Introduction
Carcinoma showing thymus-like differentiation of the
thyroid (CASTLE) is a rare intrathyroidal neoplasm, which may arise
from ectopic thymus tissue or branchial pouch remnants (1). Chan and Rosai (2) classified the clinicopathological
features of CASTLE into four types: i) Ectopic hamartomatous
thymoma; ii) ectopic cervical thymoma; iii) spindle epithelial
tumor with thymic-like differentiation; iv) and CASTLE. At present,
CASTLE is considered an independent clinicopathological entity of
thyroid tumors, according to the World Health Organization
classification of tumors of endocrine organs (3). To the best of our knowledge, solely 3
patients have presented with CASTLE at Nanjing Drum Tower Hospital
(The Affiliated Hospital of Nanjing University Medical School;
Nanjing, China) to date. Due to the rarity of CASTLE, there is
currently no unified standard method of diagnosis or therapy
(1). In 2013, Huang et al
(4) summarized 45 cases of CASTLE
identified in China. To fully understand this disease, a search of
the relevant literature in Pubmed and Chinese databases was
performed in the present study, which identified a total of 82
cases of CASTLE reported to date. These cases are summarized in the
present study, and recommendations for the diagnosis and treatment
of CASTLE are suggested.
Materials and methods
Database search
Electronic searches of the PubMed (www.ncbi.nlm.nih.gov/pubmed), China National
Knowledge Infrastructure (www.global.cnki.net/kns50/single_index.aspx) and
Ten Thousand databases (http://g.wanfangdata.com.cn) were performed using the
following key words: Thyroid, thymus and carcinoma. A total of 82
patients with CASTLE were identified, and their clinical
characteristics, diagnosis, treatment, pathology and follow-up were
reviewed.
Review of preoperative
examinations
The results of preoperative examinations, including
ultrasound (n=57), computed tomography (CT; n=27), emission CT
(ECT; n=10), thyroid function (n=52) and fine-needle aspiration
cytology (n=24), were reviewed. Histopathological examination of
surgical specimens was performed using standard hematoxylin and
eosin staining (H&E), alongside specific immunohistochemical
techniques. The primary immunohistochemical markers were cluster of
differentiation (CD)5, CD117, cytokeratin (CK), CK19, CK AE1/AE3,
tumor protein (TP)63, carcinoembryonic antigen (CEA),
synaptophysin, B-cell lymphoma 2, epithelial membrane antigen
(EMA), chromogranin A, calcitonin (CT), thyroglobulin (TG) and
thyroid transcription factor-1 (TTF-1). All images are of a single
patient and are representative of all patients analyzed.
Statistical analysis
The χ2 test was used to evaluate the
effects of lymph node metastasis and radiotherapy on recurrence.
P<0.05 was considered to indicate a statistically significant
difference. All P-values were two-sided. All statistical
calculations were performed using SPSS software version 19.0 (IBM
SPSS, Armonk, NY, USA).
Results
Baseline characteristics demonstrated
wide variations
Of the 82 cases reviewed in the present study, 59
patients were Chinese, 11 were Japanese, 9 were American, 1 was
Italian, 1 was Korean and 1 was Portuguese. A total of 37 patients
were males and 45 were females. The male:female ratio was 1:1.22.
The average patient age was 48.8±12.8 years (range, 25–79 years).
The patients presented with a range of symptoms, including a neck
tumor in 40 cases (48.78%), hoarseness in 13 patients (15.85%),
dyspnea in 8 patients (9.76%), cough in 3 patients (3.66%), neck
pain in 3 patients (3.66%) and dysphagia in 1 patient (1.22%). For
14 patients (17.07%), the symptoms were unknown. A total of 34
CASTLE tumors were located in the left lobe of the thyroid, 44 were
in the right lobe and 3 were bilateral. In 1 patient, the location
of the tumor was unknown. The location of the tumor was more
specifically described in 50 cases, of which, 47 presented the
tumor in the lower part of the thyroid and 3 in the upper part. The
baseline characteristics of the patients are summarized in Table I.
 | Table I.Clinical characteristics of 82
patients with carcinoma showing thymus-like differentiation of the
thyroid. |
Table I.
Clinical characteristics of 82
patients with carcinoma showing thymus-like differentiation of the
thyroid.
| Parameter | Number of
patients | Percentage |
|---|
| Country |
|
|
|
China | 59 | 71.95 |
|
Japan | 11 | 13.41 |
|
America | 9 | 10.98 |
|
Italy | 1 | 1.22 |
|
Korea | 1 | 1.22 |
|
Portugal | 1 | 1.22 |
| Age, years |
|
|
|
<40 | 23 | 28.05 |
|
40–60 | 40 | 48.78 |
|
>60 | 19 | 23.17 |
| Gender |
|
|
| Male | 37 | 45.12 |
|
Female | 45 | 54.88 |
| Symptom |
|
|
| Neck
tumor | 40 | 48.78 |
|
Hoarseness | 13 | 15.85 |
|
Dyspnea | 8 | 9.76 |
|
Cough | 3 | 3.66 |
| Neck
pain | 3 | 3.66 |
|
Dysphagia | 1 | 1.22 |
|
Unknown | 14 | 17.07 |
| Thyroid location |
|
|
| Left
lobe | 34 | 41.46 |
| Right
lobe | 44 | 53.66 |
| Bilateral
lobe | 3 | 3.66 |
|
Unknown | 1 | 1.22 |
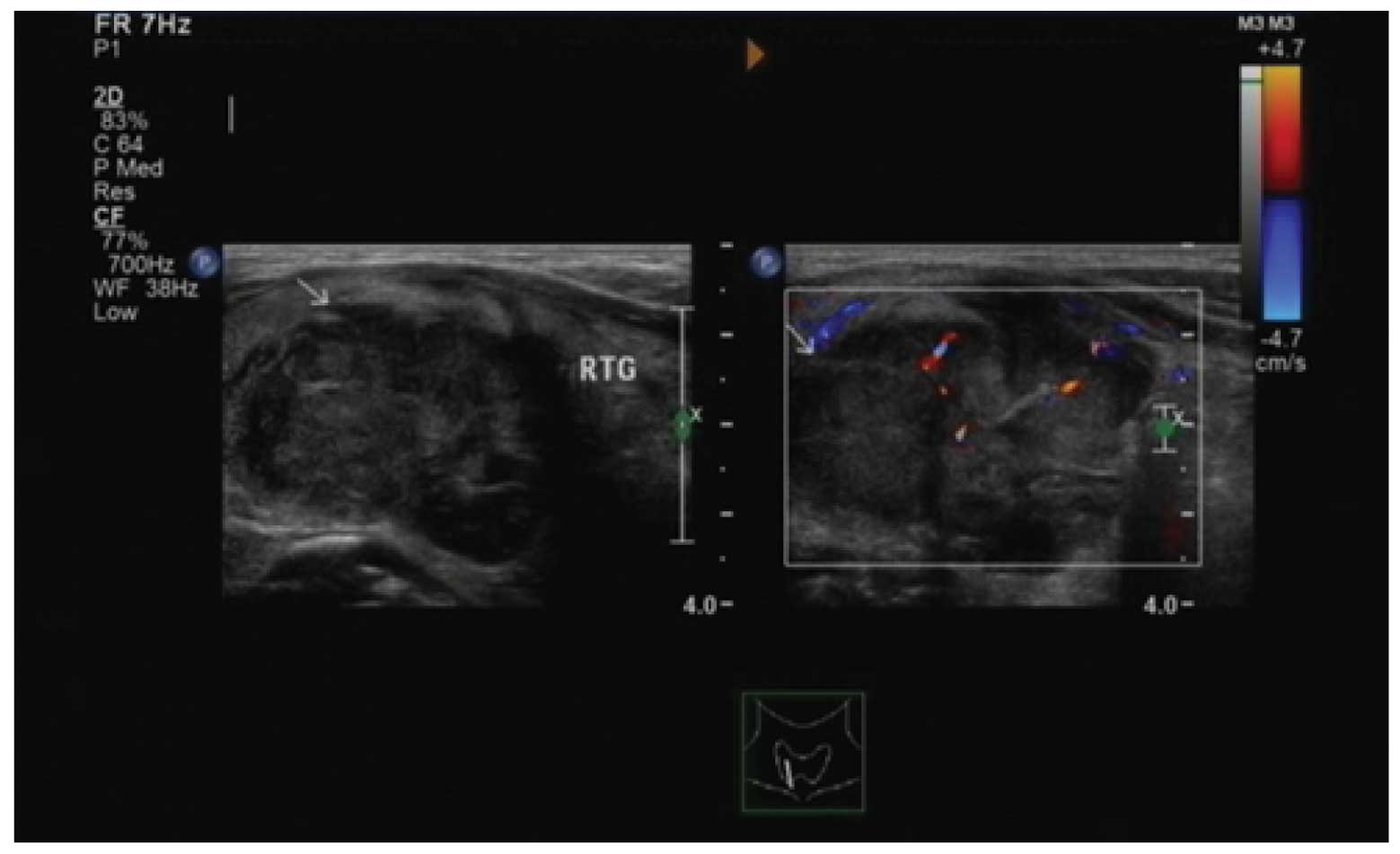
Preoperative examinations varied from
patient to patient
In the present study, descriptions of ultrasound
examination were recorded for 57 patients, whose CASTLE was
typically described as a solid and hypoechoic mass with
heterogeneous echo (Fig. 1). Results
of ECT in 10 patients were acquired in the present study, and all
tumors were described as ‘cold nodule’. CT examination in 27
patients revealed that CASTLE was a well-defined, soft tissue
density mass without calcification, and the mass appeared enhanced
following administration of contrast medium. A total of 52 patients
underwent a test of thyroid function. Of these, 51 cases were
normal and 1 exhibited hyperthyroidism. A total of 24 patients
underwent fine-needle aspiration cytology. Of these, 2 patients
were diagnosed with CASTLE, 17 cases were demonstrated to be
malignant tumors, 1 case was hyperplasia and the remaining 4 cases
were negative.
Treatment and follow-up demonstrated
wide variations across patients
Of the 81 patients who had undergone surgery, lymph
node metastasis was observed in 22 patients, and distant metastasis
to the lung was identified in 2 patients. Postoperative radiation
was administered as an adjuvant therapy in 29 patients, while 4
patients received chemotherapy in addition to radiation. The median
follow-up time was 14 months (range, 1–312 months), and no
follow-up period was reported for 15 patients. Of the 78 patients
who had undergone radical surgery, 12 experienced recurrence, with
a median time to recurrence of 11 months (range, 1–144 months;
Table II). The effect of lymph node
metastasis and radiotherapy on recurrence was subsequently
evaluated by χ2 test using SPSS software version 19.0
(Table III).
| Table II.Follow-up of 12 patients exhibiting
carcinoma showing thymus-like differentiation of the thyroid who
experienced recurrence. |
Table II.
Follow-up of 12 patients exhibiting
carcinoma showing thymus-like differentiation of the thyroid who
experienced recurrence.
| Authors | Time until
recurrencea, months | Treatment | Follow-up
timea, months | Outcome |
|---|
| Liu et al
(6) | 144 | Surgery | 27 | NED |
| Liu et al
(6) | 22 | Surgery | 44 | NED |
| Bai et al
(7) | 22 | Surgery and
radiotherapy | 50 | NED |
| Pan et al
(8) |
3 | Surgery, radiotherapy
and chemotherapy | 12 | NED |
| Luo et al
(9) | 24 | Surgery, radiotherapy
and chemotherapy |
6 | NED |
| Wu et al
(10) |
1 | Radiotherapy | 25 | NED |
| Da et al
(11) |
6 | Surgery | 108 | NED |
| Da et al
(11) |
6 | Surgery | 132 | NED |
| Da et al
(11) |
3 | Unknown | 36 | SD |
| Reimann et al
(13) | 72 | Radiotherapy | 96 | SD |
| Reimann et al
(13) | 36 | Surgery | 96 | NED |
| Tsutsui et al
(12) | 16 | Surgery | 34 | NED |
| Table III.Effect of lymph node metastasis and
radiotherapy on recurrence. |
Table III.
Effect of lymph node metastasis and
radiotherapy on recurrence.
| Parameter | Recurrence | No recurrence | χ2
value | P-value |
|---|
| Lymph node
metastasis |
|
| 1.482 | 0.144 |
|
Present | 6 | 13 |
|
|
|
Absent | 3 | 22 |
|
|
| Radiotherapy |
|
| 0.000 | 1.000 |
|
Present | 4 | 25 |
|
|
|
Absent | 3 | 16 |
|
|
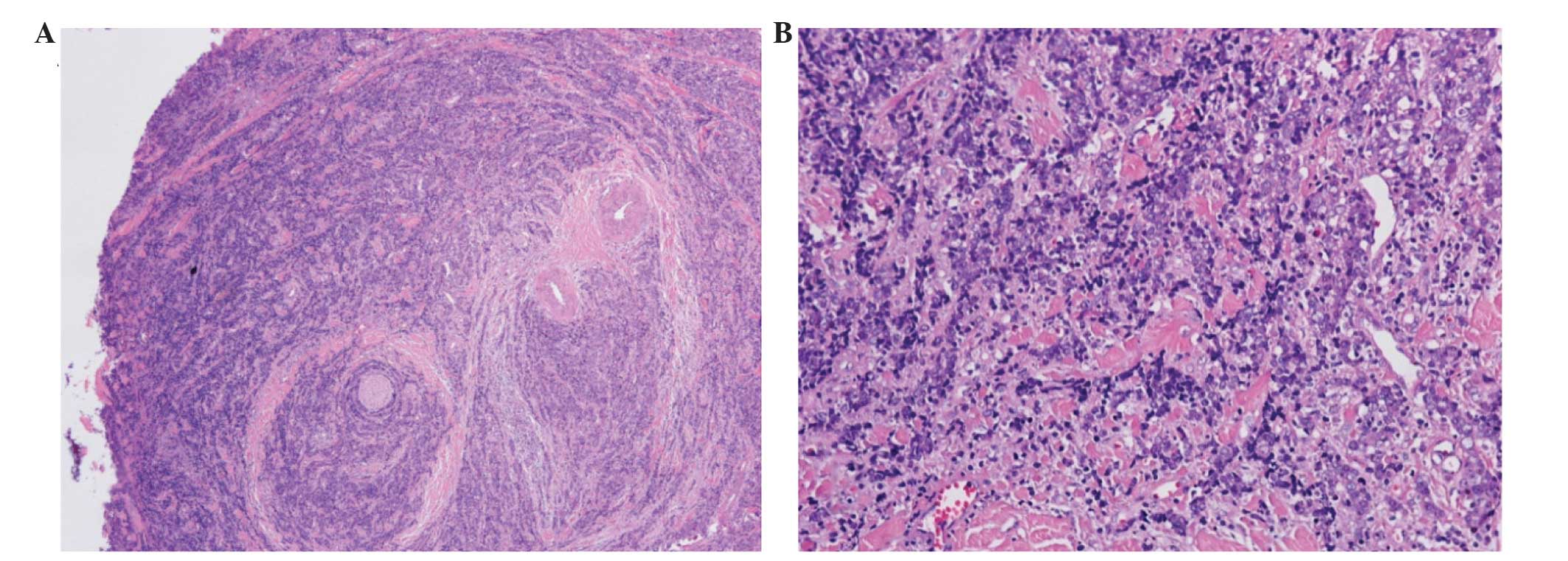
Pathological and immunohistochemical
examinations confirmed positivity for certain markers
Microscopic examination revealed the presence of
confluent nests and lobules of various glands with a few
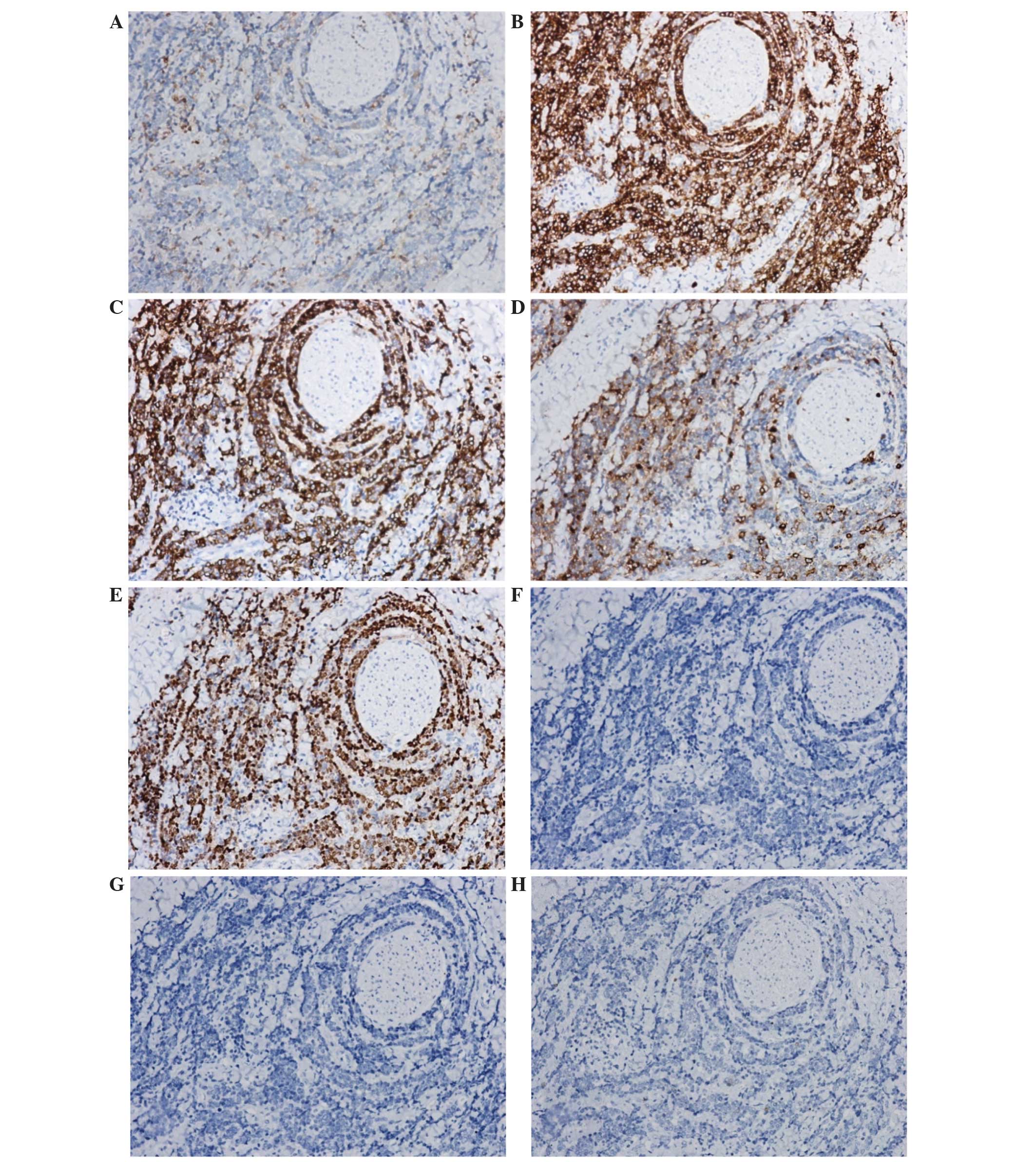
lymphocytes and plasma cell infiltration (Fig. 2). The immunohistochemical results are
summarized in Table IV. Typical
immunohistochemical examinations demonstrated positivity for CD5,
CD117, CK19, EMA and TP63, and negativity for CT, TG and TTF-1
(Fig. 3).
| Table IV.Immunohistochemical results of 82
cases of carcinoma showing thymus-like differentiation of the
thyroid. |
Table IV.
Immunohistochemical results of 82
cases of carcinoma showing thymus-like differentiation of the
thyroid.
| Immunological
marker | Number of cases
studied | Number of positive
cases | Percentage |
|---|
| CD5 | 63 | 63 | 100.00 |
| CK | 19 | 10 |
52.63 |
| CD117 | 37 | 36 |
97.30 |
| CK19 | 14 | 14 | 100.00 |
| Tumor protein
63 | 32 | 32 | 100.00 |
| Carcinoembryonic
antigen | 25 | 16 |
64.00 |
| Synaptophysin | 19 | 5 |
26.32 |
| CK AE1/AE3 | 11 | 11 | 100.00 |
| B-cell lymphoma
2 | 14 | 14 | 100.00 |
| Epithelial membrane
antigen | 7 | 5 |
71.43 |
| Chromogranin A | 9 | 2 |
22.22 |
| Thyroglobulin | 55 | 0 |
0.00 |
| Calcitonin | 35 | 0 |
0.00 |
| Thyroid
transcription factor-1 | 51 | 0 |
0.00 |
Discussion
CASTLE is a rare, indolent and slow-growing
malignant neoplasm of the thyroid gland, which was initially
reported by Miyauchi et al in 1985 (5). According to the relevant literature, and
to the best of our knowledge, 82 cases of CASTLE have been reported
thus far, primarily in the form of case reports. The present study
summarized the clinical characteristics of all the cases of CASTLE
published to date in the relevant literature. The male:female ratio
was 1:1.22, and the average patient age was 48.8±12.8 years (range,
25–79 years). The clinical manifestations of CASTLE varied across
the patients, and were not specific. The majority of previous
reports have described CASTLE tumors involving predominantly the
lower part of the thyroid, which may be due to CASTLE originating
from ectopic thymic tissue or branchial pouch remnants in or
adjacent to the thyroid (2,14).
The preoperative diagnosis of thyroid tumors relies
on ultrasound, ECT, CT, thyroid function and fine-needle aspiration
cytology (1,6–11). In the
present study, ultrasound imaging of CASTLE identified a solid and
hypoechoic mass, whose echo was typically heterogeneous. Yamamoto
et al (15) studied the
sonographic findings in three cases of CASTLE and concluded that
CASTLE was solid and hypoechoic, with a heterogeneous echo pattern
and without cystic components or calcifications, which is in
agreement with the results of the present study. CASTLE was
previously described as ‘cold nodule’ in ECT, suggesting that it
was a malignancy (1). In CT, CASTLE
was revealed as a well-defined, soft tissue density mass without
calcification, and the mass appeared enhanced following
administration of contrast medium (16,17). Tests
of thyroid function were normal in almost all the CASTLE cases
analyzed, suggesting that CASTLE did not affect the thyroid
function (1). A total of 24 patients
underwent fine-needle aspiration cytology. Of these, 2 were
diagnosed with CASTLE, thus indicating that fine-needle aspiration
cytology contributed to the primary diagnosis of CASTLE, while its
exact diagnosis depended on pathological and immunohistochemical
examination. However, due to the false-negative rates exhibited by
fine-needle aspiration cytology, the results should be interpreted
with caution, and the examination repeated if required (18).
The preoperative diagnosis of CASTLE is difficult,
and conclusive diagnosis often relies on pathological examination,
particularly immunohistochemistry (1). A number of studies have indicated that
CD5 may be a useful marker for the diagnosis of CASTLE, as it is a
marker for carcinoma of thymic origin (19,20).
Similar to thymic carcinoma, CASTLE is immunohistochemically
positive for CD5, but negative for CT, TG and TTF-1 (19). Ito et al (21) reported a sensitivity and specificity
of 82 and 100%, respectively, for CD5 positivity for the diagnosis
of CASTLE. In the present study, 63 patients underwent CD5 testing
and all demonstrated positivity for this marker, while all the
cases tested demonstrated negativity for CT, TG and TTF-1. However,
since a lack of CD5 expression does not completely rule out CASTLE,
the final diagnosis was based on H&E findings. A previous study
reported that expression of high molecular weight CK, CEA and TP63
in CASTLE provided evidence of the thymic origin of the tumor, and
were useful diagnostic markers for distinguishing thyroid CASTLE
from other thyroid neoplasms (13).
In the present study, the positive rates for CK19, CEA and TP63
were 100.00, 64.00 and 100.00%, respectively. Reimann et al
(13) reported that the majority of
nuclei stained positively for TP63 in 11/11 thyroid solid cell
nests, 7/7 CASTLEs, 10/10 thymic carcinomas and 23/23 thymomas. In
the present study, TP63 was examined in 32 patients and all cases
proved to be positive. In addition, CD117 may be a useful maker for
distinguishing CASTLE from other thyroid tumors, since the results
of the present study demonstrated a positive rate for CD117
expression of 97.30%.
In the present study, 81 patients underwent surgery.
Lymph node metastasis was observed in 22 patients, however, only 19
patients with lymph node metastasis completed follow-up.
Postoperative radiation was administered as an adjuvant therapy to
28 patients, and 4 patients received chemotherapy in addition to
radiation. Of the 78 patients who had undergone radical surgery, 12
experienced recurrence. The present study evaluated the effects of
lymph node metastasis and radiotherapy on recurrence. The results
demonstrated that lymph node metastasis did not promote recurrence
following radical surgery (P=0.144), and postoperative radiation
was not able to reduce the recurrence rate (P=1.000). By contrast,
Roka et al (22) reported that
node-negative CASTLE presented a low risk of recurrence, and that
curative surgery of the tumor with resection of the adjacent organs
involved in addition to systematic dissection of the lymph nodes,
followed by radiation therapy, was able to prevent locoregional
recurrence. Therefore, the findings of the present study require
further confirmation, due to the limited sample size of the
study.
The prognosis of CASTLE is relatively positive
(12). In the present study, the
recurrence rate was 18.57% (13/70 patients). During follow-up, 4
patients were reported to succumb to disease, and the longest
follow-up time of these 4 patients was 26 years.
In conclusion, thyroid CASTLE is a rare malignancy
of the thyroid gland that may display various manifestations.
Preoperative examinations, including CT, ECT and ultrasound, may
not be capable of establishing an exact diagnosis, which typically
requires pathological examination, particularly immunohistochemical
results. Radical resection is the primary treatment for CASTLE, and
the prognosis for this disease is favorable following surgery.
Postoperative radiation appears to be unable to reduce the
recurrence rate in patients with CASTLE.
References
|
1
|
Liu Z, Teng XY, Sun DX, Xu WX and Sun SL:
Clinical analysis of thyroid carcinoma showing thymus-like
differentiation: Report of 8 cases. Int Surg. 98:95–100. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chan JK and Rosai J: Tumors of the neck
showing thymic or related branchial pouch differentiation: A
unifying concept. Hum Pathol. 22:349–367. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
DeLellis RA, Lloyd RV, Heitz PU and Eng C:
Parathyroid carcinoma. World Health Organization Classification of
Tumours. Pathology and Genetics of Tumors of Endocrine Organs.
96:(Lyon). IARC Press. 124–127. 2004.
|
|
4
|
Huang C, Wang L, Wang Y, Yang X and Li Q:
Carcinoma showing thymus-like differentiation of the thyroid
(CASTLE). Pathol Res Pract. 209:662–665. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Miyauchi A, Kuma K, Matsuzuka F,
Matsubayashi S, Kobayashi A, Tamai H and Katayama S: Intrathyroidal
epithelial thymoma: An entity distinct from squamous cell carcinoma
of the thyroid. World J Surg. 9:128–135. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Liu X, Hadeti B, Zhang W and Wang J:
Thyroid carcinoma showing thymus-like differentiation: A
clinicopathologic study of 8 cases. Zhonghua Bing Li Xue Za Zhi.
40:89–93. 2011.(In Chinese). PubMed/NCBI
|
|
7
|
Bai T, Zhang YF, Wu HY and Bian A:
Cytological diagnosis of carcinoma shwoing thymus-like
differentiation of the thyroid gland. Acta Acad Med Xuzhou.
12:802–805. 2010.(In Chinese).
|
|
8
|
Pan YL, Xie Y, Pu WL, Luo ZM, Yuan CY and
Cai PR: Carcinoma showing thymus-like element of the thyroid: A
clinicopathological observation. J Diagn Pathol. 5:373–376.
2007.(In Chinese).
|
|
9
|
Luo J, Ni XH, Zhang G, et al:
Clinicopathologic features of carcinoma showing thymus-like
differentiation in the neck. J Oncol. 11:906–909. 2008.(In
Chinese).
|
|
10
|
Wu HP, Zhang ZP and Pan YL: Thyroid
carcinoma showing thymus-like differentiation: A case report. J
Diagn Concepts Pract. 6:2882007.(In Chinese).
|
|
11
|
Da J, Shi H and Lu J: Thyroid
squamous-cell carcinoma showing thymus-like element (CASTLE): A
report of eight cases. Zhonghua Zhong Liu Za Zhi. 21:303–304.
1999.(In Chinese). PubMed/NCBI
|
|
12
|
Tsutsui H, Hoshi M, Kubota M, Suzuki A,
Nakamura N, Usuda J, Shibuya H, Miyajima K, Ohira T, Ito K and
Ikeda N: Management of thyroid carcinoma showing thymus-like
differentiation (CASTLE) invading the trachea. Surg Today.
43:1261–1268. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Reimann JD, Dorfman DM and Nosé V:
Carcinoma showing thymus-like differentiation of the thyroid
(CASTLE): A comparative study: Evidence of thymic differentiation
and solid cell nest origin. Am J Surg Pathol. 30:994–1001. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Yoneda K, Matsui O, Kobayashi T, Gabata T,
Minato H and Hirokawa M: CT and MRI findings of carcinoma showing
thymus-like differentiation. Radiat Med. 23:451–455.
2005.PubMed/NCBI
|
|
15
|
Yamamoto Y, Yamada K, Motoi N, Fujiwara Y,
Toda K, Sugitani I and Kohno A: Sonographic findings in three cases
of carcinoma showing thymus-like differentiation. J Clin
Ultrasound. 41:574–578. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sun T, Wang Z, Wang J, Wu Y, Li D and Ying
H: Outcome of radical resection and postoperative radiotherapy for
thyroid carcinoma showing thymus-like differentiation. World J
Surg. 35:1840–1846. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kusada N, Hara Y, Kobayashi S, Weihua T,
Nakamura Y, Kakudo K and Yuasa H: A case of aggressive carcinoma
showing thymus-like differentiation with distant metastases.
Thyroid. 15:1383–1388. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Chang S, Joo M and Kim H: Cytologic
findings of thyroid carcinoma showing thymus-like differentiation:
A case report. Korean J Pathol. 46:302–305. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kakudo K, Bai Y, Ozaki T, Homma K, Ito Y
and Miyauchi A: Intrathyroid epithelial thymoma (ITET) and
carcinoma showing thymus-like differentiation (CASTLE):
CD5-positive neoplasms mimicking squamous cell carcinoma of the
thyroid. Histol Histopathol. 28:543–556. 2013.PubMed/NCBI
|
|
20
|
Dorfman DM, Shahsafaei A and Miyauchi A:
Intrathyroidal epithelial thymoma (ITET)/carcinoma showing
thymus-like differentiation (CASTLE) exhibits CD5 immunoreactivity:
New evidence for thymic differentiation. Histopathology.
32:104–109. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ito Y, Miyauchi A, Nakamura Y, Miya A,
Kobayashi K and Kakudo K: Clinicopathologic significance of
intrathyroidal epithelial thymoma/carcinoma showing thymus-like
differentiation: A collaborative study with Member Institutes of
The Japanese Society of Thyroid Surgery. Am J Clin Pathol.
127:230–236. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Roka S, Kornek G, Schüller J, Ortmann E,
Feichtinger J and Armbruster C: Carcinoma showing thymic-like
elements - a rare malignancy of the thyroid gland. Br J Surg.
91:142–145. 2004. View
Article : Google Scholar : PubMed/NCBI
|