Introduction
Cystadenoma of the salivary gland is an uncommon
benign neoplasm that is further subdivided into papillary and
mucinous types (1,2). Cystadenoma accounts for 4.2–4.7% of all
benign tumors, and 2% of all minor tumors of the salivary gland,
worldwide (3–5). This tumor closely resembles Warthin
tumors, but does not demonstrate the lymphoid elements; Warthin
tumors are strongly associated smoking and commonly present as
asymptomatic slow-growing round masses. They are typically composed
of glandular and cystic strutures, occassionally with a papillary
cystic arrangement. Typically, the tumors are lined by an
epithelial bilayer comprised of inner columnar eosinophilic or
oncocytic cells surrounded by smaller basal cells and the stroma
contains a variable amount of lymphoid tissue with germinal centres
(6). The most frequent clinical
finding of salivary gland cystadenoma is a painless mass beneath
the mucosa of the palate, lips or buccal mucosa. Oncocytic change
can be observed focally or extensively. The majority of cystadenoma
cases are treated by simple excision, and recurrence is extremely
rare (3). The present study reports
an extremely rare case of a papillary cystadenoma arising from the
palate, with oncocytic features. Written informed consent was
obtained from the patient.
Case report
A 60-year-old man was referred by his dentist to the
Second Department of Oral and Maxillofacial Surgery at Osaka Dental
University Hospital (Osaka, Osaka, Japan) for the diagnosis of a
mass of the left palate in August 2008. This mass had been
identified by the dentist approximately one month prior to the
diagnosis, and the patient had not identified the tumor previously.
Physical examination revealed a mass that was 10 mm in diameter,
well-circumscribed, elastic, soft, round and located on the left
hard palate (Fig. 1). The surface of
the mass was smooth and a normal color. The hematological and
biochemical examinations were within the normal limits; white blood
cell count, 49.1×102/µl (normal range,
35.0–80.0×102/µl); red blood cell count,
445×104/µl (normal range, 380–480×104/µl);
hemoglobin level, 13.7 g/dl (normal range, 11.3–15.2 g/dl);
hematocrit, 39.1% (normal range, 34.0–43.0%); platelet count,
14.0×104/µl (normal range, 15.0–35.0×104/µl);
aspartate aminotransferase level, 18 U/l (normal range, 7–38 U/l);
alanine aminotransferase level, 15 U/l (normal range, 4–44 U/l);
alkaline phosphatase level, 178 U/l (normal range, 106–220 U/l);
lactate dehydrogenase level, 197 U/l (normal range, 106–345 U/l);
C-reactive protein level, 0.05 mg/dl (normal range, 0.00–0.30
mg/dl). Although the platelet count was marginally lower than
normal, the level was not significant enough to have an impact on
symptoms. Based on the findings of the physical examination, the
benign salivary gland tumor was pre-operatively diagnosed, and an
incisional biopsy was performed in September 2008. The microscopic
findings (magnification, ×20) were interpreted as consistent with a
papillary oncocytic cystadenoma. Therefore, the lesion was excised
under general anesthesia in November 2008. Subsequent to the
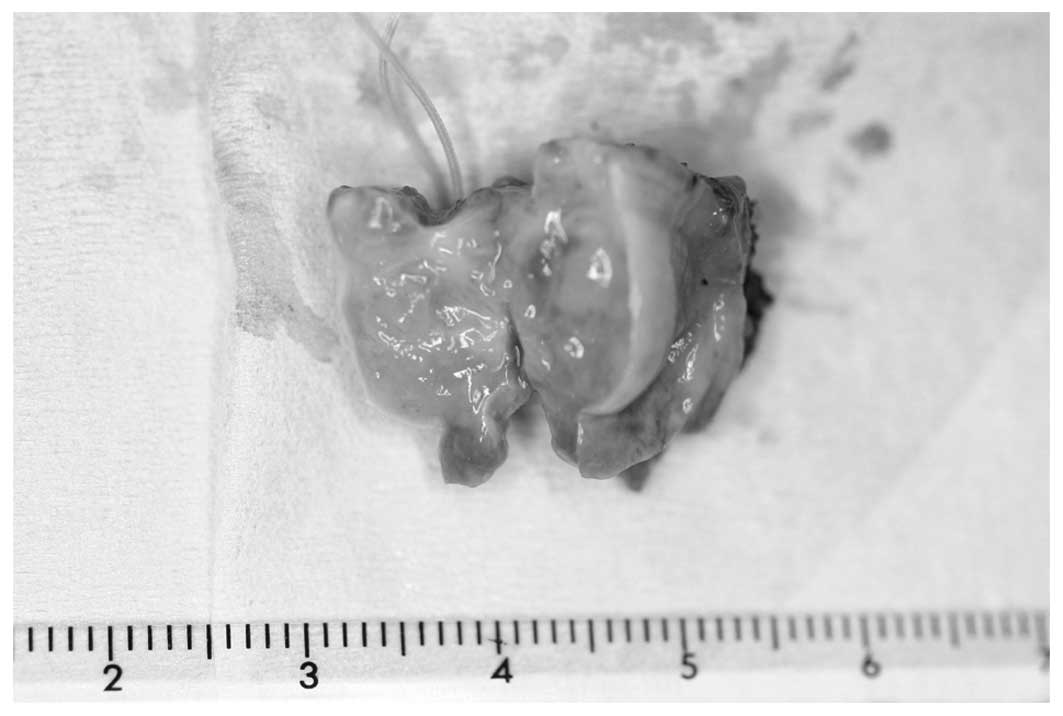
procedure, the healing was uneventful. The excised mass was a solid
soft-tissue mass 10×9 mm in size, which was white-yellow in color
on the cut surface (Fig. 2).
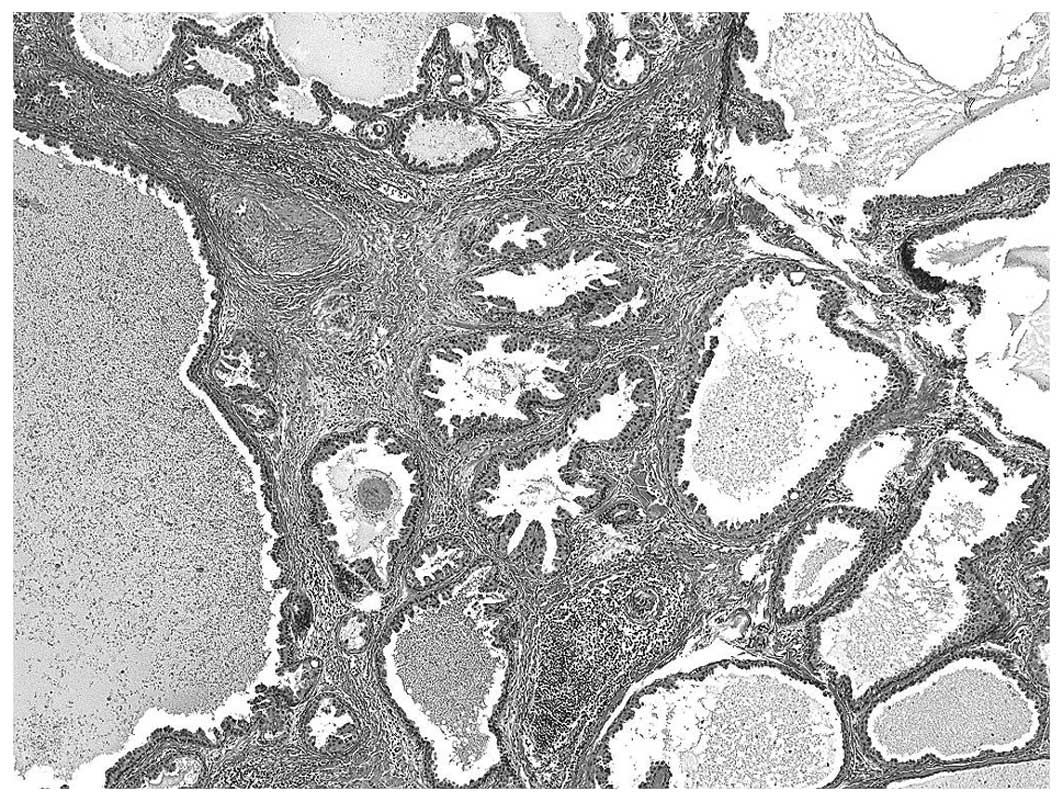
Microscopic examination (BX50; Olympus Corporation, Tokyo, Japan)
of hematoxylin-stained tissue sections and certain papillary
intraluminal projections revealed a submucosal adenomatous cystic
nodule (Fig. 3). The latter findings
were supported, as the core of the thin fibrous connective tissue
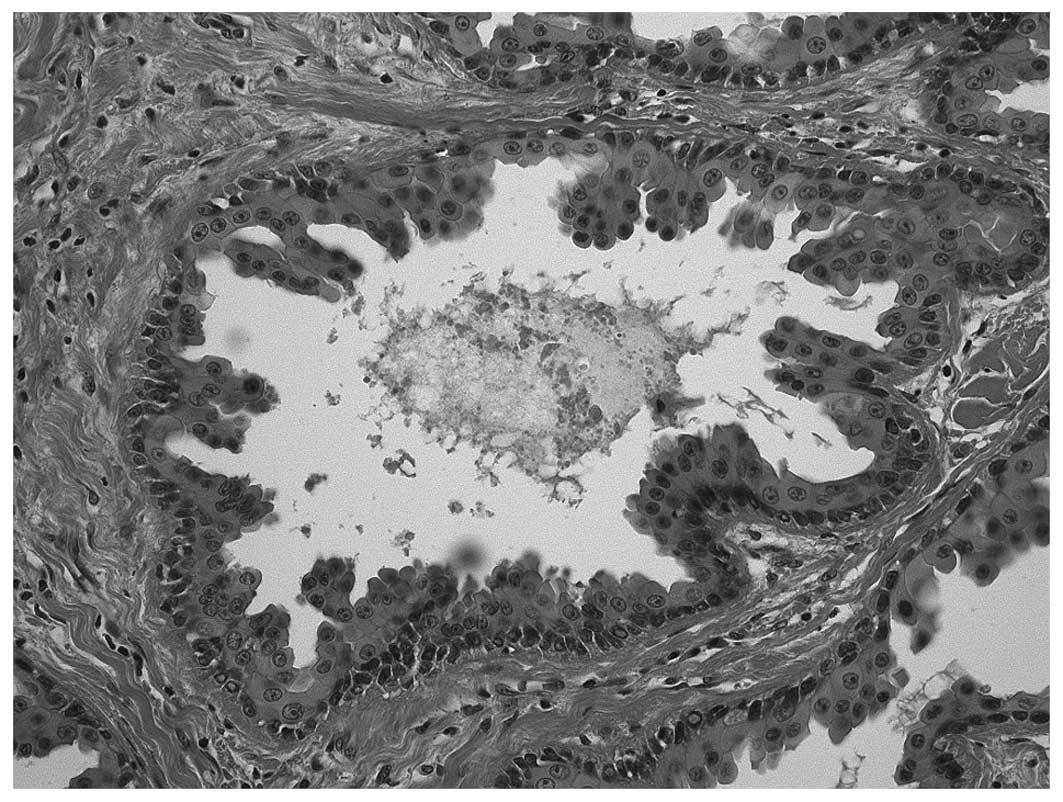
lacked lymphocytic components. Cystic papillary projections and the
major cyst cavity were lined by bilayer oncocytic columnar
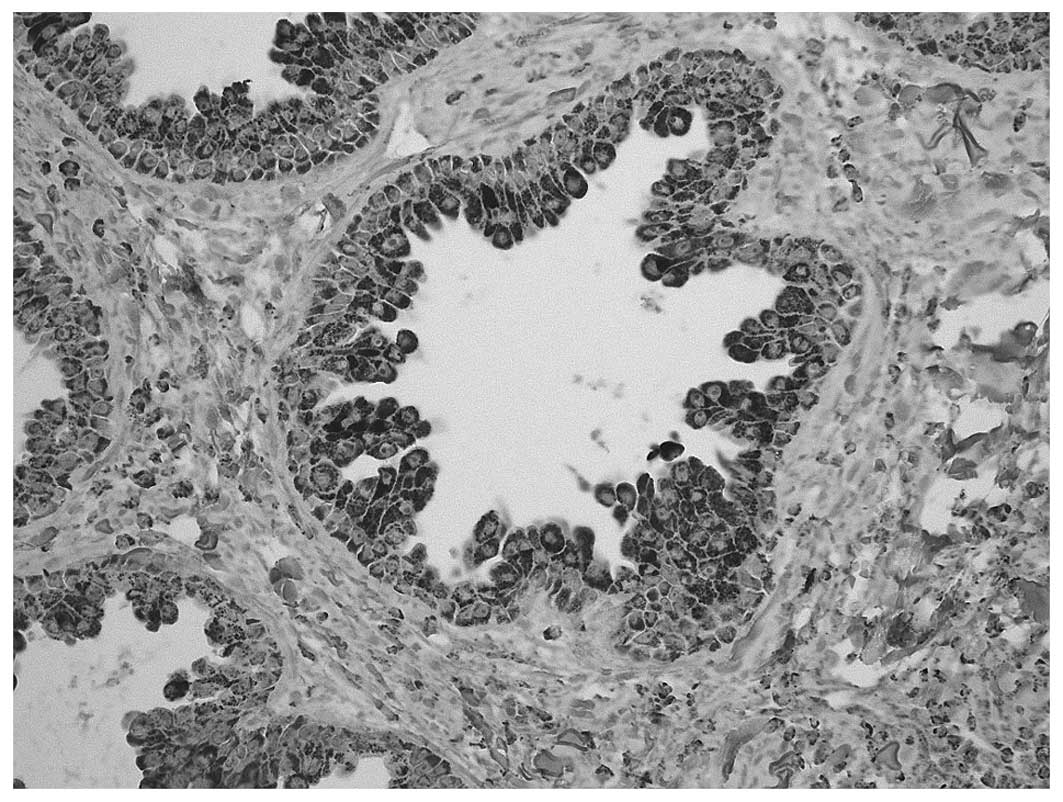
epithelium (Fig. 4). Mitotic figures
and cytological atypia were not observed. Mitochondria (EMD
Millipore, Temecula, CA, USA) were found to be present in the
oncocytic columnar epithelium using immunohistochemistry
(monoclonal mouse anti-human mitochondria antibody; cat. no.
MAB1273; 1:100; EMD Millipore) (Fig.
5). Therefore, the histopathological diagnosis of papillary
oncocytic cystadenoma was made. The post-operative course was
uneventful, and there has been no evidence of recurrence at 5 years
subsequent to the procedure.
Discussion
Cystadenoma of the salivary gland was first
subclassified into various types of monomorphic adenoma in the
first edition of the World Health Organization Histological
Classification of Salivary Gland Tumors (1). In the second edition, which was
published in 1991, cystadenomas were more clearly defined as a
specific histopathological entity that was further subdivided into
papillary and mucinous types (2).
However, in the third classification published in 2005,
cystadenomas were only subdivided into papillary and mucinous types
(6).
The frequency of papillary cystadenoma is extremely
low. Toida et al (7) reported
1 case of papillary cystadenoma among 82 cases of intraoral minor
salivary gland tumors. Chaudhry et al (8) reported only 3 cases of the tumor (7.0%)
out of 43 cases of intraoral benign minor salivary gland tumors. In
addition, out of the 800 benign intraoral minor salivary gland
tumors reported in the English language literature between 1927 and
1960, 16 cases of papillary cystadenoma (2.0%) have been reported
(3). Due to the rarity of papillary
cystadenoma, the cytological features of the lesion have not been
well described in textbooks and other publications. The cytological
findings of a reported case of papillary cystadenoma from a minor
salivary gland revealed cohesive groups of epithelial cells
demonstrating a complex folded appearance in a cystic proteinaceous
background, and the possibility of salivary gland tumors was raised
in the fine needle aspiration diagnosis (9). Nasuti et al (10) reported that the aspiration material
was insufficient in the papillary oncocytic cystadenoma.
Microscopically, it has been revealed that the
tumors are generally well circumscribed and surrounded by fibrous
capsules. Although the extent of solid regions is usually limited,
there are cystic regions into which papillae lined by two layers of
cuboidal to columnar cells usually project (11). In the majority of cases, the
multilocular individual cystic space is separated by a limited
amount of interstitial intervention. Lumens, in numerous cases,
contain eosinophilic material with scattered epithelial,
inflammatory or foamy cells. Oncocytic, mucus, epidermoid and
apocrine cells are occasionally present locally, or may be
predominant. Oncocytic variants of cystadenomas predominantly
consist of oncocytes in a unilayered or two-layer papillary
structure, similar to the epithelium of Warthin tumors, but without
lymph stroma.
Therefore, papillary cystadenoma closely resembles
Warthin tumors, but the present case was distinguished from Warthin
tumors by the almost complete lack of lymphoid follicles. Sections
of the lesion revealed multiple small cystic spaces or a single
large cyst surrounded by lobules of salivary gland or connective
tissue. Although the focal variation in epithelial differentiation
is typical, a single cystadenoma, a single cell type, is
characteristically dominant. Auclair et al (12) identified the oncocytic differentiation
in 16% of the cases of papillary cystadenomas assessed.
During differential diagnosis, it may be challenging
to distinguish between papillary cystadenoma and
cystadenocarcinoma, as the tumors demonstrate similar structures
(13). The two tumors usually
demonstrate papillary proliferation of the epithelial layer, which
is composed of cells which possess ‘bland-looking’ nuclei (5).
Commonly, cystadenoma is treated by simple excision,
and recurrence is not observed (4).
However, Skorpil (14) and Collins
(15) have each reported cases that
experienced recurrence.
However, a lack of evidence of locally devastating
behavior, the relative quiescence of the tumors, which results in
the tumors often being found incidentally, histological evidence of
a well-circumscribed tumor lacking mitoses and atypia, and the
notable failure of any of these tumors to metastasize all prevent
the suggestion of malignant potential. Therefore, it is likely that
recurrences are attributable to incomplete resection or possibly
due to a misdiagnosis of a low-grade cystadenocarcinoma (11). For these reasons, the present patient
is followed-up at regular intervals, and a similar management plan
is recommended for all patients that are diagnosed with papillary
cystadenoma.
References
|
1
|
Thackeray AC and Sabin LH: Adenoma.
Histological Typing of Salivary Gland Tumors (Switzerland). World
Health Organization Geneva. 221972.
|
|
2
|
Seifert G: Adenoma. Histological Typing of
Salivary Gland Tumors (2nd). (Berlin Germany). Springer-Verlag.
16–17. 1991.
|
|
3
|
Tsurumi K, Kamiya H, Yokoi M and Kameyama
Y: Papillary oncocytic cystadenoma of palatal minor salivary gland,
A case report. J Oral Maxillofac Surg. 61:631–633. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sher L: The papillary cystadenoma of
salivary gland origin. Diastema. 10:37–41. 1982.PubMed/NCBI
|
|
5
|
Chin S, Kim HK and Kwak JJ: Oncocytic
papillary cystadenoma of major salivary glands, Three rare cases
with diverse cytologic features. J Cytol. 31:221–223. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Leon B, Eveson JW, Reichart P and
Sidransky D: Tumours of the salivary glands. Pathology &
Genetics of Head and Neck Tumors (Lyon). IARC Press. 2732005.
|
|
7
|
Toida M, Shimokawa K, Makita H, Kato K,
Kobayashi A, Kusunoki Y, Hatakeyama D, Fujitsuka H, Yamashita T and
Sibata T: Intraoral minor salivary gland tumors, A
clinicopathological study of 82 cases. Int J Oral Maxillofac Surg.
34:528–532. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Chaudhry AP, Vickers RA and Gorlin RJ:
Intraoral minor salivary gland tumors: An analysis of 1,414 cases.
Oral Surg Oral Med Oral Pathol. 14:1194–1226. 1961. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lim CS, Ngu I, Collins AP and McKellar GM:
Papillary cystadenoma of a minor salivary gland, Report of a case
involving cytological analysis and review of the literature. Oral
Surg Oral Med Oral Pathol Oral Radiol Endod. 105:e28–e33. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Nasuti JF, Gupta PK, Fleisher SR and
LiVolsi VA: Nontyrosine crystalloids in salivary gland lesions,
Report of seven cases with fine-needle aspiration cytology and
follow-up surgical pathology. Diagn Cytopathol. 22:167–171. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Alexis JB and Dembrow V: Papillary
cystadenoma of a minor salivary gland. J Oral Maxillofac Surg.
53:70–73. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Auclair PL, Ellis GL and Gnepp DR: Other
benign epithelial neoplasms. Surgical Pathology of the Salivary
Glands. Ellis GL, Auclair PL and Gnepp DR: (Philadelphia, PA). WB
Saunders Company. 2522008.
|
|
13
|
Foss RD, Ellis GL and Auclair PL: Salivary
gland cystadenocarcinomas. Histopathology. Am J Surg Pathol.
20:1440–1447. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Skorpil F: Uber dasC ystadenoma papillare
der grossen und Kleinen Speicheldrusen. Frankfurt Ztschr Path.
55:391941.
|
|
15
|
Collins EM: Papillary cystadenoma of
accessory salivary gland. Am J Surg. 96:749–750. 1958. View Article : Google Scholar : PubMed/NCBI
|