Introduction
Bronchogenic cysts (BC) occurring in the head and
neck region were first reported by Park and Buford (1) in 1955. The cysts usually appear in the
mediastinum and chest of infants and children, but they seldom
occur in adults, particularly in elderly individuals (2–4). The ratio
of males to females diagnosed with congenital cysts is 4:1
(5). According to their location, BC
can be divided into intrathoracic or extrathoracic BC. Based on
this foundation, Maier (6) further
classified BC into five groups: The carinal, paratracheal, hilar,
paraesophageal and atypical groups. BC of the cervical region
belongs to the atypical group. BCs are easily confused with third
or fourth branchial cleft cysts, particularly when the lesions
occur in the root of cervical region accompanied by deep neck
abscesses (2,3). Considering the recurrence of cysts
following incomplete excision and the possibility of malignant
biological behavior, a complete resection is the optimal method for
the treatment of BC. The current study reports the case a
70-year-old female who presented with a painful mass in the right
cervical region, and also provides a review of the literature.
Case report
In August 2012, a 70-year-old female presented to
the Ninth People's Hospital (College of Stomatology, Shanghai Jiao
Tong University School of Medicine, Shanghai, China) with a painful
mass in the right cervical region that had been apparent for one
month. There had been no mass in the area prior to the appearance
of the clinical symptoms. A physical examination found a soft,
smooth, tender, unmovable cystic mass, ~4.0 cm in diameter, below
the right thyroid gland. No fistulae or scars on the skin were
detected. Slight mobility was discovered during patient
aspiration.
Ultrasound examination showed a 46×31-mm, mixed
echoic cystic mass below the right thyroid gland tissue, with a
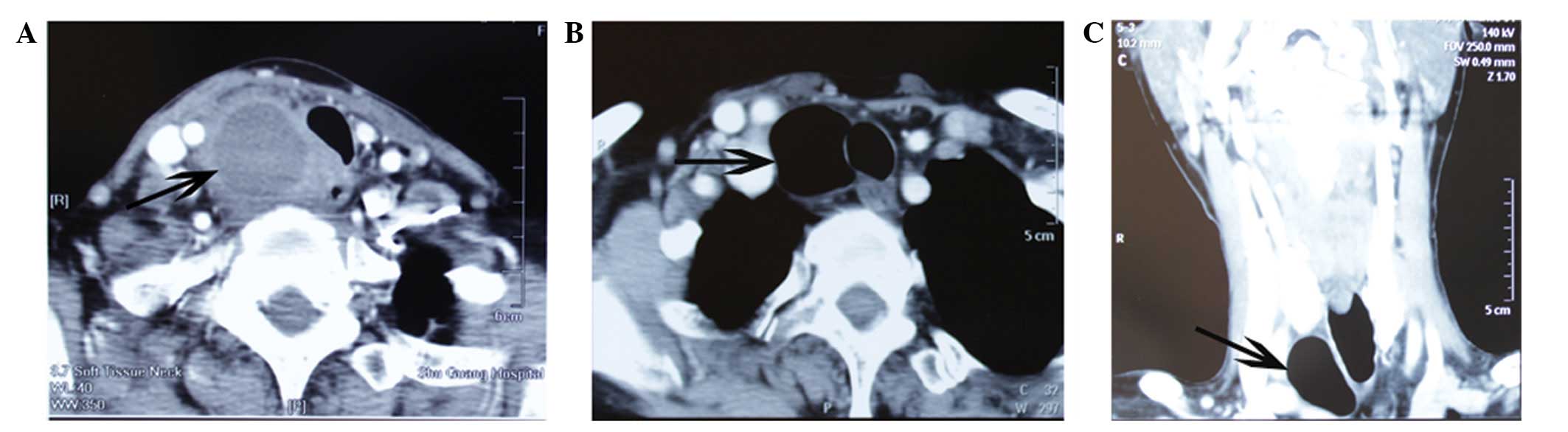
clear border. Computed tomography (CT) scans confirmed the presence
of a 3.3×3.0-cm hypodense cystic mass with regular margins located
in the right cervical region. A left shift of the trachea was also
observed due to compression by the cyst (Fig. 1A). The pre-operative diagnosis was of
a branchial cleft cyst accompanied by infection. Antibiotics
(cefoxitin sodium, injected at a dose of 2 g/day for 3 days) were
applied prior to the surgery due to symptoms of inflammation.
Repeat CT showed a 2.9×2.8-cm oval mass of gaseous density, with a
C value of −988 HU. Only a thin septum, without evident perforation
between the mass and trachea, was observed by CT (Fig. 1B–C); this showed the elimination of
inflammation and the real nature of the disease.
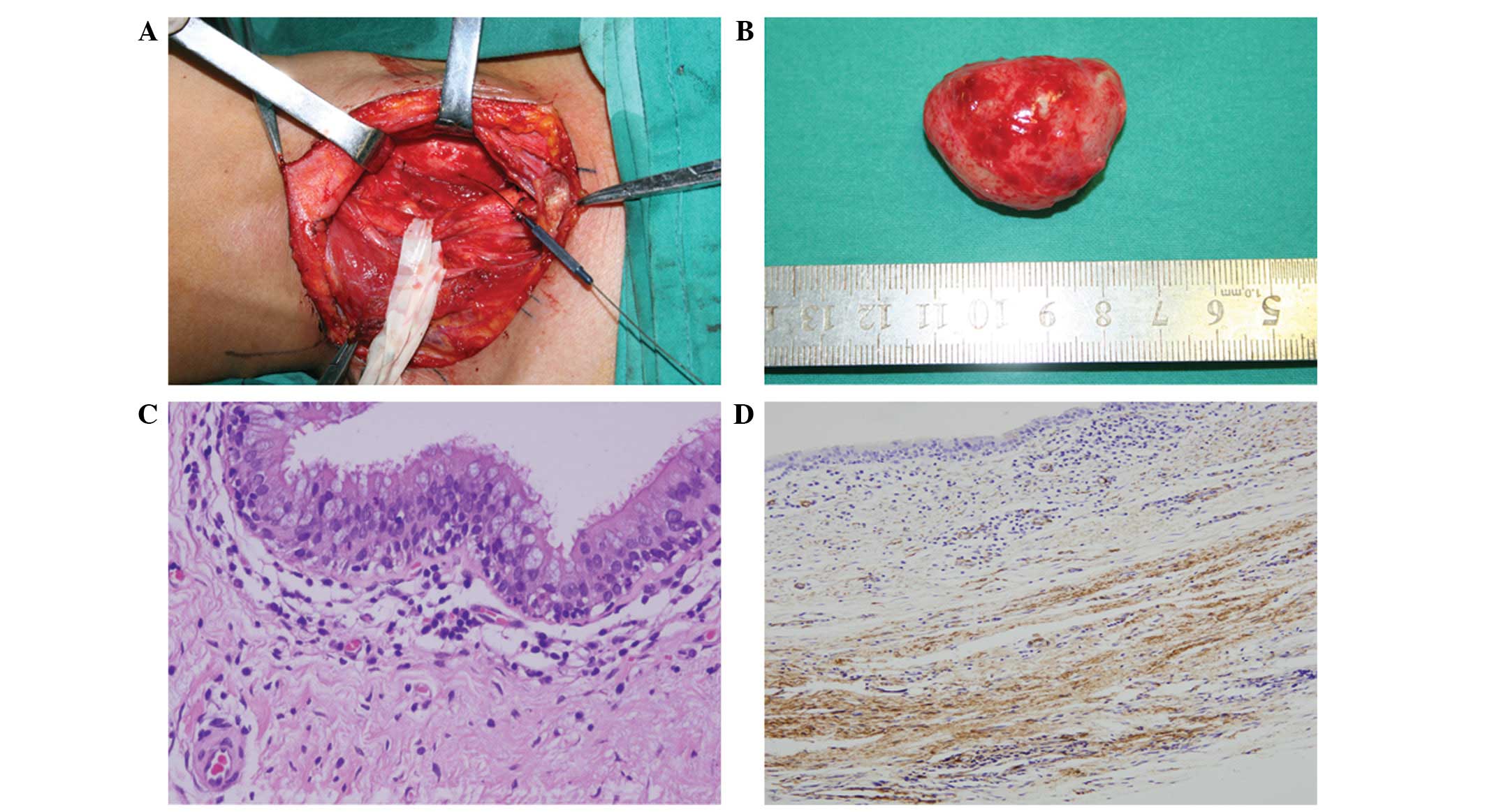
Surgery was performed when inflammation subsided
after antibiotic treatment. A rounded mass filled with air was
detected attached to the right trachea with a short fibrous duct
during the surgery. After complete resection with clear margins,
the mass was able to return to its original shape following
extraction of the air content, which was performed using a 10-ml
injector (Fig. 2A and B). The gross
pathology revealed a unilocular cyst filled with gas.
Microscopically, the lining of the cyst was pseudostratified
cilliated columnar epithelium accompanied by scattered mucous
metaplastic cells (Fig. 2C). Smooth
muscle was found in the cyst wall, while cartilage was not observed
(Fig. 2D). The histological diagnosis
was of a BC accompanied by infection. The patient was followed up
for 34 months, without experiencing any discomfort or
recurrence.
Discussion
BCs are congenital cystic lesions arising from
aberrated budding of the ventral foregut, which takes place during
the gestation period (7). The
deformity of the ventral foregut may occur in different phases of
embryogenesis, with the result of the formation of BC in various
positions. If the aberrated buddings arise in the initial stage of
embryogenesis, it may lead to the BC being located along the
tracheobronchial system, which differs from BC located in the
mediastinum or lung parenchyma, due to malformations in development
in the late stages (8,9). BCs in the midline of the neck may have
an intimate association with the development stage of the trachea
during which the abnormal buddings occur, while cysts may be
localized in the lower and lateral neck due to malformed
development of the bronchial system (10).
BCs may present as asymptomatic cystic lesions in
the head and neck region, with extremely low morbidity rates in
elderly individuals, particularly elderly females (2–5). The size
of the BC does not go unchanged and may enlarge with body growth.
Disimilar to other studies, the case reported in the present study
exhibited no evident mass or discomfort in the right neck during
the 70 years prior to the onset of illness. It therefore remains
uncertain as to how congenital disease occurs in elderly patients.
Infection is not usually apparent in BC according to the cases
previously reported in the literature (3). Cyst infections are usually caused by the
communication of the cyst with the tracheal-bronchus system through
fibrous connections, which may not be easily observed by CT or
magnetic resonance imaging until during surgery (11). It has been reported that in adults,
BCs of the thyroid and paratracheal region may be more likely to be
infected compared with those in the supraclavicular and
suprasternal notch (12). With regard
to the present study, the patient suffered from local radioactive
soreness or general infectious symptoms due to cyst infection. This
infection could be easily observed in the third or fourth branchial
cleft cysts, located in the root of the neck, and were
characterized by local, recurrent deep abscesses.
Various types of image can be presented by CT
examinations of BC, including homogeneous density, fluid and
air-liquid level masses. BC filled with air only, as observed in
the present study, is extremely rare. Air-filled lesions may be
observed on CT images when communication exists between the cyst
and the tracheal-bronchus system (13). Bacteria can make best use of this
narrow pathway to enter the cysts, which results in local or
general infection, thus forming a deep abscess. In the present
case, successive CT images are shown prior to and following
anti-inflammatory therapy. In the inflammatory stage, the lesion
presented with a heterogeneous hypodense cystic image, while after
antibiotic treatment it became an image of a mass with gaseous
density. There are no particular CT standards to distinguish BCs
from other cysts.
BCs are characteristically lined by pseudostratified
ciliated columnar epithelium, while squamous metaplasia,
inflammation or totally necrotic tissues may be found when there
has been previous infection (14,15). The
cyst wall may be comprised of cartilage, mucus-secreting goblet
cells, fibrous connective tissue and smooth muscle, which may
contribute to the cyst contraction, as observed in the present
case. The majority of these components may easily be observed in
intrathoracic BC, but are rarely found in cervical BC. In the
analysis of cutaneous BC, a previous study reported that smooth
muscle was most likely to be found at a ratio of 70%, followed by
57% glandular cells and 19% cartilage (16). It is really difficult to distinguish
BC from branchial cleft cysts. Branchial cleft cysts usually appear
in the upper triangle of the neck followed by the lateral neck,
while BCs commonly occur in one side of the neck, with few cases
reported in the upper cervical region (17). Therefore, the location of lesions
cannot be used to form a definitive diagnosis. Branchial cleft
cysts are typically lined with squamous epithelium, but scattered
pseudostratified ciliated columnar epithelium may not be excluded.
It is difficult to distinguish between BCs and branchial cleft
cysts when relying solely on the histopathology. The clinical
symptoms and histopathology manifestations should be additionally
assessed to improve the distinction.
BCs are benign tumors in the majority of cases,
although they may have an intimate connection with malignant
tumors. When considering the potential risk of cyst recurrence and
its complications, such as opportunistic infections and hemorrhage,
a complete surgical resection of the BC should be recommended,
particularly in elderly patients.
In conclusion, BCs are rare congenital lesions that
seldom occur in the oromaxillofacial-head and neck region of
elderly females, with few cases reported in the literature. The
case described in the present study showed that congenital
diseases, such as BC, may also appear in elderly individuals
without clinical manifestations. It is a challenge for head and
neck surgeons to form a correct differential diagnosis for BC and
other cystic lesions, thus acquiring preferable therapeutic
effects.
Acknowledgements
This study was supported by generous grants from the
National Natural Science Foundation of China (no. 81271112), the
Shanghai Municipal Human Resources and Social Security Bureau (no.
201312), SMC Rising Star (A) Scholar, supported by Shanghai Jiao
Tong University.
References
|
1
|
Park OK and Buford CH: Bronchogenic cyst
of neck and superior mediastinum. Ann Surg. 142:130–133. 1955.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Al-kasspooles MF, Alberico RA, Douglas WG,
Litwin AM, Wiseman SM, Rigual NR, et al: Bronchogenic cyst
presenting as a symptomatic neck mass in an adult: case report and
review of the literature. Laryngoscope. 114:2214–2217. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hazenberg AJ, Pullmann LM, Henke RP and
Hoppe F: Recurrent neck abscess due to a bronchogenic cyst in an
adult. J Laryngol Otol. 124:1325–1328. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wilkinson N, Reid H and Hughes D:
Intradural bronchogenic cysts. J Clin Pathol. 45:1032–1033. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pul N and Pul M: Bronchogenic cyst of the
scapular area in an infant: case report and review of the
literature. J Am Acad Dermatol. 31:120–122. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Maier HC: Bronchiogenic cysts of the
mediastinum. Ann Surg. 127:476–502. 1948. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Chapman KR and Rebuck AS: Spontaneous
disappearance of a chronic mediastinal mass. Chest. 87:235–236.
1985. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Di Lorenzo M, Collin PP, Vaillancourt R
and Duranceau A: Bronchogenic cysts. J Pediatr Surg. 24:988–991.
1989. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
St-Georges R, Deslauriers J, Duranceau A,
Vaillancourt R, Deschamps C, Beauchamp G, et al: Clinical spectrum
of bronchogenic cysts of the mediastinum and lung in the adult. Ann
Thorac Surg. 52:6–13. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ustundag E, Iseri M, Keskin G, Yayla B and
Muezzinoglu B: Cervical bronchogenic cysts in head and neck region.
J Laryngol Otol. 119:419–423. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kostopoulos G, Efstathiou A, Skordalaki A
and Fessatidis I: Bronchogenic cyst infected by Salmonella
enteritidis followed gastroenteritis. Eur J Cardiothorac Surg.
21:935–937. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Moz U, Gamba P, Pignatelli U, D'Addazio G,
Zorzi F, Fiaccavento S and Milesi F: Bronchogenic cysts of the
neck: a rare localization and review of the literature. Acta
Otorhinolaryngol Ital. 29:36–40. 2009.PubMed/NCBI
|
|
13
|
Touloukian RJ: Air filled bronchogenic
cyst presenting as a cervical mass in the newborn. J Pediatr Surg.
17:311–312. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Newkirk KA, Tassler AB, Krowiak EJ and
Deeb ZE: Bronchogenic cysts of the neck in adults. Ann Otol Rhinol
Laryngol. 113:691–695. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Mehta RP, Faquin WC and Cunningham MJ:
Cervical bronchogenic cysts, a consideration in the differential
diagnosis of pediatric cervical cystic masses. Int J Pediatr
Otorhinolaryngol. 68:563–568. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zvulunov A, Amichai B, Grunwald MH,
Avinoach I and Halevy S: Cutaneous bronchogenic cyst, delineation
of a poorly recognized lesion. Pediatr Dermatol. 15:277–281. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Shimazu R, Kuratomi Y and Inokuchi A: A
case of an upper cervical bronchogenic cyst in an adult. Auris
Nasus Larynx. 33:351–353. 2006. View Article : Google Scholar : PubMed/NCBI
|