resection is the most favorable treatment strategy and the
rate of tumor recurrence is fairly low, ranging between 0 and 60%
(2,4,5). Epidural
AMs are extremely rare. In the present study, we report the case of
an epidural AM in a 55-year-old female. The clinical manifestation,
radiological findings, treatment and outcome of the patient are
presented. Written informed consent was obtained from the patient's
family and study approval was obtained from the Institutional
Review Board of Beijing Tiantan Hospital, Beijing, China.
Case report
A 55-year-old female presented at Beijing Tiantan
Hospital, China, with a 2-year history of progressive back pain and
weakness in both legs. No sphincter dysfunction was noted.
Neurological examination revealed a paraparesis, with motor deficit
3/5 in the both legs (as classified by the Medical Research Council
grading system) (6). This finding was
associated with hypesthesia and brisk osteotendinous reflexes.
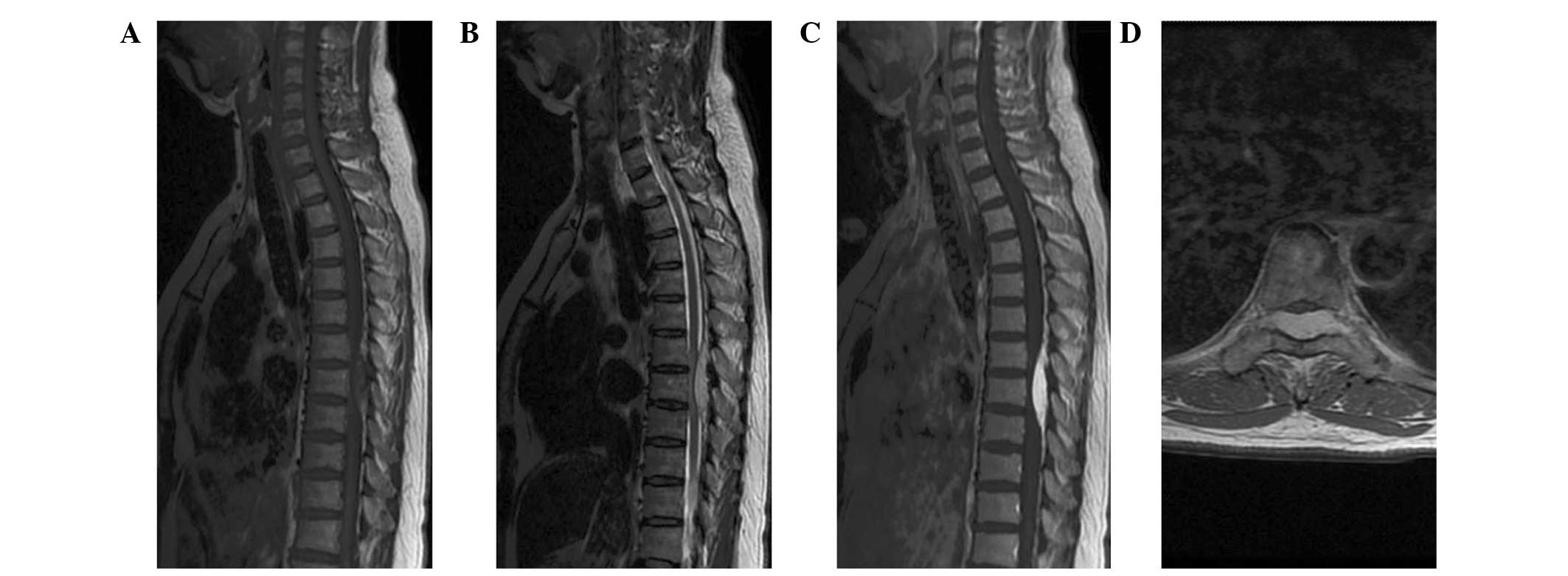
Magnetic resonance imaging (MRI) demonstrated a
well-circumscribed oval lesion in the dorsal-lateral space at T6–8
(Fig. 1). The lesion was isointense
on T1-weighted images (WI), hyperintense on T2-WI, and enhanced
homogeneously on contrast-enhanced T1-WI. The ‘dural tail sign’ was
positive. The preoperative differential diagnoses considered
included lymphoma, metastatic tumor, angiolipoma, cavernous
hemangioma, meningioma and hemangiopericytoma (HPC).
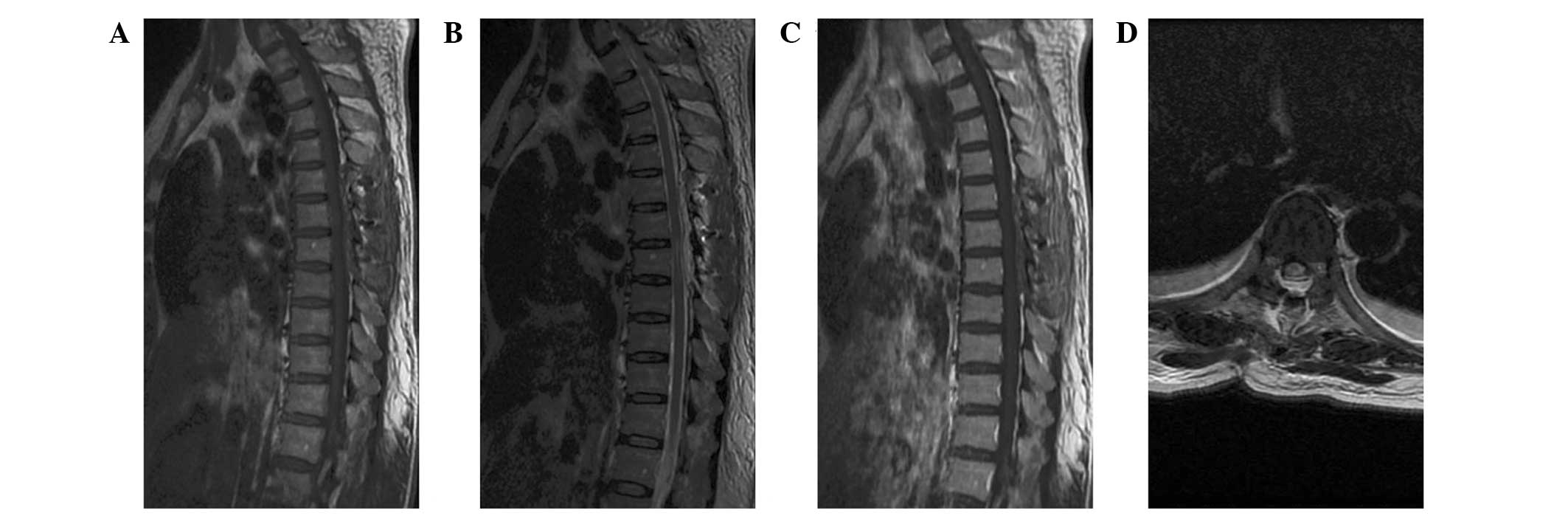
The patient underwent a T6–8 laminectomy.
Intraoperative monitoring of somatosensory and motor-evoked
potentials was performed. The lesion was well-delineated, fresh
red, vascular, and located in the epidural space. It was removed
en bloc following circumferential dissection. The dural
attachment was located dorsal-laterally and was not resected but
extensively bipolar cauterized. Postoperative MRI revealed no
residual tumor (Fig. 2).
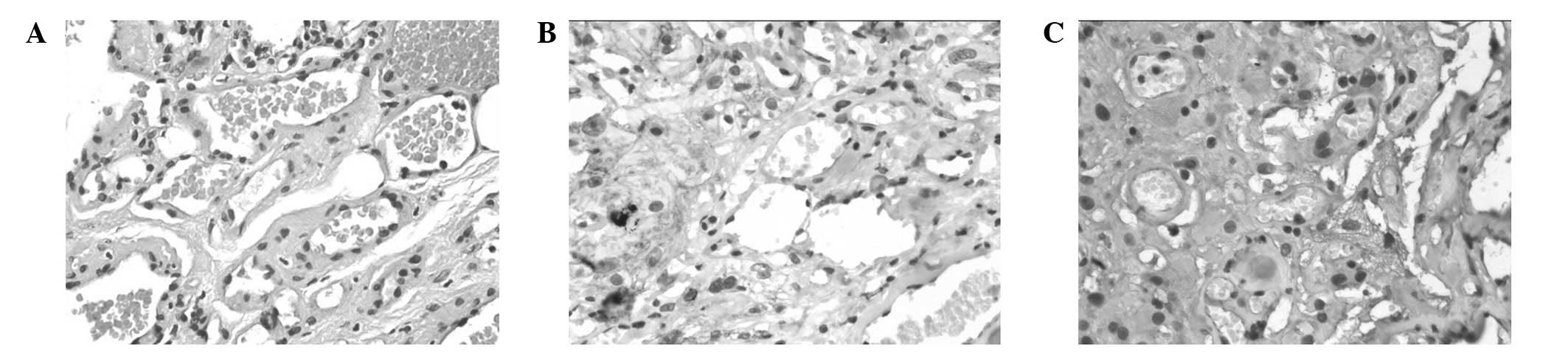
Microscopically, the tumor consisted of
meningothelial and vascular elements (Fig. 3). There was no mitotic activity or
endothelial proliferation. Immunohistochemical examination revealed
that the tumor cells were positive for EMA and vimentin.
Delayed paraplegia occurred at 4 h postoperatively.
The patient was treated with methylprednisolone and hyperbaric
oxygen, and was discharged to an in-patient rehabilitation facility
at day 14 postoperatively. Gradually, over the next six months, the
patient's bilateral leg strength improved to grade 4/5, and no
tumor recurrence was noted.
Discussion
Spinal meningiomas are mostly IDEM in location, and
the diagnosis of a tumor is usually simple, and based on
radiological findings. However, meningiomas also occasionally occur
in an epidural location. Since the publication of the earliest
study in 1963, only 50 cases of epidural meningiomas have been
described, and psammomatous types were the predominant subtype
(7–10). Epidural AMs are extremely rare. No
other examples of foraminal extension of this specific type were
identified in the literature.
The precise pathogenesis of epidural meningiomas is
still unclear. Various hypotheses have been proposed, which include
arachnoid villi isolated from the arachnoid layer which migrated
into the dura mater, vestigial remnants of the embryonal arachnoid
layer, aberrant arachnoid islets in the epidural space, and villi
from nerve roots where the dura layer is thin (7,8,11,12).
Similar to those observed with common epidural
tumors, the symptoms of our patient were progressive motor deficits
and local pain due to the effect of the mass. The clinical course
was relatively slow (24 months), which may reflect the benign
nature of epidural AMs. Unlike epidural cavernous hemangioma, which
may present with acute neurological symptoms due to their tendency
to hemorrhage (13), epidural AM does
not appear to have a propensity for acute intratumoral bleeding
despite being highly vascularized. Similarly, spontaneous
intratumoral bleeding was only observed in one intracranial AM
(2). This phenomenon argues against a
high incidence of hemorrhage in AMs.
MRI is the most reliable method for identifying
intraspinal tumors. On MRI, the epidural AM in the present case
demonstrated isointensity on T1-WI, hyperintensity on T2-WI, and
homogeneous enhancement on contrast-enhanced T1-WI. Intracranial
AMs usually exhibit notable signal voids of vessels (1); however, signal void areas were not
evident in the present case. These radiological characteristics are
nonspecific. The ‘dural tail sign’, which is useful for the
identification of IDEM meningioma, was positive in the current
case. However, this finding has also been present in metastatic
tumors and lymphoma (14,15). Thus, the differential diagnosis
includes all epidural contrast-enhancing lesions, including
lymphoma, metastatic tumor, cavernous hemangioma, angiolipoma and
HPC. An accurate diagnosis depends on the pathology. However, due
to the similar microscopic features, hematoxylin and eosin staining
may be not sufficient to differentiate AMs from HPCs. Therefore,
immunohistochemical staining is necessary. EMA is the most reliable
immuno-marker of meningiomas, whereas HPCs are negative with EMA
(16,17). In the current case, the tumor
exhibited abundant vascular components which exceeded 50% of the
total area, a lack of cytonuclear atypia or mitotic activity, and
EMA immunoreactivity. Thus, the tumor was diagnosed as AM (World
Health Organization grade I).
Since cord compression is the main pathogenic
mechanism, gross total resection (GTR) is the primary treatment of
choice for spinal lesions (18,19). Due
to the hypervascularity, piecemeal resection of AM should be
avoided (19). In the present case,
the feeding arteries were coagulated and en bloc removal was
performed. Selective spinal angiography and preoperative
embolization may exhibit feeding arteries and reduce intraoperative
bleeding (1); however, the diagnosis
still needs to be confirmed. For intracranial and intraspinal
meningiomas, tumor recurrence may be prevented by total removal of
the tumor and dural attachment (1,2). However,
if the dural attachment of intraspinal meningiomas is located
ventrally, laterally or dorsal-laterally, cauterizing the dura
takes priority over dural resection, preventing postoperative
cerebrospinal fluid leak or cord damage (4). Although the neurological function of our
patient was deteriorated following surgery, the symptoms were
improved to normal levels within six months, and no tumor
recurrence was noted. Therefore, epidural AMs are amenable to
surgery, and a positive clinical outcome following GTR (Simpson
grade I and II resection) is expected.
In conclusion, AM should be included in the
differential diagnosis of spinal epidural lesions. A definitive
diagnosis is difficult based on MRI alone due to its nonspecific
characteristics. Since AM is a histologically benign and highly
vascularized tumor, timely GTR (en bloc resection) is the
most effective treatment. A good clinical outcome may be expected
following GTR (Simpson grade I and II resection).
References
|
1
|
Liu Z, Wang C, Wang H, Wang Y, Li JY and
Liu Y: Clinical characteristics and treatment of angiomatous
meningiomas: a report of 27 cases. Int J Clin Exp Pathol.
6:695–702. 2013.PubMed/NCBI
|
|
2
|
Hasselblatt M, Nolte KW and Paulus W:
Angiomatous meningioma: a clinicopathologic study of 38 cases. Am J
Surg Pathol. 28:390–393. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Levy WJ Jr, Bay J and Dohn D: Spinal cord
meningioma. J Neurosurg. 57:804–812. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Boström A, Bürgel U, Reinacher P, Krings
T, Rohde V, Gilsbach JM and Hans FJ: A less invasive surgical
concept for the resection of spinal meningiomas. Acta Neurochir
(Wien). 150:551–556. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Nakamura M, Tsuji O, Fujiyoshi K, Hosogane
N, Watanabe K, Tsuji T, Ishii K, Toyama Y, Chiba K and Matsumoto M:
Long-term surgical outcomes of spinal meningiomas. Spine (Phila Pa
1976). 37:E617–E623. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Dyck PJ, Boes CJ, Mulder D, Millikan C,
Windebank AJ, Dyck PJ and Espinosa R: History of standard scoring,
notation and summation of neuromuscular signs. A current survey and
recommendation. J Peripher Nerv Syst. 10:158–173. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Haft H and Shenkin Ha: Spinal epidural
meningioma: Case report. J Neurosurg. 20:801–804. 1963. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fortuna A, Gambacorta D and Occhipinti EM:
Spinal extradural meningiomas. Neurochirurgia (Stuttg). 12:166–180.
1969.PubMed/NCBI
|
|
9
|
Takeuchi H, Kubota T, Sato K and Hirose S:
Cervical extradural meningioma with rapidly progressive myelopathy.
J Clin Neurosci. 13:397–400. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zevgaridis D and Thomé C: Purely epidural
spinal meningioma mimicking metastatic tumor: case report and
review of the literature. Spine (Phila Pa 1976). 27:E403–E405.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kumar S, Kaza RC, Maitra TK and Chandra M:
Extradural spinal meningioma arising from a nerve root: case
report. J Neurosurg. 52:728–729. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sato N and Sze G: Extradural spinal
meningioma: MRI. Neuroradiology. 39:450–452. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sarikaya-Seiwert S, Gierga K, Wessalowski
R, Steiger HJ and Hänggi D: Solitary spinal epidural cavernous
angiomas in children presenting with acute neurological symptoms
caused by hemorrhage. J Neurosurg Pediatr. 5:89–93. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Rokni-Yazdi H and Sotoudeh H: Prevalence
of ‘dural tail sign’ in patients with different intracranial
pathologies. Eur J Radiol. 60:42–45. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Tien RD, Yang PJ and Chu PK: ‘Dural tail
sign’: a specific MR sign for meningioma? J Comput Assist Tomogr.
15:64–66. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Rao S, Rajkumar A and Kuruvilla S:
Angiomatous meningioma: a diagnostic dilemma. Indian J Pathol
Microbiol. 51:53–55. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
D'Amore ES, Manivel JC and Sung JH:
Soft-tissue and meningeal hemangiopericytomas: an
immunohistochemical and ultrastructural study. Hum Pathol.
21:414–423. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Orchowski J, Bridwell KH and Lenke LG:
Neurological deficit from a purely vascular etiology after
unilateral vessel ligation during anterior thoracolumbar fusion of
the spine. Spine (Phila Pa 1976). 30:406–410. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wu L, Yang T, Yang C, Deng X, Fang J and
Xu Y: Surgical treatment of intraspinal angiomatous meningiomas
from a single center. Neurol Med Chir (Tokyo). 55:328–335. 2015.
View Article : Google Scholar : PubMed/NCBI
|