Introduction
Inflammatory cells are present in the tumor
microenvironment of most cancers and have been reported to affect
tumor progression (1–3). The long-term survival of patients with
colon cancer is dependent on the pathological stage as well as the
complex interactions between tumor- and patient-associated factors.
In particular, systemic and local host inflammatory responses are
important determinants of cancer outcome. In contrast to the
systemic response, local infiltration of inflammatory cells in the
tumor microenvironment is associated with improved survival in
patients with colon cancer. Tumor-infiltrating T cells may be an
indicator of host immune response to tumor and an attractive target
for immunotherapy (4–7). However, the specific role of individual
leukocytic infiltrates in individual tumors remains to be
elucidated. This diversity of immunologic response to malignancies
renders the targeting of the immune system as part of anticancer
therapies a challenge.
Treatment of advanced colon cancer has improved over
the past 15 years. The combination of chemotherapy and biological
drugs, such as anti-epidermal growth factor receptor (EGFR) or
anti-vascular endothelial growth factor antibodies, as well as the
sequencing of different active drugs as the disease progresses, can
significantly improve outcomes (8,9). In
particular, treatment with monoclonal antibodies (cetuximab or
panitumumab) against the extracellular domain of the receptor has
become a major therapeutic strategy in the treatment of metastatic
colorectal cancer. However, the responses to EGFR-targeted
antibodies are relatively low, with improvements in survival
usually lasting only several months, and efficacy limited to
certain patient subtypes (10).
Nevertheless, despite these advances, the optimal treatment for
patients with advanced colon cancer in clinical practice is not yet
defined.
Overexpression of bone morphogenetic protein 7
(BMP7) promotes gene amplification and mutation consequence in cell
proliferation, survival, invasion, metastasis, and tumor-induced
neoangiogenesis (11–14). Thus targeting BMP7 constitutes an
effective therapy in colon cancer. In the present study, the BMP7
expression in surgical specimens of colon cancer was examined to
assess the association between this molecule and local immune
response. The examination of individual cell types cannot predict
outcomes, but it does suggest a prominent role at the level of
nodal involvement and lymphatic invasion in these patients. Thus,
the results support that the combination of adaptive immunotherapy
and biological drugs impact the treatment strategy for colon cancer
in distinct clinical settings.
Materials and methods
Clinical samples
Paraffin-embedded specimens of patients with
colorectal cancer (stages I–III) were retrieved retrospectively
from 46 patients who underwent surgery at the Department of
Surgery, Siping Hospital of China Medical University (Siping
China), between January 2005 and December 2014. The present study
was approved by the Research Ethics Committee at Siping Hospital of
China Medical University.
The patients were divided into 3 groups as per their
nodal metastasis grade (N0, N1, or N2). The first group comprised
11 patients (N0), the second group 20 patients (N1), and the third
group 15 patients (N2). The exclusion criteria for the study were:
i) Clinical evidence of active infection; ii) the presence of a
chronic inflammatory condition; and iii) preoperative
chemoradiotherapy. The tumors were staged according to the fifth
edition of the tumor, node and metastasis classification (15). Additional pathological data were
obtained from reports issued at the time of resection. The
clinicopathological characteristics of patients are shown in
Table I.
 | Table I.Pathological characteristics of colon
cancer patients. |
Table I.
Pathological characteristics of colon
cancer patients.
| Characteristics | N0 | N1 | N2 |
|---|
| Median age (range),
years | 62.36 (51–72) | 61.19 (53–69) | 60.72 (50–71) |
| Gender, no. (%) |
|
|
|
|
Female | 5 (37.5) | 9
(46.9) | 6 (47.6) |
| Male | 6 (62.5) | 11 (53.1) | 9 (52.4) |
| T stage primary
tumor, no. (%) |
|
|
|
| T0 | 0 | 0 | 0 |
| T1 | 0 | 0 | 0 |
| T2 | 2 | 0 | 0 |
| T3 | 9 | 20 | 15 |
| T4 | 0 | 0 | 0 |
| N stage primary
tumor, no. (%) |
|
|
|
|
Node-negative | 11 (100.0) | 0 | 0 |
|
Node-positive | 0 | 20 (100.0) | 15 (100.0) |
| N1 | 0 | 20 (100.0) | 0 |
| N2 | 0 | 0 | 15 (100.0) |
| M stage primary
tumor, no. (%) |
|
|
|
| M0 | 11 (100.0) | 14 (50.0) | 11 (100.0) |
| M1 | 0 | 6
(50.0) | 4 |
| Largest median
diameter, cm (range) | 3.29 (2.11–7.36) | 5.56 (2.09–8.73) | 6.67 (2.13–9.84) |
Immunofluorescence of
paraffin-embedded tissue sections and evaluation of staining
Paraffin-embedded sections (4 µm) were obtained to
assess lymphocyte markers, including CD4 (rabbit, polyclonal, IgG,
catalog no: ABIN671376 at a dilution of 1:1000), CD8 (rabbit,
polyclonal, IgG, catalog no: ab85792 at a dilution of 1:1000), CD25
(mouse, monoclonal, catalog no: ABIN320392 at a dilution of
1:1000), CD45 (rabbit, polyclonal, IgG, catalog no: ab17553 at a
dilution of 1:1000) and CD56 (mouse, monoclonal, catalog no:
ABIN2658999 at a dilution of 1:1000). The primary antibodies were
purchased from BD Biosciences (Wuhan, China). To detect CD4 and
CD25, a general Treg cell antigen was used. CD45 was used as a
common leukocyte antigen. CD8 was used as a cytotoxic T lymphocyte
(CTL) marker. CD45 was used as a leukocyte common antigen and CD56
was used as an NK cell marker. BMP7 immunoreactivities were
detected in the nucleus, and the data were evaluated as a labeling
index (LI), as previously described (16). Fluorescent staining with anti-mouse
and anti-rabbit Ig secondary antibodies [anti-rabbit IgG
(H+L)-FITC: 211-095-109, Jackson ImmunoResearch, Düsseldorf,
Germany] conjugated with Alexa dyes 488 and 568 (Invitrogen Life)
conjugated with Alexa dyes 488 and 568 (Invitrogen Life
Technologies, Paisley, UK) was used for double staining (CD4 and
CD25; CD8 and CD56). Nuclear counterstaining in this case was
performed with DAPI (Roche, Mannheim, Germany). Counting was
performed under a microscope (Olympus, BX51TF, Tokyo, Japan) at a
magnification of ×400. Stained immune cells were assessed without
knowledge of the clinical parameters of each patient. The positive
cells were evaluated in the nuclei of >1,000 tumor cells for
each case, and LI was calculated as the percentage of each type of
positive cell per 1,000 tumor cells counted at random in each
section. The cells in each sample were examined blindly by three
independent expert observers.
Statistical analysis
Data are shown as mean ± standard deviation.
Cross-tabulations variables were analyzed using Fisher's exact
test. Statistical analyses were performed using SPSS software,
version 19.0 (IBM SPSS, Chicago, IL, USA). P<0.05 was considered
to indicate a statistically significant difference.
Results
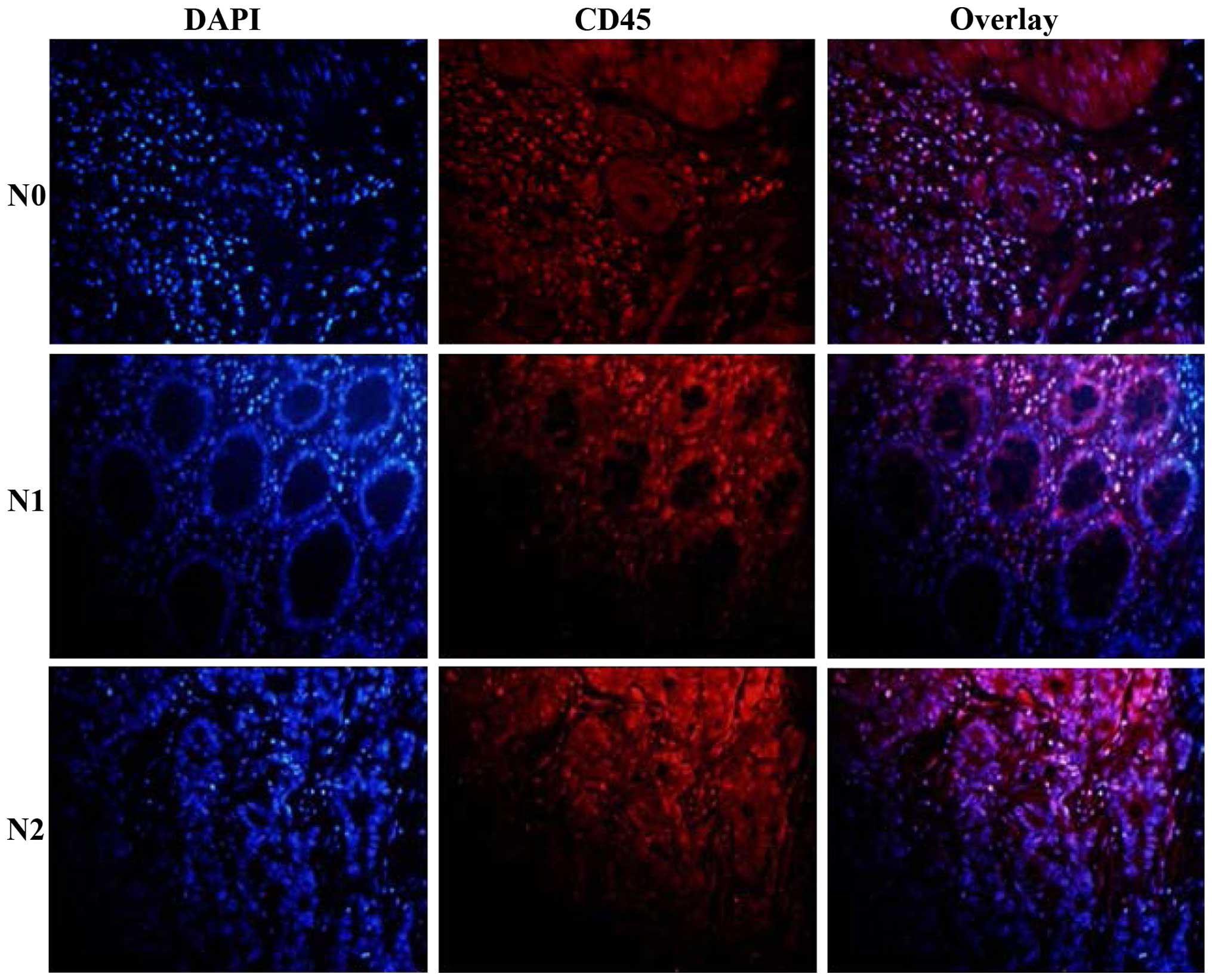
Evaluation of CD45+ cells
at the site of colon cancer tissue
Gross examination revealed massive infiltration of
CD45+ cells confined to nodal invasion (Fig. 1). Different patterns of immune cell
accumulations were observed among the patients which potentially
coexisted within the same specimen in colon cancer tissue as single
cells and diffused cell aggregates (Table II, Fig.
1). CD45+ cells were ranged at a percentage of
46.32, 31.61 and 16.74% in the N0, N1 and N2 nodal invasion groups,
respectively (Table II, Fig. 1).
| Table II.Associatoin between individual T
lymphocyte and the nodal invasion of colon cancer.a |
Table II.
Associatoin between individual T
lymphocyte and the nodal invasion of colon cancer.a
|
| Percentage of
individual T lymphocyte of colon cancer |
|---|
|
|
|
|---|
| Nodal invasion
group | CD45+ | CD4+ |
CD4+CD25+ |
CD8+ |
CD56+ |
|---|
| N0 |
46.32±6.08 |
14.63±3.47 |
8.11±3.26 |
6.23±3.13 |
4.41±1.13 |
| N1 |
31.61±4.65a,b |
21.19±6.12a |
15.42±5.09a |
2.14±2.08a |
1.98±0.69a |
| N2 |
16.74±3.37b,c |
28.63±11.35c |
21.37±11.33c |
0.21±0.36c |
0.19±1.01b |
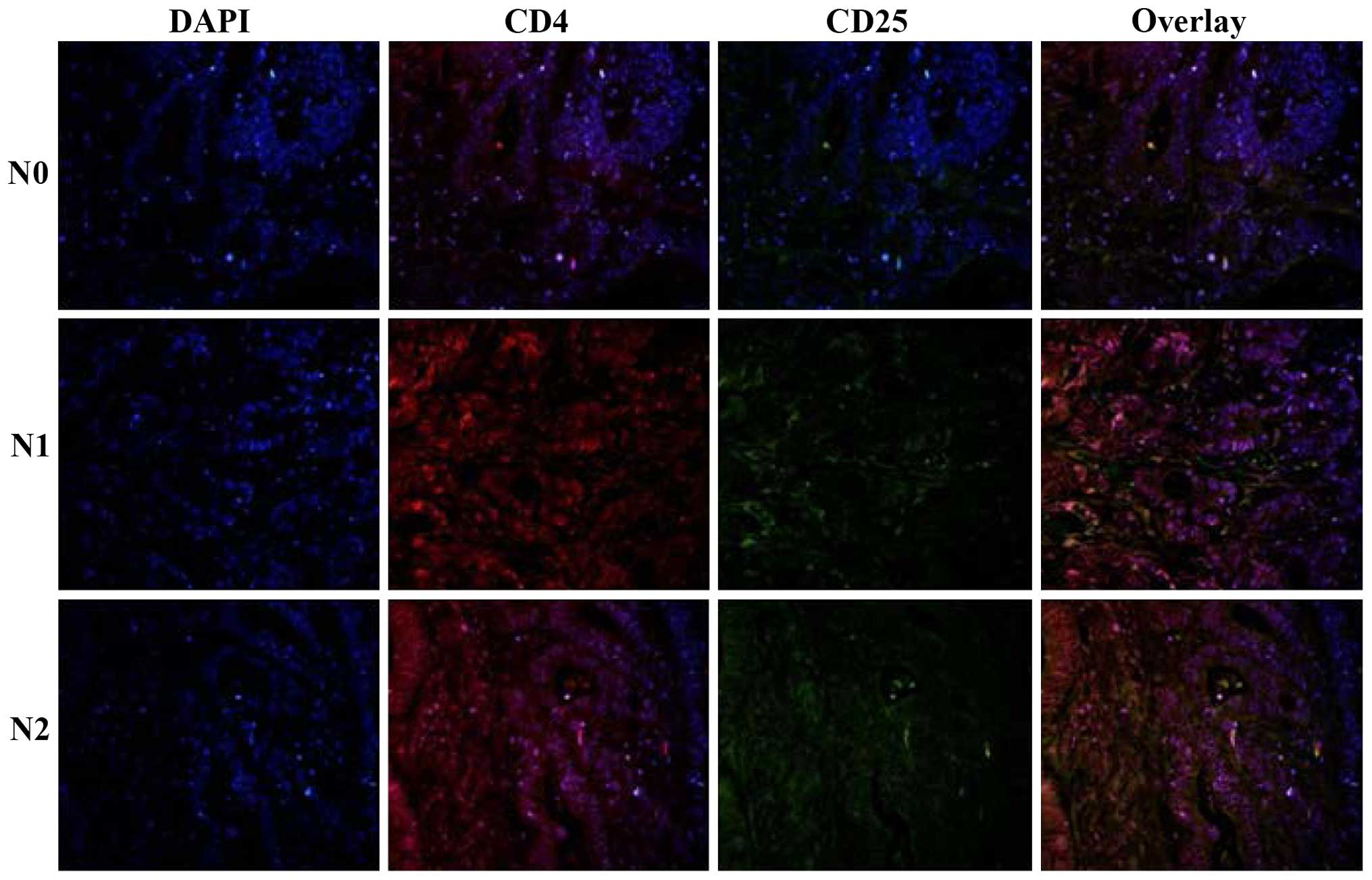
Patient-specific extent and
organization pattern of CD4+CD25+ T
lymphocytes in tumor tissue
To characterize the T-cell lineages in tumor tissue,
the tissue specimens were analyzed for
CD4+CD25+ cells. The major proportion of
cells within the large lymphocyte aggregates was
CD4+CD25+ T cells in the N2 nodal invasion
group. Quantitative evaluations of the three groups revealed the
presence of CD4+CD25+ T cells in tumor
tissue, ranging from 8.11, 15.42 to 21.37% in the N0, N1 and N2
nodal invasion groups (Table II,
Fig. 2).
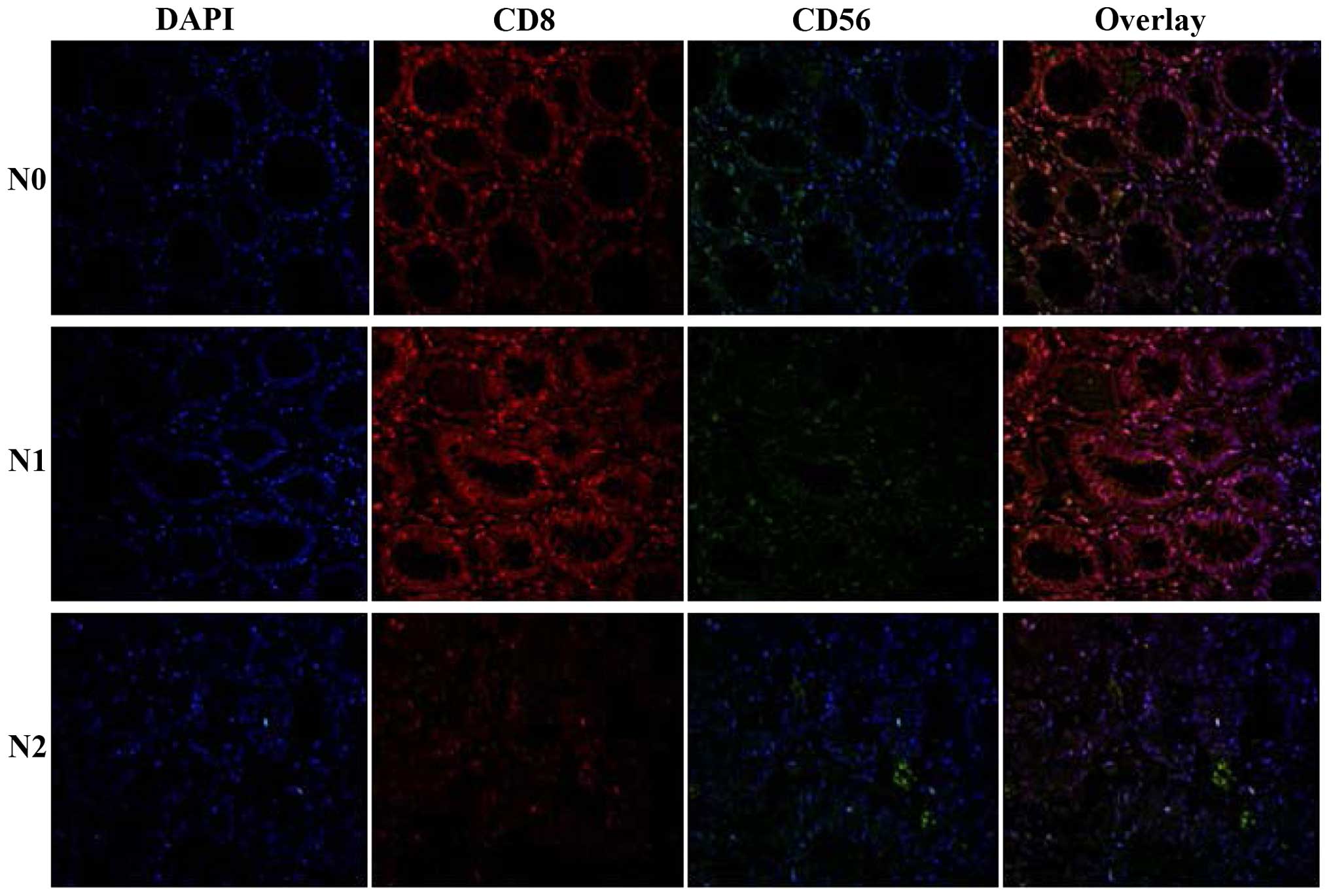
CD8+ T lymphocytes assemble
within the metastatic colon cancer
An important observation of the current study was
the presence of CD8+ T lymphocytes at the site of the
tumor tissue. CD8+ T lymphocytes were detected in all of
the patients in the N0 nodal invasion group. A comparison of the
three groups regarding CD8+ T lymphocytes in the tumor
tissue revealed statistically significant differences (Fig. 3, Table
II), whereas no CD8+ T lymphocytes were typically
present in the N2 nodal invasion group (Fig. 3, Table
II).
To characterize the role of NK cells in tumor
tissue, tissue sections were stained with anti-CD56 to define the
fully active, intra-tumoral NK cells. Only trace numbers of
CD56+ cells were observed in the N0 nodal invasion group
(Fig. 3, Table II).
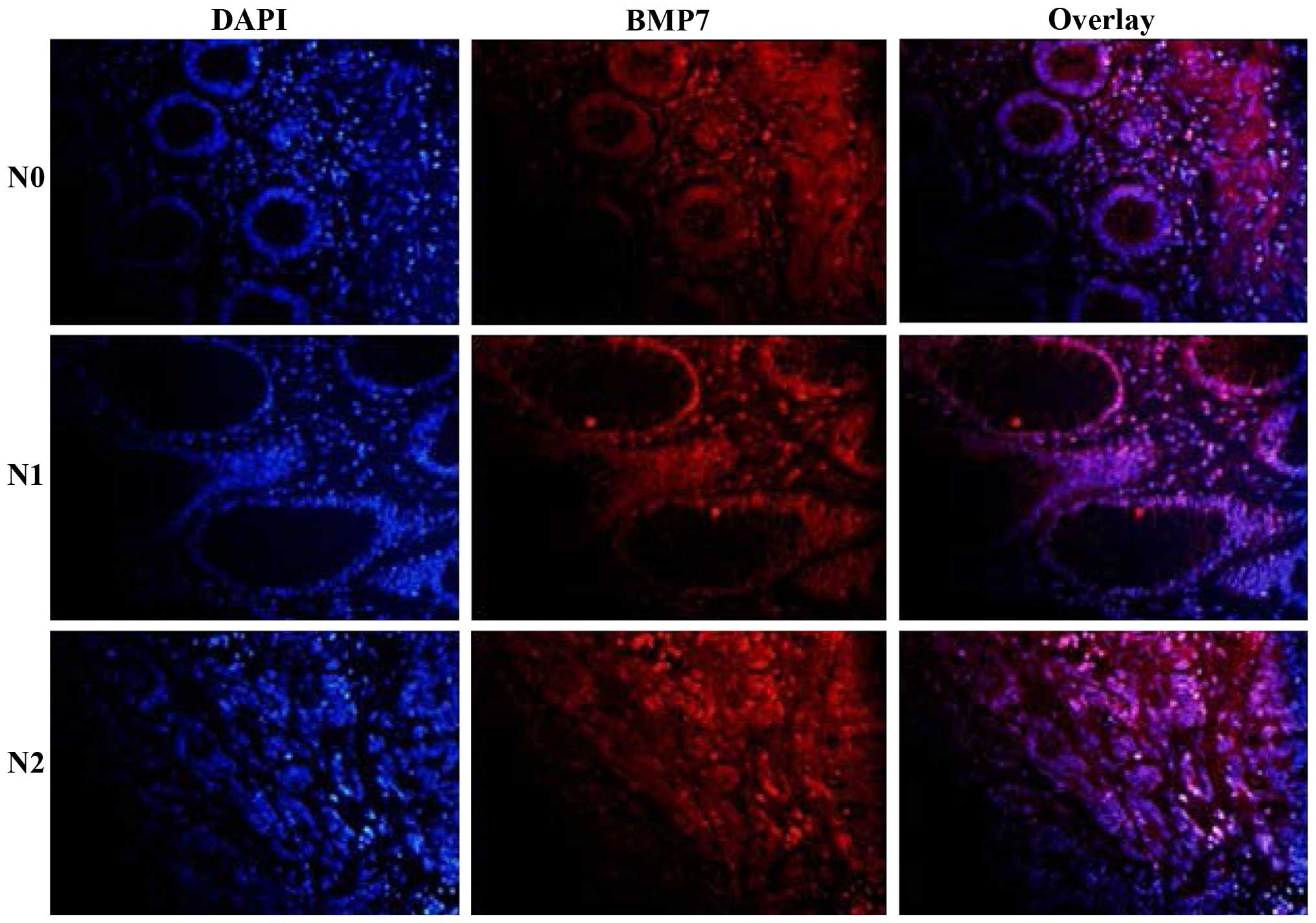
Expression of BMP7 in colon
cancer
The expression patterns and cellular localization of
BMP7 in 46 colon cancer tissues of three differentiation levels
were assessed by immunofluorescence analysis. As shown in Table III and Fig. 4, BMP7 immunoreactivity was
predominantly localized in the nuclei of CRC cells, whereas BMP7
was significantly higher in the poor nodal invasion group than in
the negative nodal group (P<0.01) (Table III, Fig.
4).
| Table III.Analyze the expression of BMP7
intra-tumor of colon cancer. |
Table III.
Analyze the expression of BMP7
intra-tumor of colon cancer.
| Expression | N0 | N1 | N2 |
|---|
| BMP7 | 13.06±1.21 |
28.32±5.64a |
40.73±8.35b,c |
Discussion
The clinical course of remission and relapse is
commonly observed in patients undergoing therapy for colon cancer
(17). In the present study, we
detected the overexpression of BMP7 in colon cancer tissues in its
advanced stage, in particular, its upregulation of BMP7 was closely
associated with nodal metastasis. Thus, the combination of
chemotherapy, radiation therapy, adaptive immunotherapy and
biological drugs, such as anti-BMP7 antibodies for first-line
treatment, can significantly improve outcomes.
The mechanisms by which a strong local adaptive
immune response improves prognosis in patients with colon cancer
remain to be elucidated. In the current study, we identified a
highly significant and independent association of CD45+
lymphocyte infiltration in the preoperative biopsy with nodal
invasion of colon cancer patients. The percentage of
CD45+ lymphocytes decreased in the later stage of colon
cancer tissue. Since the CD45 antigen was originally known as
leukocyte common antigen (18), the
findings strongly suggest that such patients mount a coordinated
inflammatory response at a local level, mediated primarily by cells
associated with adaptive immunity.
Immunotherapy was utilized for the treatment of
colon cancers. To examine T-cell subsets, we evaluated the
distribution of T lymphocytes with CD4, CD8 and CD25 phenotype and
analyzed the association between different subsets of T lymphocytes
and nodal metastasis in colon cancer tissue. For this study, CD4
and CD25 were selected as the regulatory markers for T cells, with
CD8 being used as the effector CTLs. Using double immunoflourescent
staining and confocal analysis, we confirmed that to a large extent
the markers separate in the three different situations of nodal
metastasis. We also evaluated CD56+ cells in colon
cancer tissue, which is similar to CD8+ T cells, but
decreased in the later stage of colon cancer. Of note, the
mechanism of adaptive immunity limitation was of considerable
interest and remains to be investigated.
Colon cancers resist certain therapies, such as
chemotherapy and adaptive immunotherapy. To investigate the reason
for this, the expression of BMP7 in colon cancer tissue was
examined. BMP7 has been reported in a wide range of human cancers
and has been associated with metastasis and poor prognosis
(14,19,20). In
the current study, the expression of BMP7 was 13.4, 28.1 and 40.6%
in the N0, N1 and N2 stage, respectively. These findings suggest
BMP7 overexpression tended to localize lymph node relapse. In
contrast to cells associated with the adaptive immune response, an
abundance of CD4+CD25+ T cells was associated
with the abundance of BMP7 expression. These results suggest a
protective host response, i.e., the collective effect of BMP7
expression and CD4+CD25+ T-cell infiltration
in the tumor may favor tumor growth and dissemination. Thus, our
results suggest monoclonal antibodies may be used under immune
contexture.
The study has some limitations. The identification
and classification of individual T-cell types should be
investigated. Additionally, more patients should be examined for
concrete evidence and restricting potential clinical application.
The present study focused only on the intra-tumor tissue and did
not assess the inflammatory cell invasive margin of the tumor,
which is reported to constitute a critical interface between pro-
and anti-tumor factors. Furthermore, examination of the prognostic
value of intra-tumor inflammatory cells and tumor molecular
features need to be verified.
In conclusion, our results have demonstrated the
co-expression of CD4+CD25+ T cells and BMP7
in a considerable percentage of patients with nodal metastatic
colon cancer. Overexpression of BMP7 is a potential predictor of
nodal invasion, while the molecular marker for high-risk patients
may be useful in individualizing patient therapy, such as anti-BMP7
antibodies for first-line treatment, can significantly improve
outcomes. In particular, the results suggest the combination of
adaptive immunotherapy and biological drugs impact the treatment
strategy for colon cancer in distinct clinical settings.
Acknowledgements
This study received a grant from the Department of
Science and Technology of Jilin Province (Jilin, China) (no.
201105100), and special funds for Innovation and Industrial
Development of the Independent Core Area (Beiijng, China)
(2014).
References
|
1
|
Mantovani A, Allavena P, Sica A and
Balkwill F: Cancer-related inflammation. Nature. 454:436–444. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Porta C, Larghi P, Rimoldi M, Totaro MG,
Allavena P, Mantovani A and Sica A: Cellular and molecular pathways
linking inflammation and cancer. Immunobiology. 214:761–777. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Solinas G, Marchesi F, Garlanda C,
Mantovani A and Allavena P: Inflammation-mediated promotion of
invasion and metastasis. Cancer Metastasis Rev. 29:243–248. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zou W: Regulatory T cells, tumour immunity
and immunotherapy. Nat Rev Immunol. 6:295–307. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Speetjens FM, Lauwen MM, Franken KL, van
Janssen Rhijn CM, van Duikeren S, Bres SA, van de Velde CJ, Melief
CJ, Kuppen PJ, van der Burg SH, et al: Prediction of the
immunogenic potential of frameshift-mutated antigens in
microsatellite instable cancer. Int J Cancer. 123:838–845. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Curiel TJ: Tregs and rethinking cancer
immunotherapy. J Clin Invest. 117:1167–1174. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Disis ML, Bernhard H and Jaffee EM: Use of
tumour-responsive T cells as cancer treatment. Lancet. 373:673–683.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Schmoll HJ, Van Cutsem E, Stein A,
Valentini V, Glimelius B, Haustermans K, Nordlinger B, van de Velde
CJ, Balmana J, Regula J, et al: ESMO Consensus Guidelines for
management of patients with colon and rectal cancer. a personalized
approach to clinical decision making. Ann Oncol. 23:2479–2516.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Adam R, De Gramont A, Figueras J, Guthrie
A, Kokudo N, Kunstlinger F, Loyer E, Poston G, Rougier P,
Rubbia-Brandt L, et al: Jean-Nicolas Vauthey of the EGOSLIM (Expert
Group on OncoSurgery management of LIver Metastases) group: The
oncosurgery approach to managing liver metastases from colorectal
cancer: a multidisciplinary international consensus. Oncologist.
17:1225–1239. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Siena S, Sartore-Bianchi A, Di
Nicolantonio F, Balfour J and Bardelli A: Biomarkers predicting
clinical outcome of epidermal growth factor receptor-targeted
therapy in metastatic colorectal cancer. J Natl Cancer Inst.
101:1308–1324. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Alarmo EL, Rauta J, Kauraniemi P, Karhu R,
Kuukasjärvi T and Kallioniemi A: Bone morphogenetic protein 7 is
widely overexpressed in primary breast cancer. Genes Chromosomes
Cancer. 45:411–419. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Miyazaki H, Watabe T, Kitamura T and
Miyazono K: BMP signals inhibit proliferation and in vivo tumor
growth of androgen-insensitive prostate carcinoma cells. Oncogene.
23:9326–9335. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Beck SE, Jung BH, Del Rosario E, Gomez J
and Carethers JM: BMP-induced growth suppression in colon cancer
cells is mediated by p21WAF1 stabilization and modulated by
RAS/ERK. Cell Signal. 19:1465–1472. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Aoki M, Ishigami S, Uenosono Y, Arigami T,
Uchikado Y, Kita Y, Kurahara H, Matsumoto M, Ueno S and Natsugoe S:
Expression of BMP-7 in human gastric cancer and its clinical
significance. Br J Cancer. 104:714–718. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Fleming ID, Cooper J, Henson DE, Hutter
VPR, Kennedy BJ, Murphy GP, O'Sullivan B, Sobin LH, Yarbro JW, et
al: AJCC cancer staging manual (5th). Philadelphia, PA:
Lippincott-Raven. 1997.
|
|
16
|
Rodriguez-Martinez A, Alarmo EL, Saarinen
L, Ketolainen J, Nousiainen K, Hautaniemi S and Kallioniemi A:
Analysis of BMP4 and BMP7 signaling in breast cancer cells unveils
time-dependent transcription patterns and highlights a common
synexpression group of genes. BMC Med Genomics. 4:802011.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Huh JW, Park YA, Jung EJ, Lee KY, Kwon JE
and Sohn SK: Complete remission of unresectable colon cancer after
preoperative chemotherapy selected by adenosine triphosphate-based
chemotherapy response assay. J Korean Med Sci. 23:916–919. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sorbye SW, Kilvaer T, Valkov A, Donnem T,
Smeland E, Al-Shibli K, Bremnes RM and Busund LT: Prognostic Impact
of Lymphocytes in Soft Tissue Sarcomas. PLoS One. 6:e146112011.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Motoyama K, Tanaka F, Kosaka Y, Mimori K,
Uetake H, Inoue H, Sugihara K and Mori M: Clinical significance of
BMP7 in human colorectal cancer. Ann Surg Oncol. 15:1530–1537.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Megumi K, Ishigami S, Uchikado Y, Kita Y,
Okumura H, Matsumoto M, Uenosono Y, Arigami T, Kijima Y, Kitazono
M, et al: Clinicopathological significance of BMP7 expression in
esophageal squamous cell carcinoma. Ann Surg Oncol. 19:2066–2071.
2012. View Article : Google Scholar : PubMed/NCBI
|