Introduction
CyberKnife® (Accuray Inc., Sunnyvale, CA, USA)
stereotactic body radiotherapy (SBRT) (1–4), an
image-guided robotic radiosurgery system, is a radiation delivery
platform that is capable of detecting and correcting for
intrafraction tumor motion, as well as being able to adapt to the
patients breathing pattern and moving the linear accelerator in
concert (1). CyberKnife was developed
in the United States in 1992 (2),
applied clinically in 1994 and introduced in Japan in 1997.
CyberKnife can be used to perform multi-directional irradiation and
disperse the dose among the normal tissues due to a high degree of
freedom for the direction of the irradiation. Therefore,
irradiation by CyberKnife treatment is more intensive than SBRT by
conventional linac (5).
The therapeutic indications of CyberKnife previously
included brain tumors, and head and neck cancer (3). However, therapeutic application against
cancer in the trunk, including hepatocellular carcinoma (HCC), was
begun following approval in June 2008 (4). Cancer in the trunk moves with
respiration. However, CyberKnife detects minute body movements and
fine-tunes the irradiation angle using a seeker (6). The technique is therefore expected to
become a novel local treatment for HCC due to its minimal
invasiveness and the reduced impact on patients (7–9).
CyberKnife treatment of HCC was introduced into
Saiseikai Yokohamashi Tobu Hospital (Yokohama, Japan) in December
2011, and dynamic CT has mainly been used to determine its
therapeutic effect. However, this technique could take ≥6 months to
observe a marked effect in a number of the affected patients.
Therefore, it is expected that the establishment of a method that
will allow the early determination of the effectiveness of
treatment will improve the response.
We previously performed hemodynamic diagnoses of HCC
and liver metastases, and evaluated the early responses to
sorafenib for HCC using contrast-enhanced ultrasonography (CEUS)
with Sonazoid, and confirmed their usefulness (10,11). In
the present study, CEUS was performed prior to and following
CyberKnife treatment, and the changes in the images were evaluated
to investigate whether CEUS can be applied therapeutically for the
early determination of the effect of CyberKnife treatment.
Materials and methods
Indications of CyberKnife
In Saiseikai Yokohamashi Tobu Hospital, CyberKnife
is applied to treat HCC patients with a performance status of ≤2, a
Child-Pugh score of A to 8-B, a total bilirubin level of ≤3 mg/dl,
an indocyanine green retention rate at 15 min of ≤50%, no ascites,
≤3 tumors with a tumor diameter of ≤3 cm, a single tumor with a
tumor diameter of ≤5 cm, tumors ≥1 cm away from the intestine, and
tumors with no connection to the gallbladder.
CyberKnife methodology
Since CyberKnife treatment of cancer in the trunk,
including HCC, cannot be performed using the skeleton as the focal
point, i.e., the skull in head and neck cancer, a gold fiducial
marker (Toyo Medic Co., Tokyo, Japan) was installed prior to
treatment as an ultrasound-guided target for percutaneous
transhepatic radiation. The gold fiducial marker is a coiled device
(0.75 mm in diameter by 5 mm in length) that is implanted around
the lesions. If a lesion was detected in the right or left lobe of
the liver, the marker could then be implanted in the right or left
lobe. The irradiation treatment plan was formed by CT following
implantation of the target. The initial total irradiation dose was
60 Gy and the dose was increased or decreased based upon the tumor
size, location and residual liver function, as required.
Irradiation was divided into 3–5 fractions. The irradiation range
of the hepatic parenchyma surrounding the tumors was ≥17 Gy and the
irradiated site was ≤20% of the whole liver.
Patients
The subjects consisted of 4 patients with HCC (4
lesions) who met the aforementioned criteria for treatment,
underwent CyberKnife treatment and were evaluated by image analysis
using CEUS prior to and following treatment. In all cases, the
therapeutic effects were confirmed by dynamic CT following
treatment. The patients consisted of 3 males and 1 female, with a
mean age of 78.3 years. The underlying liver diseases were
hepatitis C in 3 patients and alcoholic hepatitis in 1 patient.
Child-Pugh liver function was class A in all subjects. Primary
lesions were detected in 2 patients, while distant recurrences were
detected in the others. HCC was diagnosed as classical HCC or
distant recurrence by CEUS, dynamic CT and gadolinium ethoxybenzyl
diethylenetriamine pentaacetic acid-magnetic resonance imaging
(MRI). Informed consent was obtained from all patients for
inclusion in this study.
CEUS methodology
CEUS was performed prior to treatment, at 2 and 4
weeks post-CyberKnife treatment, and every 4 weeks thereafter for
as long as possible. Evaluation by CEUS was completed if the
therapeutic effect was confirmed by dynamic CT. The ultrasound
equipment used in this examination was an SSA-790A (Toshiba Medical
Systems, Tokyo, Japan) with a convex probe (PVT-375BT; 3.75-MHz
center frequency). The imaging mode used was wide-band harmonic
imaging (pulse subtraction) with transmission/reception frequencies
of 1.8 and 3.5 MHz, respectively. The mechanical index for acoustic
output was set to 0.2 and the dynamic range was set to 60–65 dB. A
single focal point was set at the deep site of the lesion, and an
intravenous bolus injection of Sonazoid (0.5 ml; Daiichi Sankyo,
Tokyo, Japan) was administered via a left cubital venous line
followed by flushing with 10 ml of normal saline. Following
injection of Sonazoid, the lesion was evaluated with regard to the
following: The dynamics of the enhancement of the tumor and the
hepatic parenchyma surrounding the tumor in the vascular phase
(0–40 sec), and the presence or absence of a hypoechoic area in the
hepatic parenchyma surrounding the tumor in the post-vascular phase
(after 10 min). Subsequently, the dynamics of the enhancement of
the tumor and the hepatic parenchyma surrounding the tumor were
re-evaluated using the re-injection method (12) with Sonazoid in the post-vascular
phase. Digital cine clips of the CEUS images were stored on the
hard disk of the scanner and transferred to a high-performance
personal computer for subsequent analysis. This study was approved
by the Ethical Review Board of Toho University Medical Center,
Omori Hospital.
Results
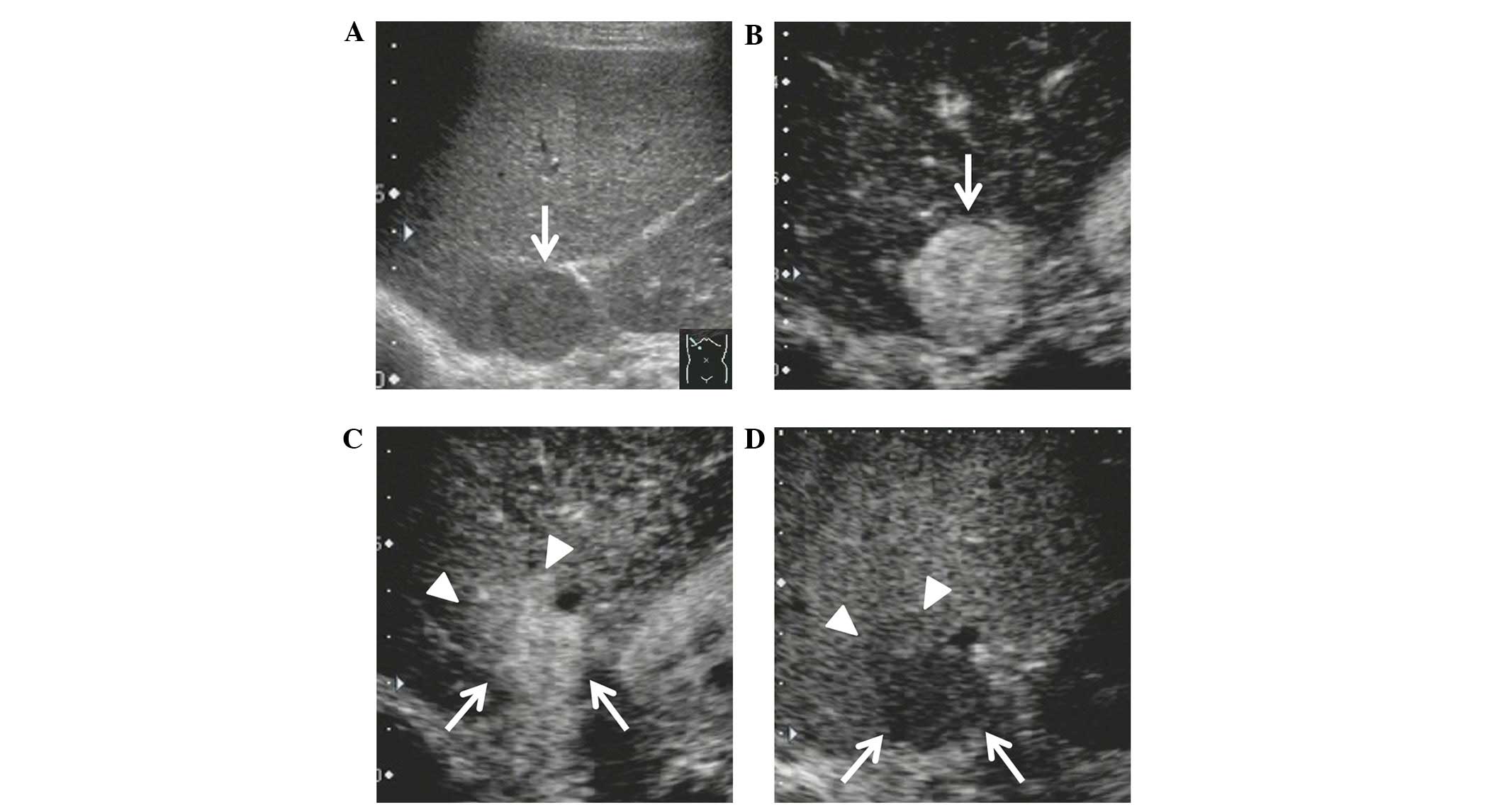
All HCC lesions showed hyperenhancement by CEUS
prior to treatment (Table I). In case
1, the tumor showed hypoenhancement at 40 weeks post-treatment.
Strong hyperenhancement was observed in the hepatic parenchyma
surrounding the tumor in the vascular phase at 12 weeks
post-treatment and a hypoechoic area was observed in the
post-vascular phase at 20 weeks post-treatment (Fig. 1). In case 2, the tumor showed
hypoenhancement at 8 weeks post-treatment. Strong hyperenhancement
was observed in the hepatic parenchyma surrounding the tumor in the
vascular phase at 12 weeks post-treatment and a hypoechoic area was
observed in the post-vascular phase at 16 weeks post-treatment. In
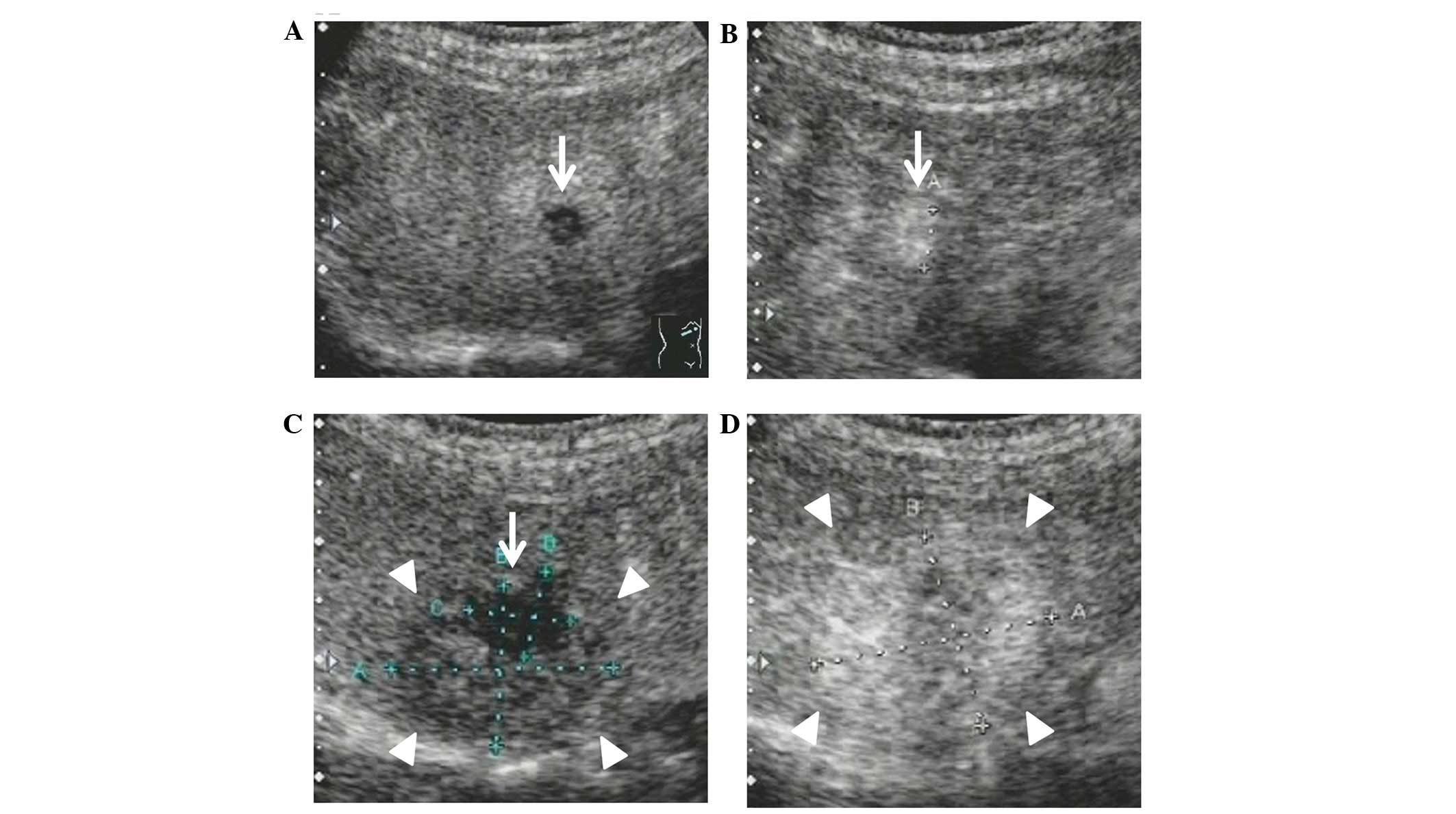
case 3, the tumor showed hypoenhancement at 4 weeks post-treatment
(Fig. 2). Strong hyperenhancement was
observed in the hepatic parenchyma surrounding the tumor in the
vascular phase at 2 weeks post-treatment and a hypoechoic area was
observed in the post-vascular phase at 4 weeks post-treatment. In
case 4, the tumor showed hypoenhancement at 12 weeks
post-treatment. Strong hyperenhancement was observed in the hepatic
parenchyma surrounding the tumor in the vascular phase at 8 weeks
post-treatment and a hypoechoic area was observed in the
post-vascular phase at 8 weeks post-treatment.
 | Table I.Characteristics of patients, and the
changes in the hemodynamics of the tumor and the hepatic parenchyma
surrounding the tumor, as observed by CEUS. |
Table I.
Characteristics of patients, and the
changes in the hemodynamics of the tumor and the hepatic parenchyma
surrounding the tumor, as observed by CEUS.
|
|
|
|
|
|
|
| Hepatic parenchyma
surrounding the tumor |
|---|
|
|
|
|
|
|
|
|
|
|---|
| Case | Etiology | Child-Pugh
classification | Area | Diameter, mm | Amount of radiation,
Gy | Week of tumor
hypoenhancementa | Week of
hyperenhancementb | Week of hypoechoic
areac |
|---|
| 1 | HCV | 5-A | S6 | 24 | 50 | 40 | 12 | 20 |
| 2 | HCV | 6-A | S8 | 37 | 36 | 8 | 12 | 16 |
| 3 | Alcohol | 5-A | S8 | 12 | 54 | 4 | 2 | 4 |
| 4 | HCV | 5-A | S3 | 25 | 54 | 12 | 8 | 8 |
The results can be summarized as follows: i) In the
patient with earlier changes, hemodynamic changes were evident in
the tumor at 4 weeks and in the hepatic parenchyma surrounding the
tumor at 2 weeks post-treatment, respectively; ii) the tumor showed
hypoenhancement in all patients; and iii) with regard to findings
in the hepatic parenchyma surrounding the tumor, strong
hyperenhancement appeared in the vascular phase initially, followed
by a hypoechoic area in the post-vascular phase.
Discussion
We previously evaluated intratumoral hemodynamics
during progression along the multistep pathway of HCC (13) and early responses to sorafenib for HCC
using CEUS with Sonazoid. It was confirmed that CEUS with Sonazoid
was less invasive compared with dynamic CT, due to the lack of
iodine allergy, exposure to radiation and influence of renal
function by administration of the contrast agent. Furthermore, a
detailed evaluation, based on the observation of real-time
hemodynamics following injection of Sonazoid, was provided. In
addition, CEUS was useful for determining the early responses to
sorafenib for HCC (11,14).
CyberKnife is expected to be a novel local treatment
for HCC, however, it takes a long-term follow-up to determine the
effect of treatment in a number of the affected patients when using
dynamic CT and MRI (15). Therefore,
there is a requirement to evaluate procedures for early
determination of the effect of CyberKnife treatment. The
hemodynamics of liver metastases and hepatic parenchyma surrounding
the tumors in SBRT have been reported on CEUS with SonoView
(Bracco, Milan, Italy) (16).
However, there has been no report of the use of CEUS with Sonazoid
to examine the hemodynamics during and following CyberKnife
treatment for HCC. In the present study, CEUS with Sonazoid was
performed prior to and following CyberKnife treatment for HCC
patients, and the therapeutic applicability of CEUS with Sonazoid
was evaluated for the early determination of the effect of
CyberKnife treatment.
Although the appearance of the hemodynamic changes
in the tumor and the hepatic parenchyma surrounding the tumor
varied depending on the patient in this study, in the patient with
earlier changes, the hemodynamic changes were evident in the tumor
at 4 weeks and in the hepatic parenchyma surrounding the tumor at 2
weeks post-treatment, respectively. These differences in the timing
of the appearance in hemodynamic changes following treatment
between patients were affected by the differences in the tumor size
and site, the total irradiation dose and the liver function.
The tumors showed hypoenhancement in all patients,
despite differences in the timing of their appearance. In HCC after
radiotherapy, contrast enhancement is considered to persist for a
relatively long period. By contrast, it has been reported that
perfusion in the tumor correlates with tumor vitality and
vascularization (17). Changes in
tumor vascularization during or following treatment may be
prognostic factors, and reduction of tumor vascularization was
considered to indicate a therapeutic effect.
With regard to the findings in the hepatic
parenchyma surrounding the tumor, strong hyperenhancement appeared
initially in the vascular phase, followed by hypoechoic areas in
the post-vascular phase of each patient in the present study. These
findings are considered to indicate radiation-induced liver
disease, based upon the findings in the study by Reed and Cox
(18). This study examined
histological changes in radiation-induced liver disease and
confirmed the association with the histological changes of
veno-occlusive disease, suggesting that the cause was vascular
endothelial dysfunction caused by the irradiation (18). The hepatic vein, distinct from the
hepatic artery and the portal vein, may be likely to exhibit damage
in the vascular endothelium due to the absence of Glisson's
capsule, resulting in congestion of the hepatic parenchyma and
damage to the hepatic vein. Consequently, an arterio-portal shunt
occurred, which was observed as strong hyperenhancement in this
study. Furthermore, damaged Kupffer cells induced dysfunction,
which likely appeared as hypoechoic areas in the area that showed
strong hyperenhancement during the post-vascular phase (18).
Radiation-induced liver disease is generally
considered to develop at 4–8 weeks post-treatment (19). On the other hand, CT images, which are
most frequently used for the evaluation of radiation-induced liver
disease, have shown that the median timing for the confirmation of
radiation liver disorder is 3 months (15). In the present study and a previous
study of liver metastases using CEUS with SonoView (16), changes of hemodynamics in the hepatic
parenchyma surrounding the tumor were detected comparatively
earlier than those on CT images. The reason was that CEUS was
sensitive to the evaluation of hemodynamics and was less invasive.
Therefore, frequent testing with CEUS can demonstrate earlier
changes after treatment.
It would be premature to conclude that all the
hemodynamic changes in the hepatic parenchyma surrounding the tumor
after CyberKnife treatment reflect the therapeutic effect against
HCC due to of the small scale of the present study. However, the
strong hyperenhancement observed in the hepatic parenchyma
surrounding the tumor may correspond with the irradiation field.
Therefore, if these findings are detected early after treatment,
the tumor may be irradiated sufficiently. It has been suggested
that CEUS may be applicable to the early determination of the
therapeutic effect of CyberKnife treatment in combination with the
evaluation of intratumoral vascularization. Further investigations
should be conducted in large-scale studies to support this
hypothesis.
In conclusion, evaluation of the hemodynamics of
tumors and the hepatic parenchyma surrounding the tumor using CEUS
with Sonazoid may be therapeutically applicable, as it is less
invasive and provides an early evaluation of the effectiveness of
CyberKnife treatment.
Acknowledgements
The authors wish to thank medical technologists Mr.
Takehide Kudo and Mr. Kenichi Maruyama of the Department of
Clinical Functional Physiology, Toho University Medical Center,
Omori Hospital.
References
|
1
|
Ernst F, Schlaefer A and Schweikard A:
Smoothing of respiratory motion traces for motion-compensated
radiotherapy. Med Phys. 37:282–294. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Martin A and Gaya A: Stereotactic body
radiotherapy: A review. Clin Oncol (R Coll Radiol). 22:157–172.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Adler JR Jr, Chang SD, Murphy MJ, Doty J,
Geis P and Hancock SL: The Cyberknife: A frameless robotic system
for radiosurgery. Stereotact Funct Neurosurg. 69:124–128. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Louis C, Dewas S, Mirabel X, Lacornerie T,
Adenis A, Bonodeau F and Lartigau E: Stereotactic radiotherapy of
hepatocellular carcinoma: Preliminary results. Technol Cancer Res
Treat. 9:479–487. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Yuan ZY, Meng MB, Liu CL, et al:
Stereotactic body radiation therapy using the CyberKnife® system
for patients with liver metastases. Onco Targets Ther. 7:915–923.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Dewas S, Bibault JE, Mirabel X, et al:
Prognostic factors affecting local control of hepatic tumors
treated by stereotactic body radiation therapy. Radiat Oncol.
7:1662012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yuan Z, Tian L, Wang P, Song Y, Dong Y and
Zhuang H: Comparative research on the efficacy of CyberKnife® and
surgical excision for Stage I hepatocellular carcinoma. Onco
Targets Ther. 6:1527–1532. 2013.PubMed/NCBI
|
|
8
|
Bibault JE, Dewas S, Vautravers-Dewas C,
Hollebecque A, Jarraya H, Lacornerie T, Lartigau E and Mirabel X:
Stereotactic body radiation therapy for hepatocellular carcinoma:
Prognostic factors of local control, overall survival, and
toxicity. PLoS One. 8:e774722013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Que JY, Lin LC, Lin KL, Lin CH, Lin YW and
Yang CC: The efficacy of stereotactic body radiation therapy on
huge hepatocellular carcinoma unsuitable for other local
modalities. Radiat Oncol. 9:1202014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Watanabe M, Shiozawa K, Takahashi M, Wakui
N, Otsuka Y, Kaneko H, Tanikawa K, Shibuya K, Kamiyama N and Sumino
Y: Parametric imaging using contrast-enhanced ultrasound with
Sonazoid for hepatocellular carcinoma. J Med Ultrason (2001).
37:81–86. 2010. View Article : Google Scholar
|
|
11
|
Shiozawa K, Watanabe M, Kikuchi Y, Kudo T,
Maruyama K and Sumino Y: Evaluation of sorafenib for hepatocellular
carcinoma by contrast-enhanced ultrasonography: A pilot study.
World J Gastroenterol. 18:5753–5758. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kudo M: Hepatocellular carcinoma 2009 and
beyond: From the surveillance to molecular targeted therapy.
Oncology. 75:1–12. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Matsui O, Kadoya M, Kameyama T, Yoshikawa
J, Takashima T, Nakanuma Y, Unoura M, Kobayashi K, Izumi R and Ida
M: Benign and malignant nodules in cirrhotic livers: Distinction
based on blood supply. Radiology. 178:493–497. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Shiozawa K, Watanabe M and Sumino Y:
Evaluation of the hemodynamic status of focal hepatic lesions 20 mm
or less in diameter by contrast-enhanced ultrasonography using
Sonazoid. Intervirology. 52:213–222. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sanuki-Fujimoto N, Takeda A, Ohashi T,
Kunieda E, Iwabuchi S, Takatsuka K, Koike N and Shigematsu N: CT
evaluations of focal liver reactions following stereotactic body
radiotherapy for small hepatocellular carcinoma with cirrhosis:
Relationship between imaging appearance and baseline liver
function. Br J Radiol. 83:1063–1071. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Krix M, Plathow C, Essig M, Herfarth K,
Debus J, Kauczor HU and Delorme S: Monitoring of liver metastases
after stereotactic radiotherapy using low-MI contrast-enhanced
ultrasound - initial results. Eur Radiol. 15:677–684. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Weidner N, Semple JP, Welch WR and Folkman
J: Tumor angiogenesis and metastasis-correlation in invasive breast
carcinoma. N Engl J Med. 324:1–8. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Reed GB Jr and Cox AJ Jr: The human liver
after radiation injury. A form of veno-occlusive disease. Am J
Pathol. 48:597–611. 1966.PubMed/NCBI
|
|
19
|
Lawrence TS, Robertson JM, Anscher MS,
Jirtle RL, Ensminger WD and Fajardo LF: Hepatic toxicity resulting
from cancer treatment. Int J Radiat Oncol Biol Phys. 31:1237–1248.
1995. View Article : Google Scholar : PubMed/NCBI
|