Introduction
Hepatoblastoma (HB) is the most common liver tumor
of childhood (1). If complete
surgical resection of the tumor is achieved, the prognosis of
children with HB is favorable, with or without additional
chemotherapy (standard-risk patients) (1). Despite recent advances in therapy for
these children, prognosis remains poor for high-risk patients
(1,2).
Among high-risk children, chemotherapy is crucial in addition to
surgical therapy. However, multi-drug resistance to chemotherapy
significantly limits the ability to successfully treat these
patients (1,3). Therefore, the employment of novel
anticancer agents against HB is needed.
The use of neurokinin-1 receptor (NK1R; also known
as TACR1) antagonists is a novel and promising approach for
future anticancer strategies (4). The
peptide substance P (SP; also known as TAC1) is a widely
distributed neuronal transmitter that, after binding specifically
to NK1R, triggers a broad variety of functions (5). It is known that SP can induce tumor cell
proliferation, angiogenesis and migration via NK1R, and that the
SP/NK1R complex is an integral part of the cancer cell itself, as
well as its tumor microenvironment (6). Aprepitant, a non-peptide NK1R
antagonist, is a clinical agent approved by the Food and Drug
Administration for the treatment of chemotherapy-induced nausea and
vomiting. Its effects as an anticancer agent have been described
extensively in vitro and in vivo (6–11).
Notably, evidence indicates that it has limited toxic side effects
even when administered in high doses (6,12).
In a previous study, we described that TACR1
is highly expressed in human HB, predominantly in its truncated
form [truncated-TACR1 (tr-TACR1)] (8). Compared with full-length
(fl-TACR1), tr-NK1R lacks 96 amino acids at the cytoplasmic
C-terminus of the receptor that are responsible for intracellular
signal transduction. Although this splice variant is considered to
be able to couple G proteins, it exhibits decreased efficiency with
respect to internalization and desensitization (8,13–15). The net result of this is a decreased
ability for negative feedback inhibition, allowing constant
activation despite saturation of the receptor complex (13–15). This,
in turn, may contribute to the correlation of expression of this
particular splice variant with cancer. In an experimental HB
setting, NK1R antagonists acted as highly active anticancer agents
in vitro and in vivo, and functioned synergistically
with established chemotherapy agents in vitro (8).
In addition to these findings, a molecular 16-gene
signature has been described for HB, in order to better classify
molecular patterns and biological characteristics of these tumors
(16,17). Using this signature, two tumor
subclasses resembling distinct phases of liver development can be
identified. Notably, this signature discriminates invasive and
metastatic from localized HB and predicts prognosis with high
accuracy (16). Additionally, it has
recently been suggested that the expression of TACR1 may
correlate with a clinically worse prognosis in some cancers
(18–22). However, scientific evidence for such
an association remains scarce. No study has previously focused on
the expression of TACR1 and a possible association with the
clinical prognosis in HB. Therefore, the present study analyzed the
expression pattern of this target among human HB subsets and
investigated whether it correlates with clinical characteristics,
such as stage, biology and outcome, including a 16-gene molecular
signature known to correlate with prognosis in these tumors. The
current results showed that tr-TACR1 is overexpressed
compared with tumor-free liver tissue in HB. Addtionally,
tr-TACR1 was expressed ubiquitously among the different
subsets of HB. Therefore, NK1R may serve as a potent anticancer
target in a number of patients with HB, independent of tumor
biology and clinical stage.
Patients and methods
Patients and tumor tissues
Analysis of tumor tissue samples from patients with
HB (n=47) who were all part of the German Cooperative Pediatric
Liver Tumor Registry Study HB99 and its subsequent Register for
Pediatric Liver Tumors was performed. The two registries were
multicentric and were initiated by the German Society for Pediatric
Oncology and Hematology. They were open to registration for
patients from Germany, Austria and Switzerland up to the age of 20
years with untreated HB. The registry protocols were assigned by
the institutional Ethical Committee of the University Children's
Hospital Basel (Basel, Switzerland) and the University of Bonn
(Bonn, Germany), and written consent was obtained from the parents
for treatment, data collection and analysis.
Clinical information, including demographic,
therapeutic, tumor and clinical outcome variables, were retrieved
from the two clinical studies. The treatment protocol consisted of
preoperative chemotherapy followed by delayed surgery and
postoperative chemotherapy according to two risk groups (standard-
versus high-risk). The two risk groups were based on the
International Childhood Liver Tumor Strategy Group risk criteria
(23). Standard risk patients
received two or three courses of neoadjuvant ifosfamide, cisplatin
and doxorubicin (IPA) chemotherapy prior to surgery (1
g/m2 ifosfamide every 72 h, days 1–3; 20
mg/m2 cisplatin every 1 h, days 4–8; and 60
mg/m2 doxorubicin every 48 h, days 9–10). Radical
surgery was conducted after the second or third course depending on
the resectability. Postoperatively, another course of IPA was
applied. In case of microscopically incomplete resection, two
adjuvant courses of IPA were administered. Patients with
small-extended tumors (PRETEXT stage I) (24) could be resected without neoadjuvant
chemotherapy and were treated with two courses of IPA
postoperatively. High-risk patients received up to seven courses of
carboplatin-based chemotherapy preoperatively depending on tumor
shrinkage and resectability. Patients were initially treated with
two courses of carbo/VP16 (200 mg/m2 carboplatin every
24 h, days 1–4; and 100 mg/m2 etoposide every 24 h, days
1–4) followed by stem cell collection. In case of tumor response,
the therapy was continued with high dose carboplatin and etoposide
(500 mg/m2 per 24 h, days 8–5) following autologous stem
cell transplantation. Patients without tumor response were treated
with IPA. Resection was scheduled as soon as the tumor was
determined to be completely resectable. In case of persisting
non-resectability, liver transplantation was recommended. Lung
metastases were resected if residual metastases were still observed
on radiological images after chemotherapy.
Tumor specimens were reviewed by the local
institution as well as the Institute of Pediatric Pathology,
University of Kiel (Kiel, Germany), which served as a reference
center. Matched adjacent liver tissue samples from the surgical
specimens without macroscopic or microscopic tumors served as
tumor-free controls (n=9). Clinical and molecular data, such as
gender, age at diagnosis, PRETEXT staging (24), including vascular invasion and
multifocality, metastatic disease, histology, CTNNB1
mutation, 16-gene signature and overall survival, were retrieved
from the HB99 database and our recent exome sequencing study,
respectively (25).
RNA extraction and reverse
transcription
RNA extraction, complementary (c)DNA synthesis and
quantitative polymerase chain reaction (qPCR) analysis were
performed as previously described (26). Briefly, total RNA was isolated from
all the samples using TRIzol® reagent (Invitrogen Life
Technologies, Carlsbad, CA, USA) and dissolved in RNase-free water.
The purity and quality of the RNA was checked using a Nanodrop®
2000 spectrophotometer (Thermo Fisher Scientific, Inc., Waltham,
MA, USA). RNA (2 µg) was reverse transcribed using SuperScript™ II
reverse transcriptase (Invitrogen Life Technologies), according to
the manufacturer's instructions. The amplification reactions were
performed with 40 ng complementary DNA, 500 nM forward and reverse
primers and iTaq SYBR®-Green Supermix (Bio-Rad Laboratories,
Hercules, CA, USA) in a final reaction volume of 20 µl and were
incubated at 95°C for 7 min, subjected to 40 cycles of 95°C for 30
sec, 60°C for 30 sec and 72°C for 30 sec, followed by a final
extension cycle at 72°C for 7 min. All the reactions were conducted
on ice to minimize the risk of RNA degradation. cDNA obtained was
stored at −80°C.
Reverse transcription-qPCR
(RT-qPCR)
According to the modified method of Bigioni et
al, the prepared cDNA (2 µl) was used in a PCR with specific
primers, based on the common sequence of the TACR1 (NK1R)
human isoforms, which yield a 186-bp fragment (27). Specific primers were as follows:
Forward, 5′-AACCCCATCATCTACTGCTGC-3′ and reverse,
5′-ATTTCCAGCCCCTCATAGTCG-3′ for fl-TACR1 (NM_001058.3);
forward, 5′-GGGCCACAAGACCATCTACA-3′ and reverse,
5′-AAGTTAGCTGCAGTCCCCAC-3′ for tr-TACR1 (NM_015727.2); and
forward, 5′-GCCCGAAACGCCGAATAT-3′ and reverse,
5′-CCGTGGTTCGTGGCTCTCT-3′ for the TBP housekeeping gene. The
amplification reactions were performed with iTaq SYBR®-Green
Supermix (Bio-Rad Laboratories, Hercules, CA, USA) in a final
reaction volume of 20 µl and were incubated at 95°C for 7 min,
subjected to 40 cycles of 95°C for 30 sec, 60°C for 30 sec and 72°C
for 30 sec, followed by a final extension cycle at 72°C for 7 min.
PCR was performed using a Mastercycler ep Gradient S (Eppendorf,
Hamburg, Germany) and the transcript numbers were normalized
according to the expression of the housekeeping gene. Relative
quantification of gene expression was performed using the
2−∆∆Ct method, as described by Pfaffl (28).
Statistical analysis
Data are presented as mean ± SD. Mean and individual
relative expression values of tumor and control samples are
expressed in dot plots for each group. Statistical comparisons were
performed with a standard t-test and Mann-Whitney U test using
GraphPad Prism biostatistics software (version 5.0d; GraphPad
Software, Inc., La Jolla, CA, USA). P<0.05 and P<0.01
indicated a statistically significant difference for all the
comparisons. To differentiate between a high and low expression of
TACR1 and its components, 3-fold of the mean of 9 tumor-free
control samples was used as a cutoff for high expression.
Kaplan-Meier estimates of specific survival time in the two groups
were compared using the log-rank Mantel-Cox test.
Results
TACR1 is overexpressed in human HB
patients
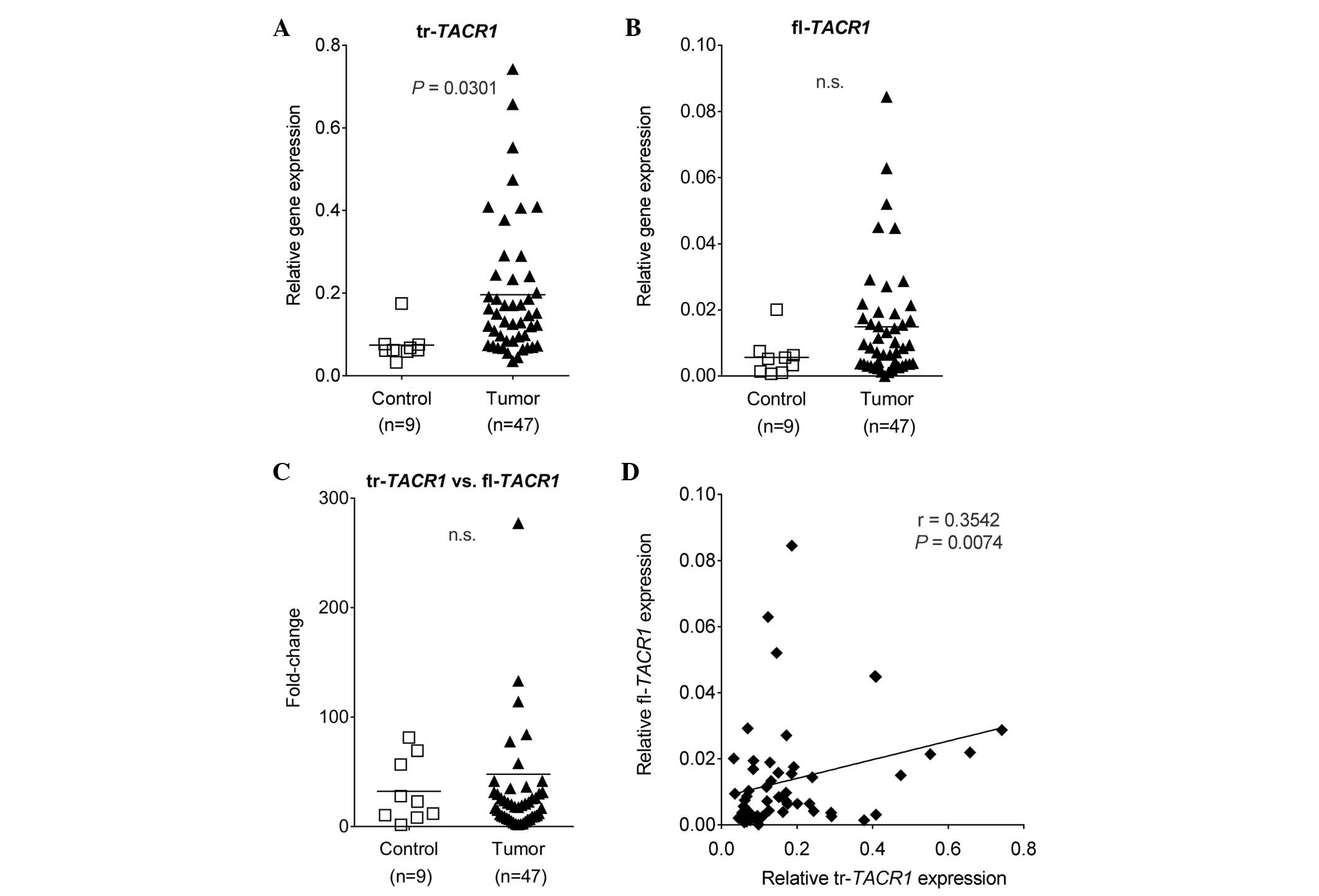
To address the aforementioned hypotheses, the gene
expression pattern of fl-TACR1 and tr-TACR1 were
analyzed in tumor tissue samples of HB and non-tumorous liver
tissue. A significantly higher expression of tr-TACR1 was
observed in HB compared with the control specimens (P=0.0301;
Fig. 1A). Although not statistically
significant, the expression of fl-TACR1 also tended to be
higher in tumor specimens (P>0.05; Fig. 1B). These results correlated with our
previous findings, in which in vitro and in vivo
models of HB were used to demonstrate that tr-TACR1 is
overexpressed in malignant HB cells. In turn, malignant HB cells
were correlated with responsiveness to treatment with NK1R
antagonists, such as aprepitant (8).
Expression of tr-TACR1 correlates with
fl-TACR1
Due to the wide range of gene expression, the ratio
of tr-TACR1 versus fl-TACR1 expression was presented.
It was found that the ratios were comparable between the tumor and
control samples (Fig. 1C), suggesting
a positive correlation of the two splice variants. When analyzed
in-depth, a statistically significant weak correlation was
identified between tr-TACR1 and fl-TACR1 expression
(r=0.3542), potentially indicating a mutual dependency (Fig. 1D).
TACR1 expression does not correlate
with biological characteristics
To improve understanding of whether splice variants
or their ratio correlate with the biological features of the tumor,
TACR1 expression was analyzed accordingly (Table I; Figs.
2–4). First, the truncated
variant was investigated, due to its significance in HB as a
potential therapeutic target (8). In
order to accomplish this, the relative expression of
tr-TACR1 was correlated with a recently described 16-gene
molecular signature known to be associated with prognosis (16). Similar to the original description of
this signature, the current cohort was separated into 29 patients
with HB that exhibited the C1 signature (poor prognosis; 61.7%) and
18 exhibited the C2 signature (improved prognosis; 38.3%) (Table I). Relative gene expression analysis
of tr-TACR1 revealed no significant difference between
patients with C1 and C2 signatures (Fig.
2A). The same features were then analyzed in correlation to the
gene expression of fl-TACR1 (Fig.
3A). A significant correlation was identified between low
fl-TACR1 expression and the C2 population of the 16-gene
signature (P=0.0222; Fig. 4A). It is
of note that 55.6% of the specimens grouped into the C2 population
exhibited extremely low levels of fl-TACR1.
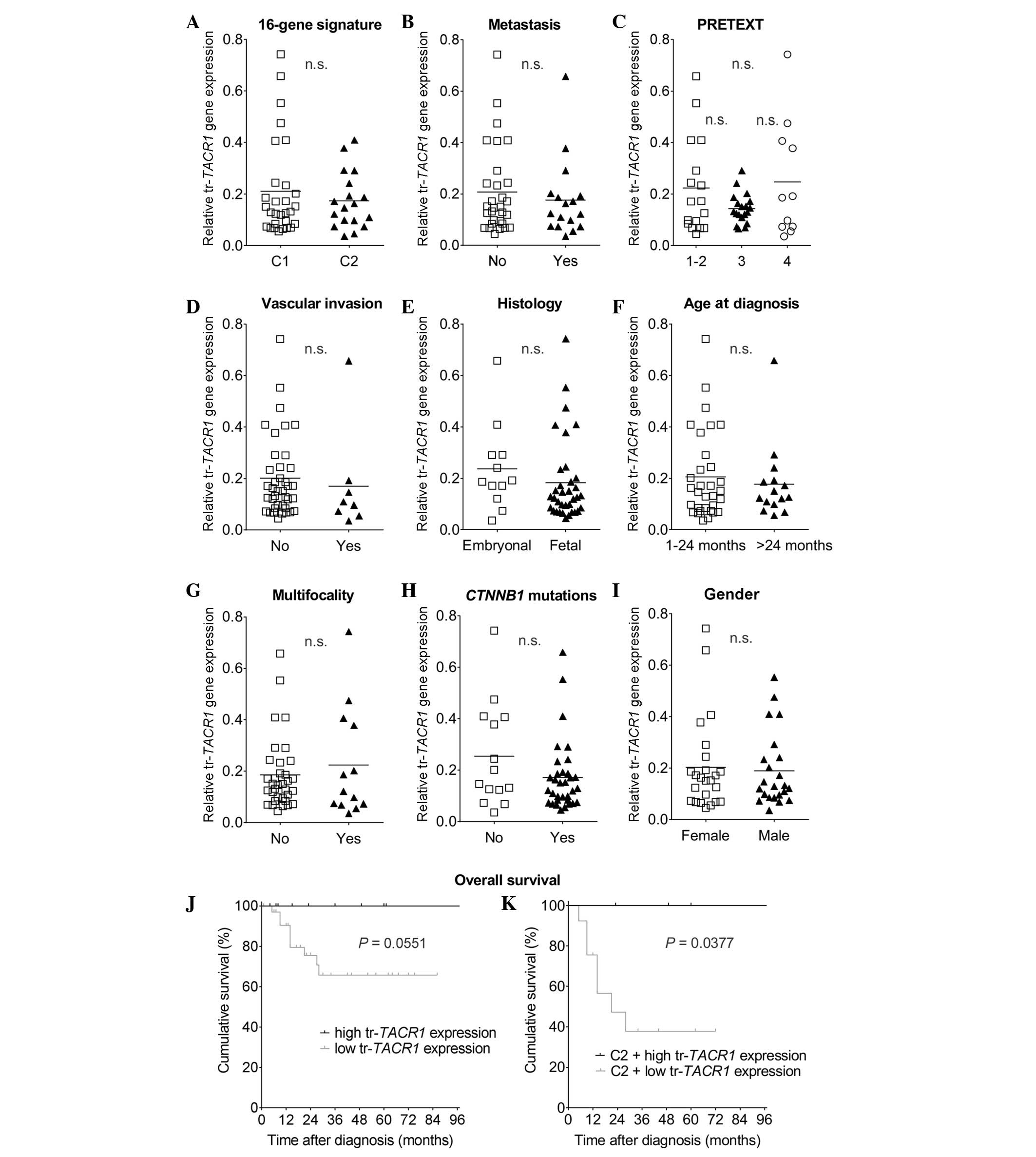 | Figure 2.tr-TACR1 expression is not
significantly associated with biological, clinical and histological
parameters. Relative gene expression of tr-TACR1 was
correlated to the (A) 16-gene signature, (B) metastasis, (C) the
preoperative staging system PRETEXT, (D) vascular invasion, (E)
histology, (F) age at diagnosis, (G) multifocality, (H)
CTNNB1 mutation status (no represents wild-type, yes
represents mutated β-catenin) and (I) gender; however, the
differences were not significant (P>0.05). (J) Overall survival
for high and low tr-TACR1 expression revealed a
non-significant difference in survival (P=0.0551). (K) Low
expression of tr-TACR1 was associated with significantly
lower overall survival in hepatoblastoma tumors harboring the C2
signature (P=0.0377). tr-TACR1, truncated-neurokinin-1
receptor; n.s., not significant. |
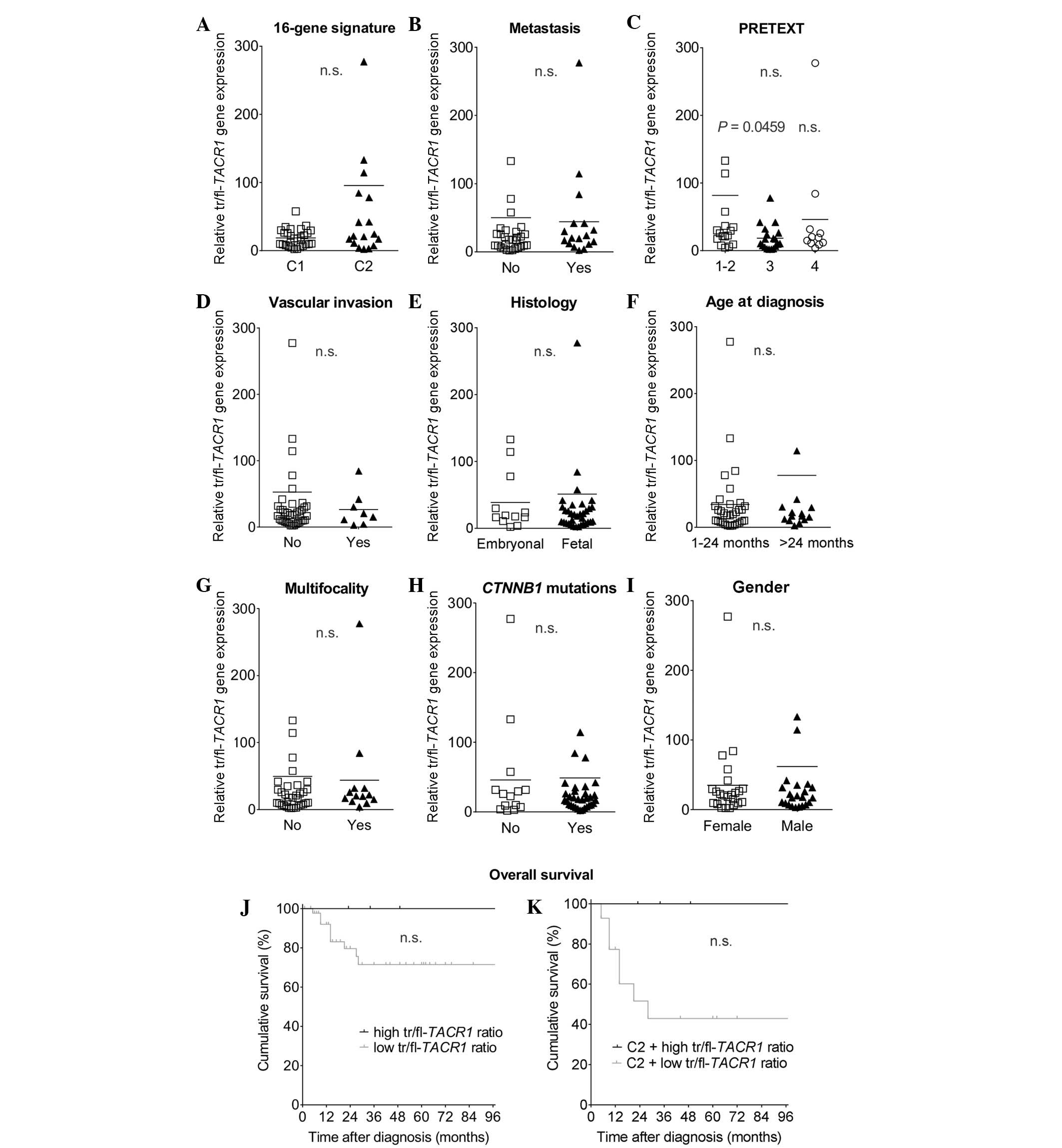 | Figure 4.Ratio of tr-TACR1 and
fl-TACR1 does not predict clinical prognosis. As in Figs. 2 and 3,
ten different clinical features were analyzed with regard to the
tr-TACR1:fl-TACR1 ratio gene expression. No
significant difference were detected in the (A) 16-gene signature,
(B) metastasis, (D) vascular invasion, (E) histology, (F) age at
diagnosis, (G) multifocality, (H) CTNNB1 mutation status and
(I) gender or (J) overall survival (P>0.05). (C) However,
PRETEXT 1–2 significantly correlated with a higher expression ratio
compared with PRETEXT 3 (P<0.05). (K) Low expression of the
tr-TACR1:fl-TACR1 ratio was associated with lower
overall survival in hepatoblastoma tumors harboring the C2
signature, however, the results were not significant (P<0.05).
tr/fl-TACR1, truncated/full-length-neurokinin-1 receptor;
n.s., not significant. |
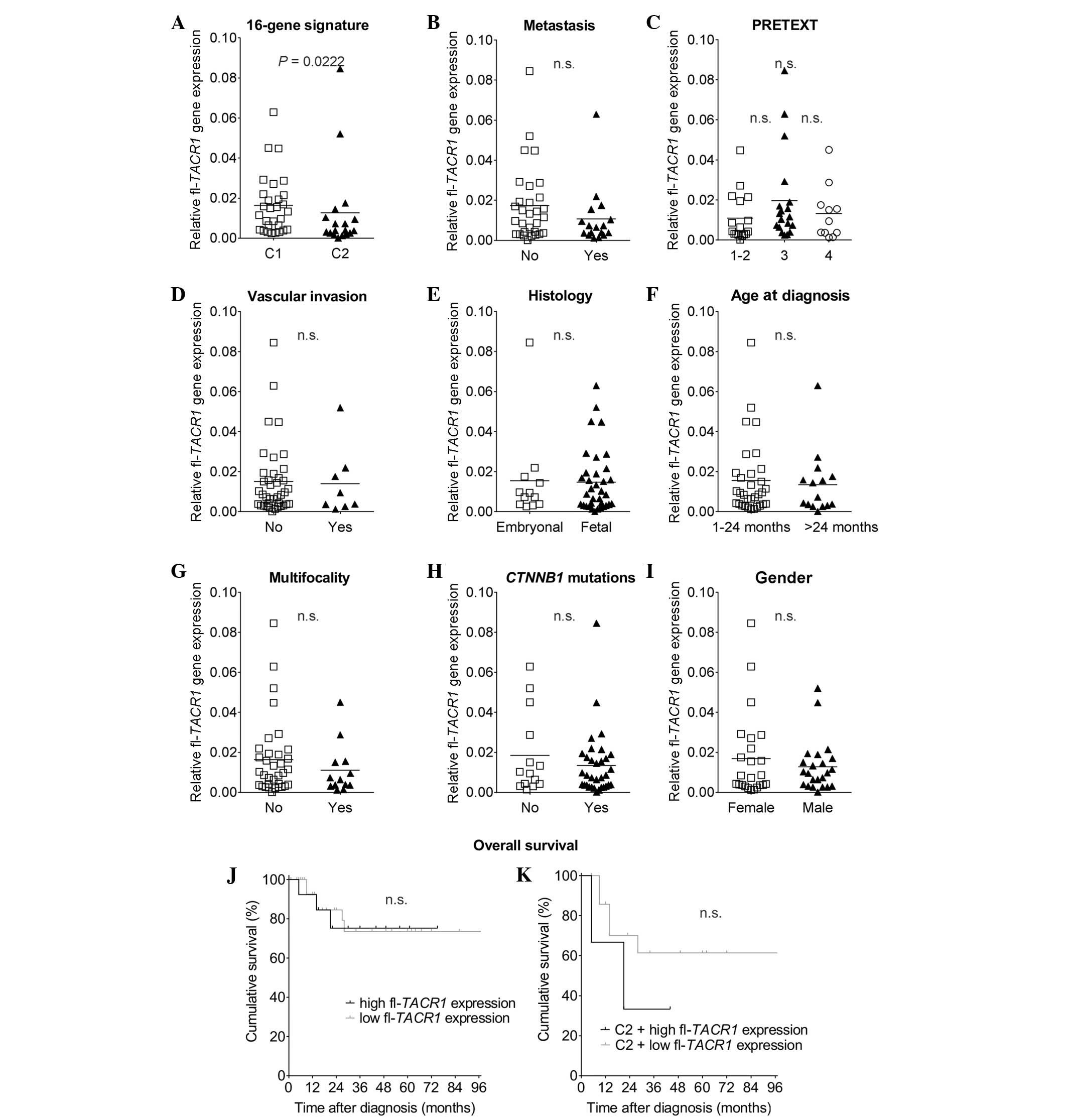 | Figure 3.fl-TACR1 expression displays
no significant difference in the majority of biological, clinical
and histological features. (A-I) Analogous to Fig. 2, relative gene expression of
fl-TACR1 was compared with the same ten parameters. (A) The
C2 signature significantly correlated with low expression of the
fl-TACR1 gene (P=0.0222). P-values for (B) metastasis, (C)
PRETEXT staging, (D) vascular invasion, (E) histology, (F) age at
diagnosis, (G) multifocality, (H) CTNNB1 mutation status and
(I) gender did not reveal any statistically significant differences
(P>0.05). (J) Analysis of overall survival for high and low
fl-TACR1 expression revealed no significant difference in
survival (P>0.05). (K) High expression of fl-TACR1 was
associated with a worse outcome in hepatoblastoma tumors harboring
the C2 signature, however, the trend was not significant
(P>0.05). fl-TACR1, full-length neurokinin-1 receptor;
n.s., not significant. |
 | Table I.Clinical, biological and histological
outcome characteristics of 47 patients with hepatoblastoma. |
Table I.
Clinical, biological and histological
outcome characteristics of 47 patients with hepatoblastoma.
| Characteristic | Patients, n
(%) |
|---|
| 16-gene
signature |
|
| C1 | 29 (61.7) |
| C2 | 18 (38.3) |
| Metastasis |
|
|
Yes | 17 (36.2) |
| No | 30 (63.8) |
| PRETEXT |
|
|
I–II | 17 (36.2) |
|
III | 19 (40.4) |
| IV | 11 (23.4) |
| Vascular
Invasion |
|
|
Yes | 8
(17.1) |
| No | 39 (82.9) |
| Histology |
|
|
Fetal | 35 (74.5) |
|
Embryonal | 12 (25.5) |
| Age at diagnosis,
months |
|
|
1–24 | 32 (68.1) |
|
>24 | 15 (31.9) |
| Multifocality |
|
|
Yes | 13 (27.7) |
| No | 34 (72.3) |
| CTNNB1
status |
|
|
Wild-type | 14 (29.8) |
|
Mutated | 33 (70.2) |
| Gender |
|
|
Female | 24 (51.1) |
|
Male | 23 (48.9) |
The ratio of fl-TACR1 to tr-TACR1 was
then calculated to determine whether it could be correlated with
the 16-gene signature (16). Notably,
extremely low ratios were identified in the favorable C1 population
and extremely high ratios were evident for the C2 population;
however, this effect was not statistically significant (data not
shown). Populations with a C2 signature were previously
demonstrated to be associated with a poor prognosis of HB (16).
Expression of TACR1 does not correlate
with clinical characteristics
The expression patterns of fl-TACR1 and
tr-TACR1 were correlated with clinical, biological and
histological characteristics, including metastasis (Figs. 2B and 3B), the preoperative classification PRETEXT
(Figs. 2C and 3C), vascular invasion (Figs. 2D and 3D), histology (Figs. 2E and 3E), onset period (Figs. 2F and 3F), multifocality (Figs. 2G and 3G), CTNNB1 mutations (Figs. 2H and 3H) and gender (Figs. 2I and 3I). Of the entire cohort, it was found that
63.8% exhibited no metastasis at the time of diagnosis, 82.9% had
no vascular invasion and only 27.7% were multifocal. Gender was
equally distributed (51.1% female vs. 48.9% male), the majority
tumors had a fetal histology (74.5 vs. 25.5% embryonal) and, as
expected, 70.2% of tumors possessed a β-catenin (CTNNB1)
mutation. The age of diagnosis was predominantly within the first
24 months of life (68.1%) and the specimens were classified as
PRETEXT 1–2 (36.2%), PRETEXT 3 (40.4%) and PRETEXT 4 (23.4%).
When analyzing tr-TACR1 expression in detail,
no statistically relevant differences were identified with respect
to the aforementioned clinical features. Notably, a high expression
of tr-TACR1 correlated with a better overall survival
(P=0.0551; Fig. 2J), although this
was only a trend as it did not reach statistical significance.
Similarly, when analyzing the pattern of
fl-TACR1 expression with metastasis, PRETEXT, vascular
invasion, histology, age at diagnosis, multifocality, CTNNB1
mutations or gender, no significant correlation was observed
(P>0.05; Fig. 3B–I). When
clustered into groups of high versus low expression of
fl-TACR1, overall survival curves did not deviate from each
other (P>0.05; Fig. 3J), contrary
to the finding for tr-TACR1 (Fig.
2J).
Use of the ratio of the two variants
(tr-TACR1:fl-TACR1), revealed no statically
significant differences with regard to the majority of the
characteristics (Fig. 4A–I). The only
exception to this was that a higher tr-TACR1:fl-TACR1
ratio, which occurred predominantly in PRETEXT 1–2 compared with
PRETEXT 3 (P=0.0459; Fig. 4C).
Similar to the analysis with tr-TACR1 alone, overall
survival was worse with a low ratio of
tr-TACR1:fl-TACR1 (P>0.05; Fig. 4J).
As the original description of the 16-gene signature
by Cairo et al (16) suggested
a worse prognosis for the C2 signature, the present study aimed to
investigate whether either factor (tr-TACR1, fl-TACR1
or the ratio thereof) could refine the predictive value in our set
of tumors. Therefore, overall survival within the C2 HB tumors was
re-analyzed, and their outcome with respect to high versus low
expression of TACR1 or its ratio was investigated. It was
identified that low tr-TACR1 predicted a poor prognosis for
C2 tumors with a higher significance than tr-TACR1 alone
(P=0.0377; Fig. 2K). Although not
significant, high fl-TACR1 suggested a worse outcome
(P>0.05; Fig. 3K), and the ratio
of the two variants had the same trend as truncated alone and as
analyzed in the whole cohort, but with a clear tendency towards a
worse prognosis for low tr/fl-TACR1 in the C2 group
(P>0.05; Fig. 4K).
Taken together, no strong correlation of
tr-TACR1, fl-TACR1 or tr-TACR1:fl-TACR1
gene expression with clinical and histological data was identified.
However, low tr-TACR1 or a low ratio was associated with a
worse prognosis, particularly when associated with the C2
signature. By contrast, no significance was identified in
fl-TACR, with a marginal trend towards a worse outcome in C2
and high fl-TACR1 expression.
Discussion
Little is known regarding the expression profile of
TACR1 and its associations with clinical outcome. NK1R is a
crucial component of cancer development and progression. Thus, NK1R
is a promising anticancer target in a multitude of cancer types,
including HB (7,8). In the present study, in-depth analysis
of the expression pattern of TACR1 in HB was performed, and
the findings were correlated with the patients' clinical tumor
stage, biology and outcome. It was determined that, compared with
tumor-free liver tissue, tumorous tissue expressed significantly
more tr-TACR1. Although the difference was not significant,
HB tissues also tended to express marginally more of
fl-TACR1. This is in accordance with our recent description
of this receptor in HB (8). Within
the tumorous tissue, expression of fl-TACR1 correlated with
the expression of tr-TACR1. Furthermore, the expression of
fl-TACR1 was lower in the C2 (poor prognosis) compared with
the C1 (improved prognosis) population of the 16-gene signature.
When analyzing the expression of low versus high fl-TACR1
within the C2 population only, no difference was found. There was
also no correlation between tr-TACR1 expression alone and
any of the tumor characteristics investigated. However, a low
expression of tr-TACR1 demonstrated a clear trend towards
worse prognosis but did not reach statistical significance. Thus,
the current data provide evidence that HB ubiquitously expresses
TACR1, supporting recent studies that NK1R antagonists may
be promising anticancer agents against a wide variety HB subsets
(8,29).
It has previously been proposed that a correlation
exists between the expression rate of the NK1R/SP complex and
prognosis in various types of cancer (18–22).
Garcia-Recio et al identified that SP contributes to
persistent transmodulation of the ErbB receptors, epidermal growth
factor receptor (EGFR) and human epidermal growth factor 2 (HER2),
in breast cancer, acting to enhance malignancy and therapeutic
resistance. Both TACR1 and TAC1 (SP) were highly
expressed in HER2+ primary breast tumors and correlated
with poor prognosis factors (18).
These findings are in contradiction to the current results in HB,
which indicated that worse prognosis was associated with a low
expression of tr-TACR1. However, it should be noted that two
separate tumor entities were investigated. In addition,
Garcia-Recio et al (18) made
no distinction between the truncated and the full-length variant of
the receptor. Notably, following treatment of xenografted mice
bearing HER2+ or HER2− human breast
carcinoma, Garcia-Recio et al (18) only observed a therapeutic effect for
HER2+ tumors, suggesting that the antitumor effects of
NK1R inhibition in carcinoma of the breast depend on the modulatory
properties of NK1R signaling on the activity of HER2 and EGFR
(18).
In a different study, Gillespie et al
identified that it was the expression of tr-TACR1 and not
fl-TACR1 that predicted the progression from quiescent
colitis to high-grade dysplasia and cancer in colitis-associated
cancer (13). This is in accordance
with the current results for HB, in which tr-TACR1 was
observed to be upregulated in cancer cells but not in non-tumorous
tissue.
Cairo et al recently described two tumor
subclasses within HB, resembling distinct phases of liver
development and containing a discriminating 16-gene signature.
Furthermore, it was found that β-catenin, a key protein of the Wnt
signaling pathway, activated different transcriptional programs in
the two distinct tumor subpopulations, C1 and C2. Notably, when
separated into the two subpopulations by this 16-gene signature,
clinical prognosis could be predicted for these children with an
extremely high accuracy (16,17). Considering these findings, the HB
tumor bank was screened in the present study and each tumor was
classified according to this specific 16-gene signature.
Subsequently, the findings were correlated with the expression of
fl-TACR1 and tr-TACR1, and it was determined that
fl-TACR1 expression was lower in the C2 signature compared
with the C1 group. A low expression of tr-TACR1 was
associated with a worse prognosis, although this was only a trend
and not significant (P=0.0551). Of note, when analysis of the C2
signature population was performed separately, a low expression of
tr-TACR1 was significantly associated with a worse prognosis
(P=0.0377). Therefore, it can be concluded that TACR1 alone
does not serve as a clinical marker for aggressiveness or potential
to metastasize in HB. However, tr-TACR1 may facilitate the
identification of tumors that have a very poor prognosis,
potentially alone but in particular within the C2 signature patient
population. More in-depth analysis of such a C2
tr-TACR1low tumor cohort is necessary to
demonstrate the value of this distinction. Additionally, when
making such distinction, it should be understood that ‘low’
expression in the present study is in reference to ‘high’
expression, as defined in the Patients and methods section. Thus, a
tumor with tr-TACR1low expression may, on
average, express significantly more tr-TACR1 compared with
non-tumorous tissue.
Previous studies identified that overexpression of
tr-TACR1 is associated with malignancy, including in HB
(6–8,30). The
present finding of low tr-TACR1 correlating with worse
prognosis initially appears to contradict this finding. Numerous
reasons exist that possibly account for this discrepancy. One
possible explanation is that tumors that express low levels of
tr-TACR1 represent an advanced stage in tumorigenesis
characterized by profound immaturity, highlighted by the fact that
a low expression of α-fetoprotein (AFP), the only accepted tumor
marker for HB, correlates with poor prognosis (1). It is proposed that this correlation
occurs because tumor cells that are unable to produce AFP are more
immature than AFP-producing tumor cells, leading to the recognized
poor prognosis. However, this hypothesis cannot be adequately
addressed by the data of the current study at this time.
Furthermore, tumors, and particularly tumors of the
liver, have been shown to be significantly heterogeneous (31). Only one sample was analyzed per tumor
in the current analysis, which may not be representative for other
areas of the cancer. In addition, gene expression does not always
correlate with protein expression. Therefore, it may be useful to
determine whether an immunohistochemical (IHC) staining
classification of HB may indicate more favorable clinical features
and improved prognosis. However, IHC staining of the different
splice variants of the NK1R/SP-complex remains a challenge and
presents a major obstacle to this endeavor. Additionally, according
to current understanding of the NK1R/SP-complex, SP is a critical
ligand required for its function. The present study did not
investigate the gene expression level of SP within the tumor or
circulating protein of it; therefore, this should be performed in
the future. Finally, all but four patients enrolled into this
retrospective registry had received chemotherapy prior to surgery
[8.8 vs. 27.7% in the original description of the 16-gene signature
by Cairo et al(16)]. This is
important to consider, as the exposure to chemotherapy could
potentially alter the expression pattern of TACR1 and its
splice variants. Our previous study demonstrated that the
expression of TACR1 did not change with prior chemotherapy
treatment in children with HB (8).
However, these data did not distinguish between the full-length and
the truncated version of the receptor (8). Therefore, the influence of systemic
chemotherapy on the expression of the NK1R complex remains, to
date, an unsolved question.
In conclusion, the results of the present study do
not indicate that the TACR1 expression pattern depends on or
predicts the clinical stage and behavior of HB. However, two splice
variants of TACR1 were demonstrated to be ubiquitously
overexpressed in HB. Furthermore, the current analysis suggests
that the prediction of overall survival in the C2
signature-expressing HB subgroup may be refined by tr-TACR1
and fl-TACR1, identifying a C2-TACR1low
population with particularly poor prognosis. Overall, the present
data further support the potential of the NK1R/SP complex as an
ideal target in a wide variety of HB subsets.
Acknowledgements
We are grateful to Mrs. Fatemeh Promoli for
technical assistance. Dr Michael Berger and Dr Matthias Ilmer were
supported by postdoctoral stipends from the German Academic
Exchange Program. Dr Michael Berger was additionally funded by the
Friedrich-Baur Foundation Munich, Münchener Medizinische
Wochenschrift, as well as the Funding for Research and Teaching of
Ludwig Maximilian University of Munich. Professor Roland Kappler
obtained funding from the Bettina Bräu Foundation (Munich, Germany)
and the Gänseblümchen-Voerde Foundation (Voerde, Germany).
References
|
1
|
von Schweinitz D: Hepatoblastoma: Recent
developments in research and treatment. Semin Pediatr Surg.
21:21–30. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Haeberle B and Schweinitz D: Treatment of
hepatoblastoma in the German cooperative pediatric liver tumor
studies. Front Biosci (Elite Ed). 4:493–498. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Warmann S, Hunger M, Teichmann B, et al:
The role of the MDR1 gene in the development of multidrug
resistance in human hepatoblastoma: Clinical course and in
vivo model. Cancer. 95:1795–1801. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Muñoz M, Rosso M and Coveñas R: The NK-1
receptor: A new target in cancer therapy. Curr Drug Targets.
12:909–921. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Palma C, Bigioni M, Irrissuto C, et al:
Anti-tumour activity of tachykinin NK1 receptor antagonists on
human glioma U373 MG xenograft. Br J Cancer. 82:480–487.
2000.PubMed/NCBI
|
|
6
|
Rosso M, Muñoz M and Berger M: The role of
neurokinin-1 receptor in the microenvironment of inflammation and
cancer. ScientificWorldJournal. 2012:3814342012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Muñoz M, Rosso M and Coveñas R: A new
frontier in the treatment of cancer: NK-1 receptor antagonists.
Curr Med Chem. 17:504–516. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Berger M, Neth O, Ilmer M, et al:
Hepatoblastoma cells express truncated neurokinin-1 receptor and
can be growth inhibited by aprepitant in vitro and in
vivo. J Hepatol. 60:985–994. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Muñoz M, Pérez A, Rosso M, Zamarriego C
and Rosso R: Antitumoral action of the neurokinin-1 receptor
antagonist L-733 060 on human melanoma cell lines. Melanoma Res.
14:183–188. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Mayordomo C, García-Recio S, Ametller E,
et al: Targeting of substance P induces cancer cell death and
decreases the steady state of EGFR and Her2. J Cell Physiol.
227:1358–1366. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Muñoz M, Berger M, Rosso M, et al:
Antitumor activity of neurokinin-1 receptor antagonists in MG-63
human osteosarcoma xenografts. Int J Oncol. 44:137–146.
2014.PubMed/NCBI
|
|
12
|
Kramer MS, Cutler N, Feighner J, et al:
Distinct mechanism for antidepressant activity by blockade of
central substance P receptors. Science. 281:1640–1645. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Gillespie E, Leeman SE, Watts LA, et al:
Truncated neurokinin-1 receptor is increased in colonic epithelial
cells from patients with colitis-associated cancer. Proc Natl Acad
Sci USA. 108:17420–17425. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ramkissoon SH, Patel PS, Taborga M and
Rameshwar P: Nuclear factor-kappaB is central to the expression of
truncated neurokinin-1 receptor in breast cancer: Implication for
breast cancer cell quiescence within bone marrow stroma. Cancer
Res. 67:1653–1659. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Patel HJ, Ramkissoon SH, Patel PS and
Rameshwar P: Transformation of breast cells by truncated
neurokinin-1 receptor is secondary to activation by
preprotachykinin-A peptides. Proc Natl Acad Sci USA.
102:17436–17441. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Cairo S, Armengol C, De Reyniès A, et al:
Hepatic stem-like phenotype and interplay of Wnt/β-catenin and Myc
signaling in aggressive childhood liver cancer. Cancer Cell.
14:471–484. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Cairo S, Armengol C and Buendia MA:
Activation of Wnt and Myc signaling in hepatoblastoma. Front Biosci
(Elite Ed). 4:480–486. 2012. View
Article : Google Scholar : PubMed/NCBI
|
|
18
|
Garcia-Recio S, Fuster G,
Fernandez-Nogueira P, et al: Substance P autocrine signaling
contributes to persistent HER2 activation that drives malignant
progression and drug resistance in breast cancer. Cancer Res.
73:6424–6434. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Esteban F, Muñoz M, González-Moles MA and
Rosso M: A role for substance P in cancer promotion and
progression: A mechanism to counteract intracellular death signals
following oncogene activation or DNA damage. Cancer Metastasis Rev.
25:137–145. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Esteban F, Gonzalez-Moles MA, Castro D, et
al: Expression of substance P and neurokinin-1-receptor in
laryngeal cancer: Linking chronic inflammation to cancer promotion
and progression. Histopathology. 54:258–260. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Castro TA, Cohen MC and Rameshwar P: The
expression of neurokinin-1 and preprotachykinin-1 in breast cancer
cells depends on the relative degree of invasive and metastatic
potential. Clin Exp Metastasis. 22:621–628. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Misawa K, Kanazawa T, Misawa Y, et al:
Frequent promoter hypermethylation of tachykinin-1 and tachykinin
receptor type 1 is a potential biomarker for head and neck cancer.
J Cancer Res Clin Oncol. 139:879–889. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Pritchard J, Brown J, Shafford E, et al:
Cisplatin, doxorubicin, and delayed surgery for childhood
hepatoblastoma: A successful approach - results of the first
prospective study of the International Society of Pediatric
Oncology. J Clin Oncol. 18:3819–3828. 2000.PubMed/NCBI
|
|
24
|
Roebuck DJ, Aronson D, Clapuyt P, et al:
International Childrhood Liver Tumor Strategy Group: PRETEXT: A
revised staging system for primary malignant liver tumours of
childhood developed by the SIOPEL group. Pediatr Radiol.
37:123–132; quiz 249–150. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Eichenmüller M, Trippel F, Kreuder M, et
al: The genomic landscape of hepatoblastoma and their progenies
with HCC-like features. J Hepatol. 61:1312–1320. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Eichenmüller M, Gruner I, Hagl B, Häberle
B, Müller-Höcker J, von Schweinitz D and Kappler R: Blocking the
hedgehog pathway inhibits hepatoblastoma growth. Hepatology.
49:482–490. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Bigioni M, Benzo A, Irrissuto C, Maggi CA
and Goso C: Role of NK-1 and NK-2 tachykinin receptor antagonism on
the growth of human breast carcinoma cell line MDA-MB-231.
Anticancer Drugs. 16:1083–1089. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Pfaffl MW: A new mathematical model for
relative quantification in real-time RT-PCR. Nucleic Acids Res.
29:e452001. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Muñoz M and Coveñas R: Neurokinin-1
receptor: A new promising target in the treatment of cancer. Discov
Med. 10:305–313. 2010.PubMed/NCBI
|
|
30
|
Muñoz M and Rosso M: The NK-1 receptor
antagonist aprepitant as a broad spectrum antitumor drug. Invest
New Drugs. 28:187–193. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Nault JC and Villanueva A: Intratumor
molecular and phenotypic diversity in hepatocellular carcinoma.
Clin Cancer Res. 10:1786–1788. 2015. View Article : Google Scholar
|