Introduction
Platelet-derived growth factor receptors (PDGFRs),
which are part of the class III receptor tyrosine kinase family,
exert stimulatory effects on c-Kit, Fms-like tyrosine kinase 3 and
macrophage colony-stimulating factor receptors (1). PDGFRs consist of an extracellular
ligand-binding region, a transmembrane domain and an intracellular
kinase domain (2). Ligand binding
induces dimerization and autophosphorylation of the receptor,
facilitating binding and activation of various cytoplasmic signal
transduction molecules (3). In this
way, multiple signaling pathways are initiated, resulting in cell
proliferation (4).
Myeloid tumors possessing PDGFRβ gene rearrangement
are a rare hematological malignancy, which present with typical
characteristics, including myeloid proliferation disorders and
eosinophilia. Chronic myelomonocytic leukemia (CMML) is a poorly
defined, heterogeneous clinicopathological syndrome that exhibits
myelodysplastic and myeloproliferative features (5), and there are no specific therapeutic
strategies for treating patients with CMML. According to laboratory
and ancillary tests, cytogenetic abnormalities occur in ~30% of
CMML patients, however, there are no consistently recurring
chromosomal translocations that can be depended upon for diagnostic
criteria, and the incidence of chromosomal translocation in CMML
patients is only 1–2% (6).
To determine the role of PDGFRβ gene rearrangement
in the pathogenesis of CMML, the current study reports a case of
CMML associated with a t(5;14)(q33;q32) fusion gene using
fluorescence in situ hybridization (FISH) and reverse
transcription-polymerase chain reaction (RT-PCR). The patient was
effectively treated with imatinib, and the relevant literature was
reviewed.
Case report
Patient
A patient with CMML was diagnosed, using
immunophenotyping and morphological methods, according to the World
Health Organization (WHO) classification of tumors of hematopoietic
and lymphoid tissues (7).
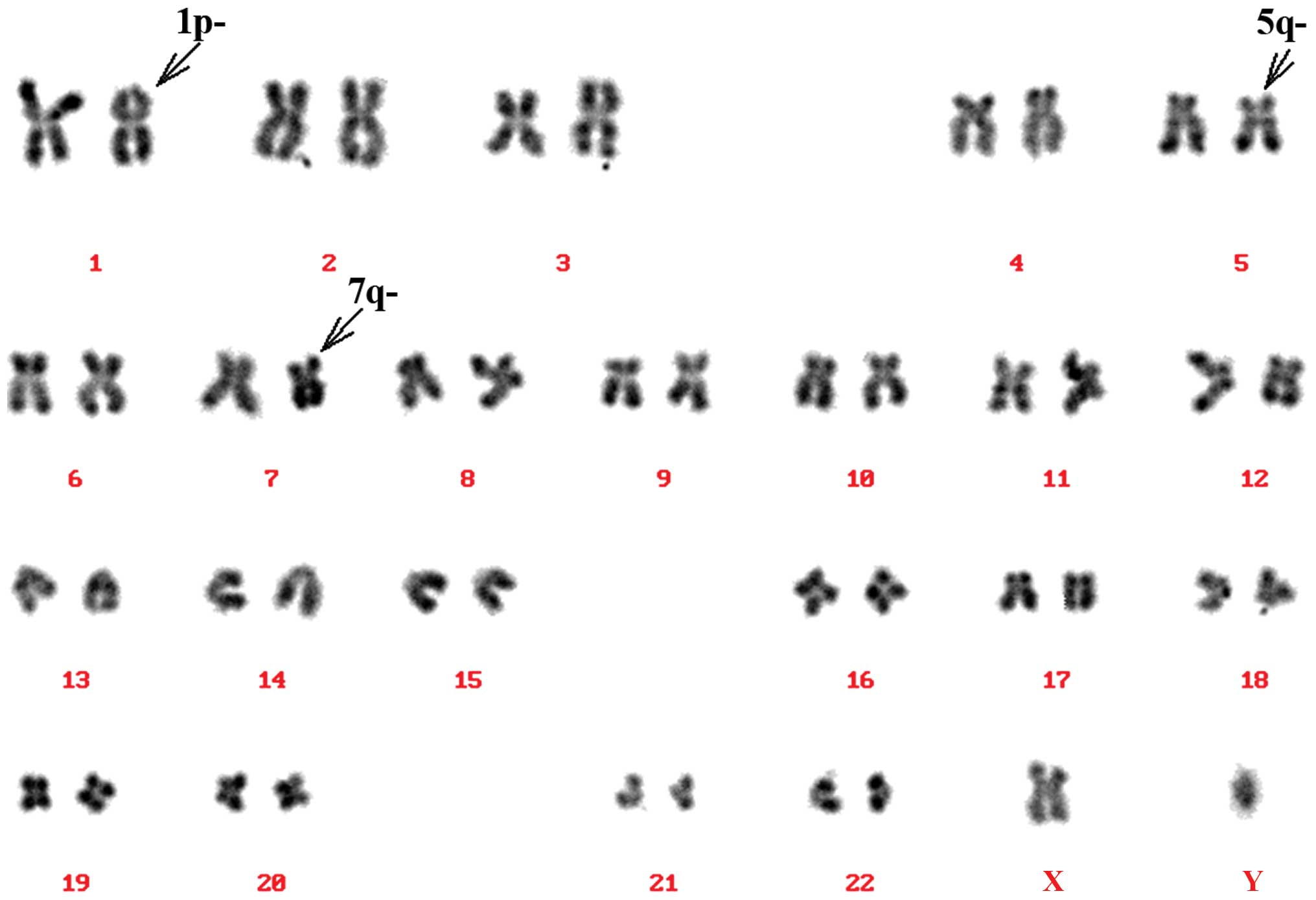
Routine karyotype analysis
A bone marrow sample was collected from the patient
(heparin lithium was used as an anticoagulant), and cultured in
Dulbecco's modified Eagle's medium with 20% fetal bovine serum
using the direct and short-term culture methods (8). Termination of culture was performed
following culturing in colchamine for 1 h, and cells were
subsequently fixed in a solution of methanol and glacial acetic
acid (methanol:glacial acetic acid, 3:1). Following fixing, cells
were collected and chromosome karyotype was analyzed after
conventional reverse-banding (9). The
remaining cells were stored in fresh fixative and preserved at
20°C. Chromosomes were analyzed according to standard procedures
(10) and the karyotype was
classified according to ‘An International System for Human
Cytogenetic Nomenclature (ISCN 2009)’ (11). The results of karyotype analysis
revealed a break in chromosome 5 (Fig.
1).
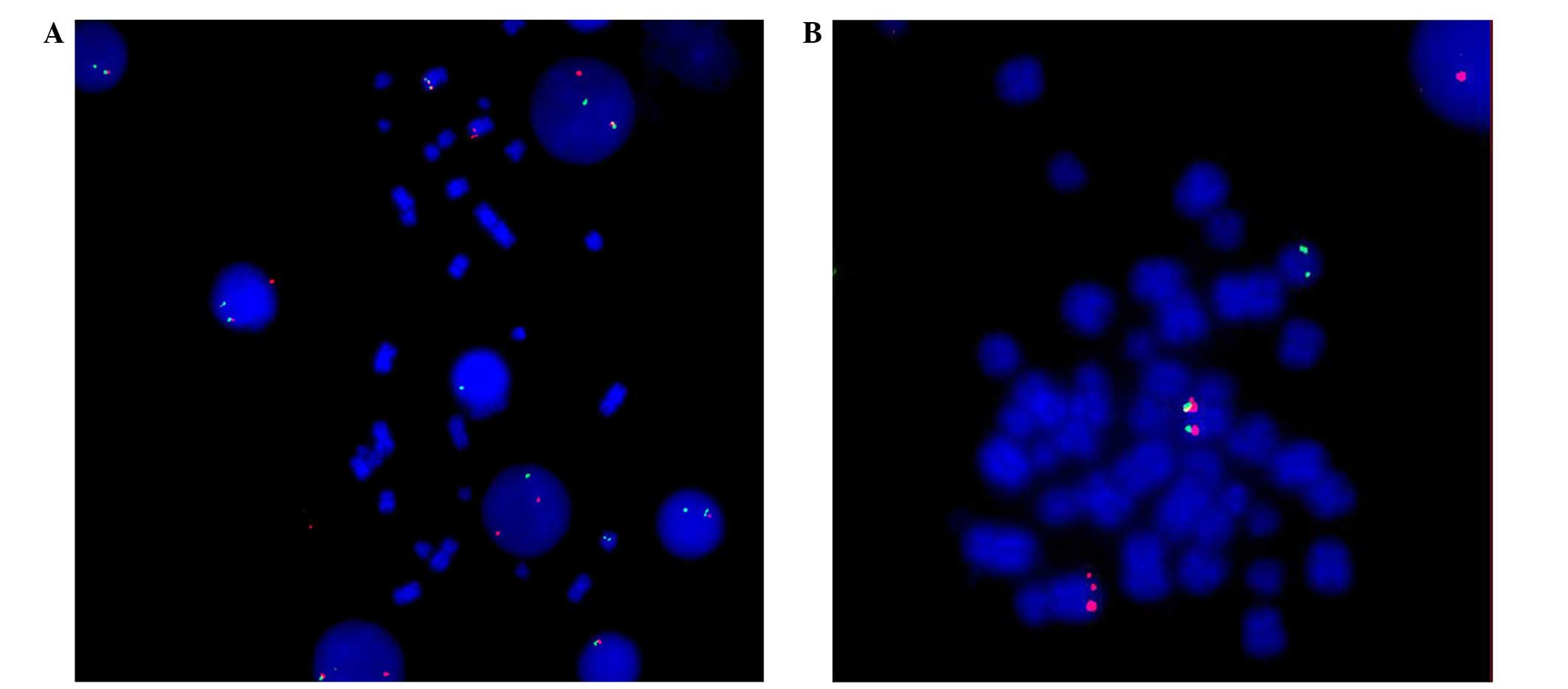
FISH
PDGFRβ isolate probe (Cytocell, Cambridge, UK),
which was complementary to the PDGFRβ gene, was applied to the
cells, and tagged with green and orange spectroscopy tags. The
methods used were previously described by Guo et al
(12). Positive abnormal signals,
including red and green fluorescence, were detected via FISH. This
indicated PDGFRβ gene rearrangement of cells during interphase
(Fig. 2A). Fig. 2B indicates the gene isolation signals,
which were located on chromosomes 5 and 14.
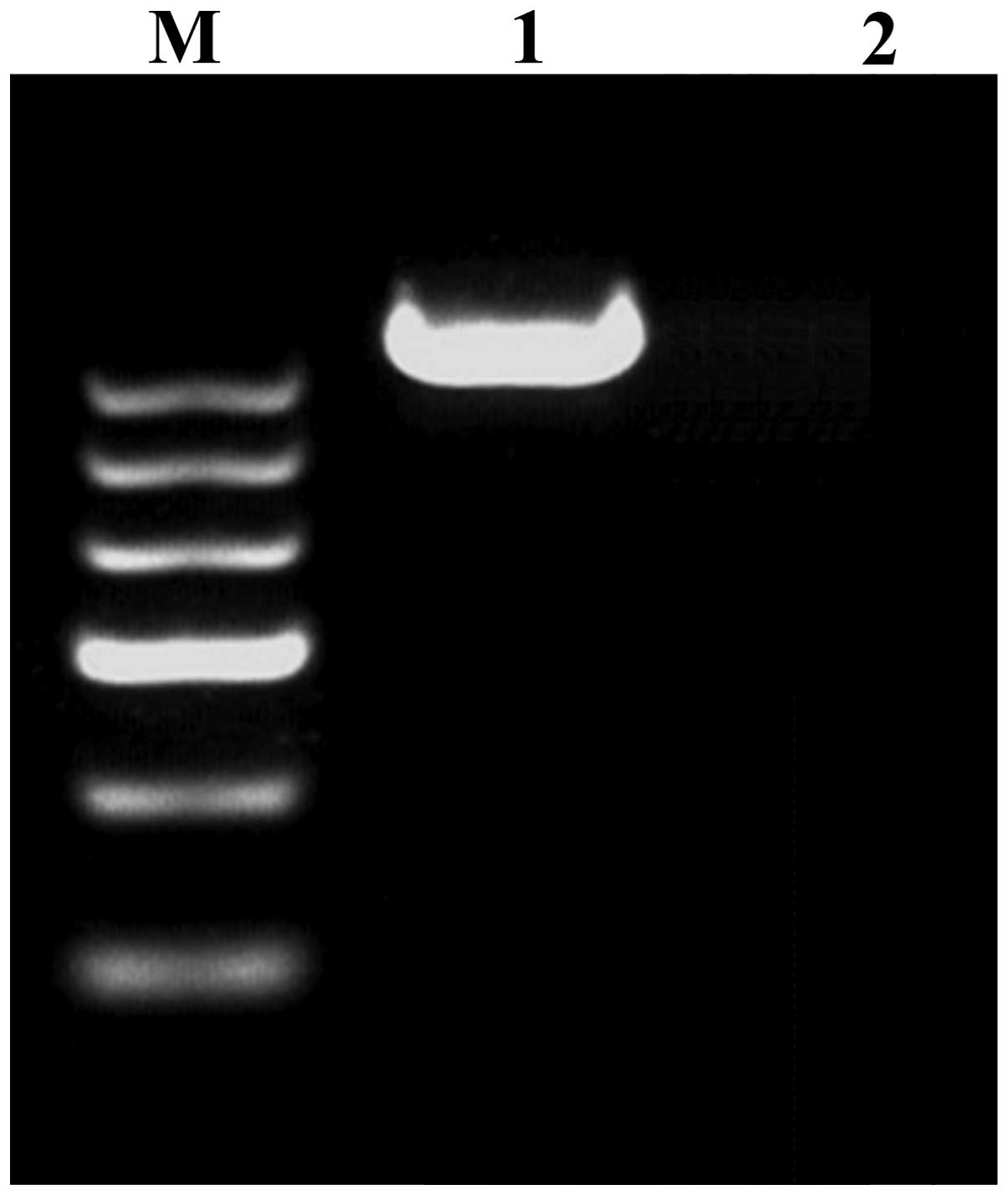
RT-PCR processing
The thyroid hormone receptor interactor 11
(CEV14)-PDGFRβ fusion gene was amplified via PCR, following the
protocol described by Huang et al (13). Samples were then analyzed for the
presence of the fusion gene product. Briefly, total RNA (1 µg) was
extracted using Trizol reagent (Invitrogen; Thermo Fisher
Scientific, Waltham, MA, USA). Complementary DNA (cDNA; 1 µl) was
synthesized using the Takara RNA PCR kit (Takara Bio, Inc., Otsu,
Japan) according to the manufacturer's instructions. According to
the reported translocated genes on chromosome 14, CEV14 (14q32)
(14), coiled-coil domain containing
88C (KIAA1509) (14q32) (15) and
ninein (GSK3B interacting protein) (NIN) (14q24) (16) primers were selected and designed. The
primers utilized were as follows: PDGFRβ forward,
5′-GTGGTGAGCACACTGCGTCTG-3′ and reverse,
5′-GTAACGTGGCTTCTTCTGCCA-3′; CEV14 forward,
5′-CGCTGCAGCTTTCTGTCTCTCAGGAACAAG-3′ and reverse,
5′-GCGAGGAGCCAAACGGATTTACATCTGTAA-3′; KIAA1509 forward,
5′-CTTATTTGGGATGGAGCCCT-3′ and reverse, 5′-CCGGGACACAGATAAGA-3′;
NIN forward, 5′-TACCAAGAACAGCATTCACCAGGCG-3′ and reverse,
5′-GCGGCAGTGCAGGGTACTACAAGAC-3′. The PCR cycling conditions used
was as follows: 30 cycles of 94°C for 1 min, 45°C for 1 min and
72°C for 1 min. PCR products were electrophoresed on 2% agarose
gels and stained with ethidium bromide. As indicated in Fig. 3, the CEV14-PDGFRβ fusion gene was
detected using RT-PCR.
Bone marrow morphology and
immunophenotyping
A bone marrow smear revealed serious granulopoiesis,
monocytosis, accompanying myelodysplasia and an increase in bone
marrow blast cell and promonocyte numbers. Hemogram analysis
revealed increased monocytic hyperplasia, progranulocytes and
promonocytes. Immunophenotyping results confirmed the diagnosis of
chronic myelomonocytic leukemia.
Discussion
The WHO classification of tumors of hematopoietic
and lymphoid tissues (2008) defined a novel category for myeloid
and lymphoid neoplasms associated with eosinophilia and
abnormalities of PDGFRα, PDGFRβ or fibroblast growth receptor 1
(17).
Myelodysplastic/myeloproliferative neoplasms (MDS/MPN),
characterized by dyshematopoiesis and myeloproliferation, may be
classified into several types: CMML, atypical chronic myelogenous
leukemia, juvenile myelomonocytic leukemia and
MDS/MPN-unclassifiable (18). MDS/MPN
occurs primarily in adult men with normal chromosome karyotypes,
and the underlying pathogenesis remains to be fully elucidated
(6).
Myeloid neoplasms associated with rearrangement of
PDGFRβ, demonstrate a PDGFRβ fusion gene on chromosome 5q31–33, and
are characterized by fever, weakness, hepatosplenomegaly and, in
certain cases, cardiac damage and skin infiltration (19). This type of neoplasm possesses a
variety of hematological symptoms, including eosinophilia,
monocytosis and characteristics of systemic mastocytosis, for
example bone marrow mastocytosis and abnormal expression of cluster
of differentiation 25 (17).
The most common chromosome translocation that
accompanies PDGFRβ gene rearrangement is t(5;12)(q33;p13) (20). Golub et al (21) confirmed that the juxtaposition of the
PDGFRβ gene on chromosome 5 and the ets variant 6 (TEL) gene on the
short arm of chromosome 12, which formed the TEL-PDGFRβ fusion
gene, sequentially activated the PDGFRβ tyrosine kinase. This
enhanced cell proliferation and inhibited apoptosis, thus
generating tumor deterioration and metastasis, through the
activation of multiple signaling pathways, ultimately leading to
the formation of a myeloproliferative disorder (22). The t(5;14) chromosome translocation
detected in the present study is rare and, to the best of our
knowledge, has been reported in the relevant literature <10
times (14,23–31). The
t(5;14) chromosome translocation has been observed to typically be
present in T-cell acute lymphoblastic leukemia (T-ALL) (24,26). The
partner genes of PDGFRβ include human homeobox 11-like 2 (Hox11L2)
(23,24,28–30) and
CEV14 (14,31). Previous studies have revealed that the
translocation of chromosomes 5 and 14 is associated with
transcriptional activation of the Hox11L2 gene (24), as well as genetic recombination of RAN
binding protein 17-T-cell leukemia, homeobox protein 3 and B-cell
lymphoma 11B (26). In the relevant
literature, CEV14-PDGFRβ fusion gene on t(5;14)(q33;q32) has been
identified in two reported cases: One T-ALL (31) and one acute myeloid leukemia case
(14). The latter of these cases
demonstrated that CEV14-PDGFRβ was capable of accelerating the
formation of leukemia, and thus may be a direct cause of cancer
formation (14). Furthermore, the
presence of the CEV14-PDGFRβ fusion gene in T-ALL was concluded to
be associated with a high rate of relapse (31). To the best of our knowledge, the
present study is the first to report a case of CMML associated with
t(5;14)(q33;q32), and further studies may be required in order to
investigate the association between the chromosome translocation
and an increased recurrence rate of CMML.
Myeloid tumors associated with PDGFRβ gene
rearrangement have been a significant research focus, due to their
susceptibility to drug therapy and high rate of complete remission
(20,32–35). With
the exception of protein kinase cyclic guanosine
monophosphate-dependent type II-PDGFRβ, PDGFRβ fusion genes are
capable of forming dimers with receptors, which leads to
autophosphorylation, and thus induces the persistent activation of
tyrosine kinases. Imatinib, a tyrosine kinase inhibitor, is
typically used to treat myeloid tumors exhibiting PDGFRβ fusion, in
order to achieve sustained remission (20,32,36). Due
to potential side-effects, including adverse drug reactions
following multiple administrations, a limited daily dosage of
imatinib has been recommended (37).
The serum creatinine value of the patient in the present study
gradually increased following treatment with imatinib (400 mg/day)
for 4 days, thus the daily dosage of imatinib was reduced to 300
mg/day. On day 5 of treatment, percussive pain over the left renal
region and hematuria were detected, and kidney stones were
diagnosed by ultrasound. Therefore, a reduced dosage of imatinib
was subsequently administered (100 mg/day), and kidney-sparing
surgery was successfully performed in order to prevent
deterioration of the patient. As symptoms were controlled by using
a lower dose of imatinib, low dosages of imatinib may be an
effective therapy for MDS/MPN associated with PDGFRβ-CEV14, however
the long-term curative effects of this therapeutic strategy require
further investigation.
Detection of PDGFRβ-associated fusion genes in
individual patients appears to be necessary for definitive
diagnosis, guiding treatment, predicting prognosis and monitoring
minimal residual disease in MDS/MPN. In the present study, an
elderly patient was diagnosed with a myeloid tumor associated with
the PDGFRβ-CEV14 fusion gene, using the methods of FISH and RT-PCR.
These methods were therefore proven to be of significant value in
improving diagnosis, guiding treatment and increasing the cure rate
of MDS/MPN patients, via the detection of multiple genes exhibiting
rearrangement, which are associated with PDGFRβ in MDS/MPN.
Acknowledgements
The present study was supported by the National
Natural Science Foundation of China (Beijing, China; grant no.
81200383).
References
|
1
|
Reilly JT: Class III receptor tyrosine
kinases: Role in leukaemogenesis. Br J Haematol. 116:744–757. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Heldin CH, Ostman A and Rönnstrand L:
Signal transduction via platelet-derived growth factor receptors.
Biochim Biophys Acta. 1378:F79–F113. 1998.PubMed/NCBI
|
|
3
|
Donovan J, Shiwen X, Norman J and Abraham
D: Platelet-derived growth factor alpha and beta receptors have
overlapping functional activities towards fibroblasts. Fibrogenesis
Tissue Repair. 6:102013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Demoulin JB, Enarsson M, Larsson J,
Essaghir A, Heldin CH and Forsberg-Nilsson K: The gene expression
profile of PDGF-treated neural stem cells corresponds to partially
differentiated neurons and glia. Growth Factors. 24:184–196. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Steensma DP, Tefferi A and Li CY: Splenic
histopathological patterns in chronic myelomonocytic leukemia with
clinical correlations: reinforcement of the heterogeneity of the
syndrome. Leuk Res. 27:775–782. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Emanuel PD: Juvenile myelomonocytic
leukemia and chronic myelomonocytic leukemia. Leukemia.
22:1335–1342. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Vardiman JW: The World Health Organization
(WHO) classification of tumors of the hematopoietic and lymphoid
tissues: an overview with emphasis on the myeloid neoplasms. Chem
Biol Interact. 184:16–20. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Finelli P, Giardino D, Rizzi N, Buiatiotis
S, Virduci T, Franzin A, Losa M and Larizza L: Non-random trisomies
of chromosomes 5, 8 and 12 in the prolactinoma sub-type of
pituitary adenomas: conventional cytogenetics and interphase FISH
study. Int J Cancer. 86:344–350. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Verma RS and Dosik H: The value of reverse
banding in detecting bone marrow chromosomal abnormalities:
Translocation between chromosomes 1, 9, and 22 in a case of chronic
myelogenous leukemia (CML). Am J Hematol. 3:171–175. 1977.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Claussen U, Michel S, Mühlig P, Westermann
M, Grummt UW, Kromeyer-Hauschild K and Liehr T: Demystifying
chromosome preparation and the implications for the concept of
chromosome condensation during mitosis. Cytogenet Genome Res.
98:136–146. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Shaffer LG, Slovak ML and Campbell LJ:
ISCN 2009: An International System for Human Cytogenetic
Nomenclature (2009): Recommendations of the International Standing
Committee on Human Cytogenetic Nomenclature (1st). Switzerland: S
Karger AG. 2009.
|
|
12
|
Guo B, Da WM, Han XP, Zhao DD, Jin HJ,
Wang K and Tang JY: Study of BCR-ABL gene rearrangement by
dual-color-dual-fusion fluorescence in situ hybridization on
acute lymphoblastic leukemia patients. Chin J Lab Med. 10:902–905.
2006.
|
|
13
|
Huang W, Cao Q and Lu Y: Detection on
BCR-ABL fusion gene in Ph1 chromosome positive leukemia by ‘nested’
retrotranscriptase/polymerase chain reaction. Chin J Hema.
13:183–186. 1992.(In Chinese).
|
|
14
|
Abe A, Emi N, Tanimoto M, Terasaki H,
Marunouchi T and Saito H: Fusion of the platelet-derived growth
factor receptor β to a novel gene CEV14 in acute myelogenous
leukemia after clonal evolution. Blood. 90:4271–4277.
1997.PubMed/NCBI
|
|
15
|
Levine RL, Wadleigh M, Sternberg DW,
Wlodarska I, Galinsky I, Stone RM, DeAngelo DJ, Gilliland DG and
Cools J: KIAA1509 is a novel PDGFRB fusion partner in
imatinib-responsive myeloproliferative disease associated with a
t(5;14)(q33;q32). Leukemia. 19:27–30. 2005.PubMed/NCBI
|
|
16
|
Vizmanos JL, Novo FJ, Román JP, Baxter EJ,
Lahortiga I, Larráyoz MJ, Odero MD, Giraldo P, Calasanz MJ and
Cross NC: NIN, a gene encoding a CEP110-like centrosomal protein,
is fused to PDGFRB in a patient with a t(5;14)(q33;q24) and an
imatinib-responsive myeloproliferative disorder. Cancer Res.
64:2673–2676. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Bain BJ: Leukaemia Diagnosis (4th).
Chichester: Wiley-Blackwell. 68–73. 2010.
|
|
18
|
Provan A, Baglin T, Dokal I and de Vos J:
Myelodysplasia. Oxford Handbook of Clinical Haematology (3rd).
(Oxford). Oxford University Press. 244–247. 2009.
|
|
19
|
Walz C, Metzgeroth G, Schoch C, Haferlach
T, Hehlmann R, Hochhaus A, Cross NCP and Reiter A: Characterization
of two new imatinib-responsive fusion genes generated by disruption
of PDGFRB in eosinophilia-associated chronic myeloproliferative
disorders. Blood. 108:6672006.
|
|
20
|
Apperley JF, Gardembas M, Melo JV,
Russell-Jones R, Bain BJ, Baxter EJ, Chase A, Chessells JM,
Colombat M, Dearden CE, et al: Response to imatinib mesylate in
patients with chronic myeloproliferative diseases with
rearrangements of the platelet-derived growth factor receptor beta.
N Engl J Med. 347:481–487. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Golub TR, Barker GF, Lovett M and
Gilliland DG: Fusion of PDGF receptor beta to a novel ets-like
gene, tel, in chronic myelomonocytic leukemia with t(5;12)
chromosomal translocation. Cell. 77:307–316. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ritchie KA, Aprikyan AA, Bowen-Pope DF,
Norby-Slycord CJ, Conyers S, Bartelmez S, Sitnicka EH and Hickstein
DD: The Tel-PDGFRbeta fusion gene produces a chronic
myeloproliferative syndrome in transgenic mice. Leukemia.
13:1790–1803. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Hélias C, Leymarie V, Entz-Werle N,
Falkenrodt A, Eyer D, Costa JA, Cherif D, Lutz P and Lessard M:
Translocation t(5;14)(q35;q32) in three cases of childhood T cell
acute lymphoblastic leukemia: A new recurring and cryptic
abnormality. Leukemia. 16:7–12. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Bernard OA, Busson-LeConiat M, Ballerini
P, et al: A new recurrent and specific cryptic translocation,
t(5;14)(q35;q32), is associated with expression of the Hox11L2 gene
in T acute lymphoblastic leukemia. Leukemia. 15:1495–1504. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Haider S, Matsumoto R, Kurosawa N, et al:
Molecular characterization of a novel translocation
t(5;14)(q21;q32) in a patient with congenital abnormalities. J Hum
Genet. 51:335–340. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Su XY, Della-Valle V, Andre-Schmutz I, et
al: HOX11L2/TLX3 is transcriptionally activated through T-cell
regulatory elements downstream of BCL11B as a result of the
t(5;14)(q35;q32). Blood. 108:4198–4201. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Berger R, Dastugue N, Busson M, Van Den A
kker J, Pérot C, Ballerini P, Hagemeijer A, Michaux L, Charrin C,
Pages MP, et al: Groupe Français de Cytogénétique Hématologique
(GFCH): t(5;14)/HOX11L2-positive T-cell acute lymphoblastic
leukemia. A collaborative study of the Groupe Français de
Cytogénétique Hématologique (GFCH). Leukemia. 17:1851–1857. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
van Zutven LJ, Velthuizen SC,
Wolvers-Tettero IL, van Dongen JJ, Poulsen TS, MacLeod RA, Beverloo
HB and Langerak AW: Two dual-color split signal fluorescence in
situ hybridization assays to detect t(5;14) involving HOX11L2
or CSX in T-cell acute lymphoblastic leukemia. Haematologica.
89:671–678. 2004.PubMed/NCBI
|
|
29
|
Nagel S, Scherr M, Kel A, Hornischer K,
Crawford GE, Kaufmann M, Meyer C, Drexler HG and MacLeod RA:
Activation of TLX3 and NKX2–5 in t(5;14)(q35;q32) T-cell acute
lymphoblastic leukemia by remote 3′-BCL11B enhancers and
coregulation by PU.1 and HMGA1. Cancer Res. 67:1461–1471. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Cavé H, Suciu S, Preudhomme C, Poppe B,
Robert A, Uyttebroeck A, Malet M, Boutard P, Benoit Y, Mauvieux L,
et al: EORTC-CLG: Clinical significance of HOX11L2 expression
linked to t(5;14)(q35;q32), of HOX11 expression, and of SIL-TAL
fusion in childhood T-cell malignancies: Results of EORTC studies
58881 and 58951. Blood. 103:442–450. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Shi HT, Zhou F, Hou J, Wei W, Guo LP and
Zhang YX: A case of T-cell acute lymphpoblastic leukemia with
translocation t(5;14) (q33; q32). J Chin Hematol. 06:8002013.(In
Chinese).
|
|
32
|
Wilkinson K, Velloso ER, Lopes LF, Lee C,
Aster JC, Shipp MA and Aguiar RC: Cloning of the t(1;5)(q23;q33) in
a myeloproliferative disorder associated with eosinophilia:
Involvement of PDGFRB and response to imatinib. Blood.
102:4187–4190. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Baxter EJ, Kulkarni S, Vizmanos JL, Jaju
R, Martinelli G, Testoni N, Hughes G, Salamanchuk Z, Calasanz MJ,
Lahortiga I, et al: Novel translocations that disrupt the
platelet-derived growth factor receptor beta (PDGFRB) gene in
BCR-ABL-negative chronic myeloproliferative disorders. Br J
Haematol. 120:251–256. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Cross NC and Reiter A: Tyrosine kinase
fusion genes in chronic myeloproliferative diseases. Leukemia.
16:1207–1212. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Salaroli A, Loglisci G, Serrao A, Alimena
G and Breccia M: Fasting glucose level reduction induced by
imatinib in chronic myeloproliferative disease with TEL-PDGFRβ
rearrangement and type 1 diabetes. Ann Hematol. 91:1823–1824. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Gallagher G, Horsman DE, Tsang P and
Forrest DL: Fusion of PRKG2 and SPTBN1 to the platelet-derived
growth factor receptor beta gene (PDGFRB) in imatinib-responsive
atypical myeloproliferative disorders. Cancer Genet Cytogenet.
181:46–51. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Tanaka MF, Kantarjian H, Cortes J, Ohanian
M and Jabbour E: Treatment options for chronic myeloid leukemia.
Expert Opin Pharmaco. 13:815–828. 2012. View Article : Google Scholar
|