Introduction
Neuroendocrine tumors are neoplasms that originate
from the cells of the endocrine and nervous systems. As rare
tumors, they have an annual incidence of 2.5–5.0 cases per 100,000
individuals (1). The thymus is one of
the rarest sites of neuroendocrine tumors. Thymic neuroendocrine
carcinoma (NEC) was categorized as thymoma until 1972, when Rosai
and Higa (2) differentiated thymic
NEC from thymoma and other thymic carcinomas; thymic NEC is
differentiated from thymoma microscopically, due to the presence of
rosettes with central necrosis, and differentiation of
neuroendocrine cells. Thymic NEC is an unusual neoplasm that
accounts for only 2–4% of all anterior mediastinal neoplasms
(3). The majority of thymic NECs have
an aggressive biological behavior, including invasion, local
recurrence and distant hematogenous metastasis (4). Distant metastasis is observed in various
locations, including the bones, lungs, spleen, liver and adrenal
glands (5,6). However, pancreatic metastasis resulting
from thymic NEC is extremely infrequent, and in the literature, to
the best of our knowledge, there have only been a few cases of
pancreatic metastasis from thymic NEC (7–9). The
current study presents the case of a patient with rare pancreatic
metastasis resulting from thymic NEC.
Case report
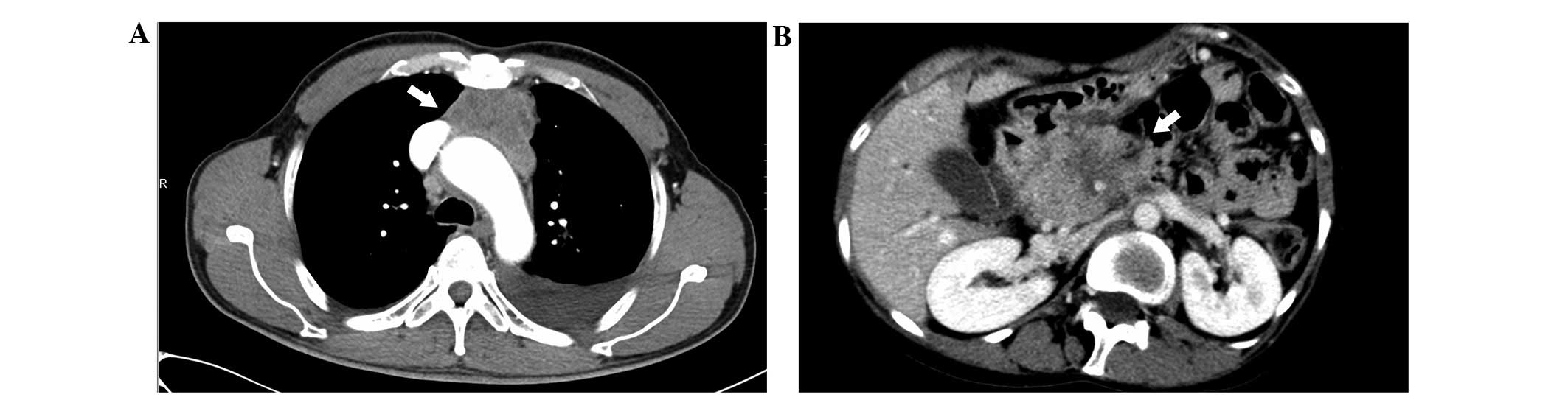
A 60-year-old man was admitted to the West China
Hospital (Chengdu, China) in January 2012 with a 7.1×6.3-cm
anterior mediastinal mass, which was observed on a routine chest
enhanced computed tomography (CT; SOMATOM Definition Flash; Siemens
Healthcare GmbH, Erlangen, Germany) scan (Fig. 1A). The medical history of the patient
revealed tuberculous pleurisy, which occurred 40 years previously.
A general physical examination was unremarkable. The patient
underwent surgery to resect the mass. During the surgery, the tumor
was observed to be located in the thymus with invasion to the
adjacent structures, including the pericardium, aortic arch and
left brachiocephalic vein. Consequently, the patient underwent
monobloc excision of the tumor with resection of the involved
structures.
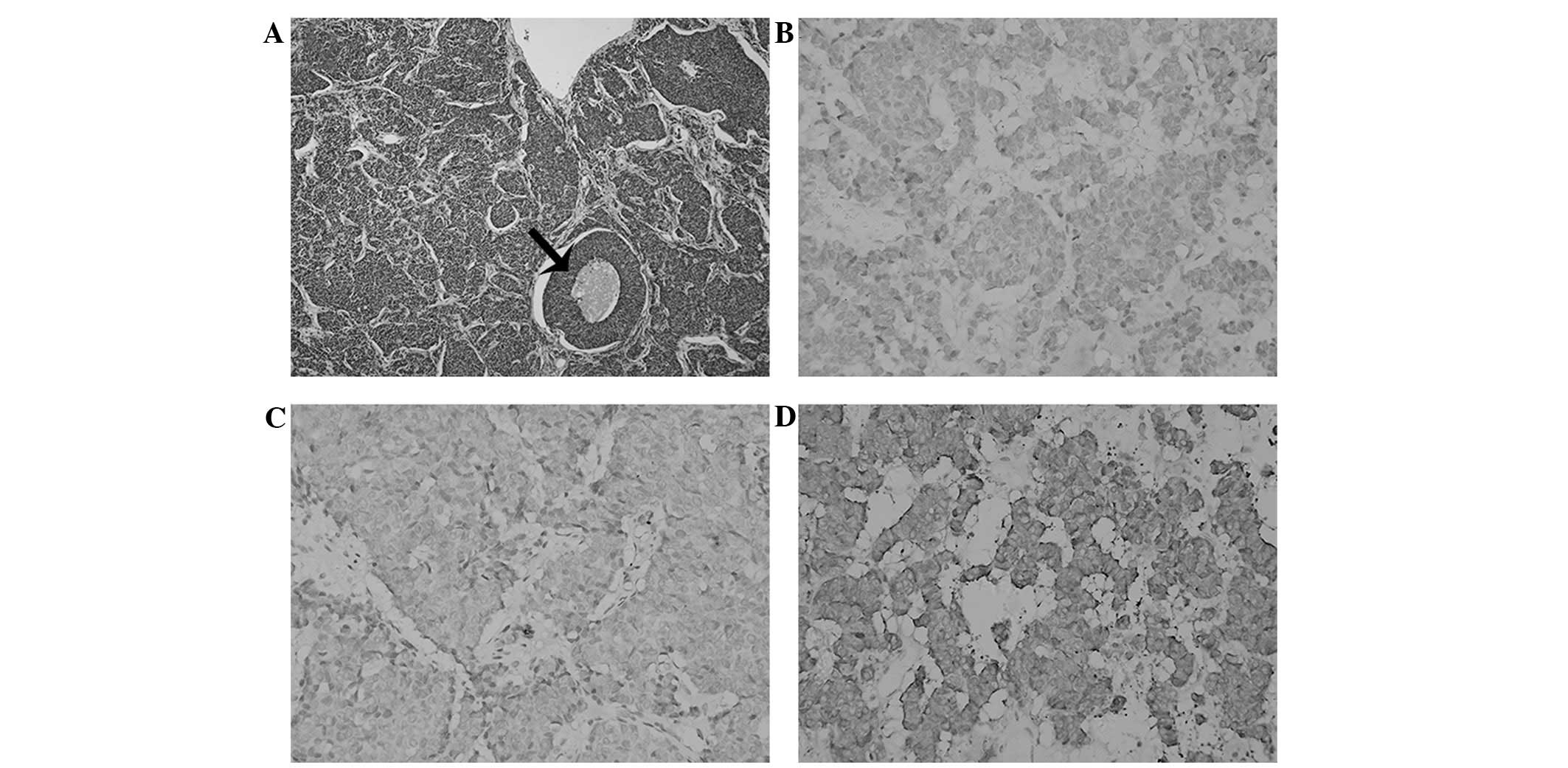
Macroscopically, the resected tumor was elastic and
soft and measured 9.0×7.0 cm in size. The cut surface of the tumor
was gray with regions of hemorrhage and necrosis. A diagnosis of
atypical thymic carcinoid was provided based on the morphological
characteristics and necrosis observed using hematoxylin and eosin
staining of formalin-fixed paraffin-embedded 5-µm thick tumor
tissue sections (Fig. 2A).
Immunohistochemistry was performed using 3,3′-diaminobenzidine
staining (ZSGB-BIO, Beijing, China) and the following primary
antibodies: Mouse monoclonal anti-human neural cell adhesion
molecule (dilution, 1:100; catalog no., ZM-0057; ZSGB-BIO); rabbit
monoclonal anti-human chromogranin A (dilution, 1:200; catalog no.,
ZA-0507; ZSGB-BIO); and rabbit polyclonal anti-human synaptophysin
(dilution, 1:200; catalog no., RAB-0155; Maixin Biotech, Fuzhou,
China). The tissue sections were then visualized under a microscope
(Eclipse E600; Nikon Corporation, Tokyo, Japan).
Immunohistochemistry demonstrated that the tumor cells expressed
neuroendocrine markers, including neural cell adhesion molecule
(Fig. 2B), chromogranin A (Fig. 2C) and synaptophysin (Fig. 2D), which confirmed the diagnosis of an
atypical thymic carcinoid. The Ki-67 index of the tumor cells was
~20%. The patient received post-operative treatment 4 weeks after
surgery, which consisted of chemotherapy and radiotherapy. In
total, the patient received 4 cycles of carboplatin (450 mg on day
1 of a 4-week cycle) and etoposide (100 mg/day on days 1–5).
Subsequently, the mediastinal structures of the patients were
irradiated with 27 fractions at a total dose of 54 Gy over 6 weeks.
Follow-up was scheduled every 6 months, and consisted of clinical
examination, CT scans and blood tests.
In November 2013, the patient was readmitted to
hospital due to the presence of a tumor in the pancreatic head,
which had been observed on a CT scan during follow-up (Fig. 1B). The patient underwent a total
pancreatectomy and splenectomy to resect the pancreatic head tumor.
Macroscopically, the resected tumor was elastic and soft, and
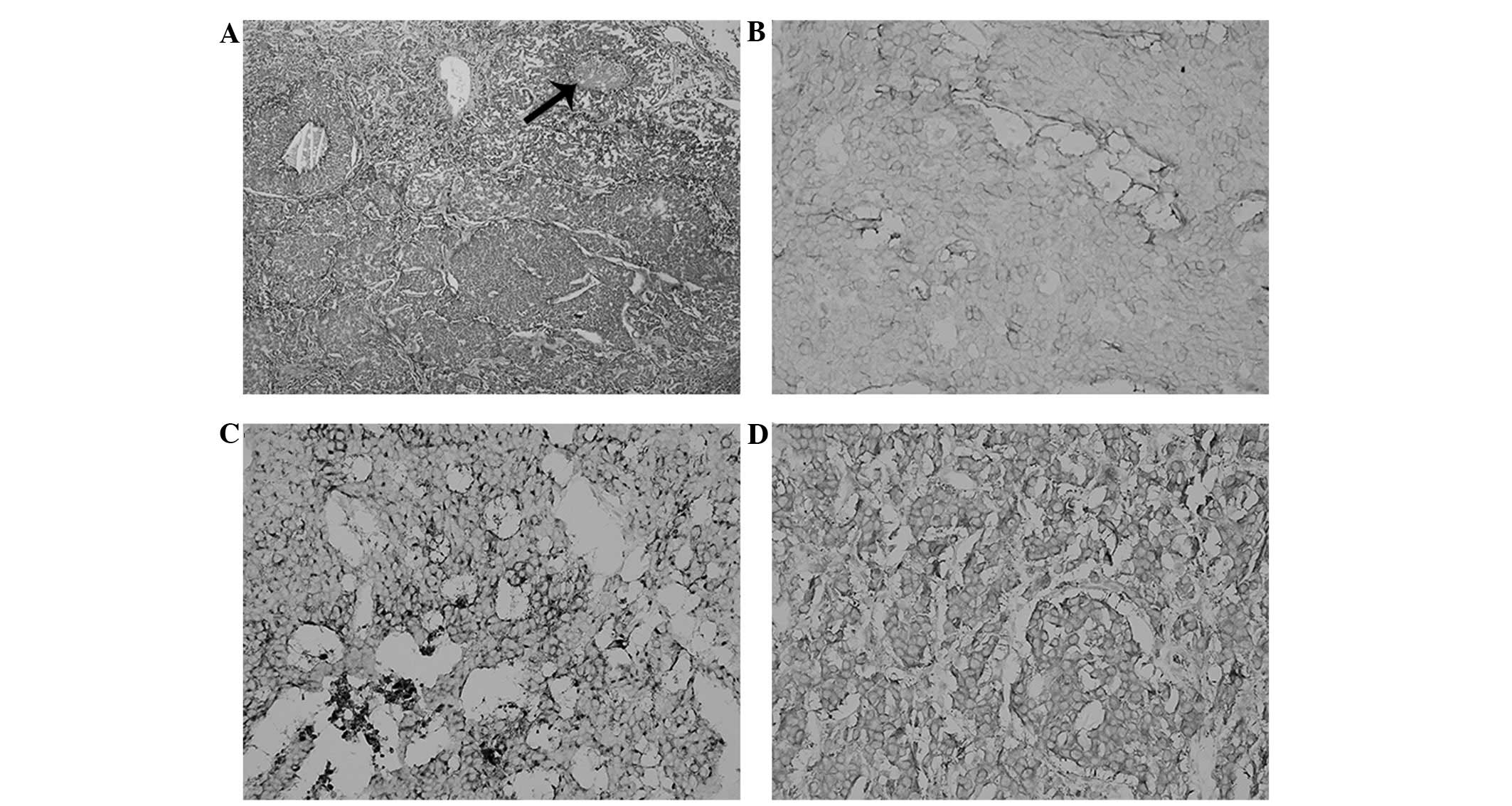
measured 7.0×6.0 cm in size. Histological examination revealed the
presence of 1 peripancreatic tumoral nodule, and 2 out of 4
peripancreatic lymph nodes were positive for metastasis.
Pathological examination revealed that the cytological morphology
of the metastasis was identical to that of the originally resected
thymic carcinoma (Fig. 3A).
Immunohistochemistry revealed that the pancreatic tumor cells
expressed neural cell adhesion molecule (Fig. 3B), chromogranin A (Fig. 3C) and synaptophysin (Fig. 3D); however, the tumor cells did not
express insulin, gastrin, glucagon and somatostatin. The Ki-67
index of the cells was 10–25%. A final diagnosis of pancreatic
metastasis resulting from thymic NEC was formed. The patient did
not receive post-operative therapies, and succumbed to the disease
9 months subsequent to surgery.
Written informed consent was obtained from the
family of the patient for the publication of the present study.
Discussion
Thymic NEC is an extremely rare tumor that only
accounts for 2–4% of all anterior mediastinal tumors and ~6% of
carcinoid tumors (3,10). The majority of patients diagnosed with
thymic NEC are in the 4th and 5th decades of life, and there is a
3:1 male to female ratio (5,11,12).
Symptomatic patients usually present with dyspnea, cough, chest
pain and superior vena cava syndrome due to the presence of the
mediastinal mass. In addition, clinical endocrinopathy develops in
~50% of all patients; Cushing's syndrome (25%) and multiple
endocrine neoplasia type 1 (15%) are the most common (12,13).
However, similar to the case presented in the current study, over
one-third of patients are asymptomatic, and the tumors are
incidentally observed on routine chest CT (4).
Thymic NEC is definitively diagnosed using
immunohistochemistry. Thymic NEC cells express neuroendocrine
markers, including synaptophysin, chromogranin A and neural cell
adhesion molecule. In addition, thymic NEC is morphologically
categorized into four main types: Typical carcinoid, atypical
carcinoid, large cell neuroendocrine carcinoma and small cell
carcinoma (14,15). Therefore, according to the
immunohistochemical and morphological diagnostic criteria, the
patient in the present study was diagnosed with thymic atypical
carcinoid.
Surgery is the most effective treatment for thymic
NEC and radical excision is the most critical factor for predicting
the long-term survival of patients (16). Radical excision often consists of
en-bloc resection of the tumor with resection of the involved
structures (17). The role of
radiotherapy in the treatment of thymic NEC is controversial;
however, it is recommended in order to prevent local recurrence of
invasive tumors (5,6,18).
Single-agent or combination drug chemotherapies, including
5-fluorouracil, streptozotocin, carmustine, cisplatin and
etoposide, have been used without any significant effect on the
recurrence rate and overall survival time of patients (11,19,20).
However, although there is a limited effect on the long-term
survival of patients, adjuvant chemotherapy may lead to mixed
short-term survival times of patients. Therefore, a
multidisciplinary therapy consisting of surgery, post-operative
chemotherapy and radiotherapy is recommended to achieve the best
outcome in patients with thymic NEC. In the current study, the
patient underwent a complete resection and received post-operative
chemotherapy and radiotherapy.
Despite multidisciplinary therapy, thymic NEC has a
poor prognosis. Metastasis is common in thymic NEC; even though the
patient in the current study had been treated with a radical
excision, plus post-operative chemotherapy and radiotherapy,
metastasis occurred in the pancreatic head. It is well known that
the majority of thymic NECs possess a more aggressive biological
behavior compared with other thymic epithelial tumors and
neuroendocrine carcinoma originating at other locations, including
the gastrointestinal tract and lungs (14). The aggressive biological behavior
exhibited by thymic NEC may comprise invasion to proximal
structures, including the pericardium, mediastinal fatty tissue,
major blood vessels and lungs, local recurrence and distant
hematogenous metastasis. Invasion to local structures is reported
in 50% of cases of thymic NEC and distant hematogenous metastasis
is reported in 20–30% of cases (21).
Distant metastasis is identified in various locations, often in the
bones, lungs, spleen, liver, brain and adrenal glands. However, in
the current study, the patient exhibited an extremely rare
pancreatic metastasis. To the best of our knowledge, there have
only been 3 cases of patients with pancreatic metastasis resulting
from thymic NEC previously reported in the literature (7–9). Axelson
et al (7) reported a case in
which several pancreatic tumors, which were located in the body and
tail of the pancreas, were diagnosed 8 years following treatment
for primary thymic NEC. In that study, the patient underwent a
thymectomy and pancreatectomy, and 40 Gy of radiotherapy following
the thymectomy. Lee et al (8)
reported a case of pancreatic metastasis resulting from thymic NEC
2 years following therapy for a primary tumor. The patient received
radiotherapy following a thymectomy and chemotherapy, which was
administered to the patient subsequent to a pancreatectomy.
Varytimiadis et al (9) also
reported a case of pancreatic metastasis of thymic NEC, which was
observed 5 years following treatment for a primary lesion. The
patient in that study received radiotherapy subsequent to each
surgery, and chemotherapy was administered to the patient following
a thymectomy. Additional details concerning the therapeutic
regimens, outcomes of patients and imaging results of the primary
thymic NEC were not provided in these 3 studies.
Thymic NEC is extremely rare, and metastatic spread
to the pancreas is particularly rare. Consequently, there is
limited clinical experience available to formulate effective
therapeutic regimens to treat thymic NEC. Therefore, more cases of
patients with thymic NEC require documentation to aid in the study
of this disease.
References
|
1
|
Oberg K and Castellano D: Current
knowledge on diagnosis and staging of neuroendocrine tumors. Cancer
Metastasis Rev. 30(Suppl 1): 3–7. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Rosai J and Higa E: Mediastinal endocrine
neoplasm, of probable thymic origin, related to carcinoid tumor.
Clinicopathologic study of 8 cases. Cancer. 29:1061–1074. 1972.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wick MR and Rosai J: Neuroendocrine
neoplasms of the mediastinum. Semin Diagn Pathol. 8:35–51.
1991.PubMed/NCBI
|
|
4
|
Chaer R, Massad MG, Evans A, Snow NJ and
Geha AS: Primary neuroendocrine tumors of the thymus. Ann Thorac
Surg. 74:1733–1740. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Fukai I, Masaoka A, Fujii Y, Yamakawa Y,
Yokoyama T, Murase T and Eimoto T: Thymic neuroendocrine tumor
(thymic carcinoid): A clinicopathologic study in 15 patients. Ann
Thorac Surg. 67:208–211. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
de Montpréville VT, Macchiarini P and
Dulmet E: Thymic neuroendocrine carcinoma (carcinoid): A
clinicopathologic study of fourteen cases. J Thorac Cardiovasc
Surg. 111:134–141. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Axelson J, Kobari M, Furukawa T and
Matsuno S: Thymic carcinoid in the pancreas: Metastatic disease or
new primary tumours. Eur J Surg. 165:270–273. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lee YT, Tse GM, Lai PB and Sung JJ:
Metastatic thymic neuroendocrine carcinoma presenting as a
pancreatic tumor. Endoscopy. 38(Suppl 2): E58–E59. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Varytimiadis K, Kalaitzakis E, Salla C,
Ghika E, Pandazopoulou A and Karoumpalis I: Pancreatic metastasis
of thymic neuroendocrine carcinoma: Is there a role for endoscopic
ultrasound? Report of a case and review of the literature.
Pancreas. 38:230–232. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Soga J, Yakuwa Y and Osaka M: Evaluation
of 342 cases of mediastinal/thymic carcinoids collected from
literature: A comparative study between typical carcinoids and
atypical varieties. Ann Thorac Cardiovasc Surg. 5:285–292.
1999.PubMed/NCBI
|
|
11
|
Filosso PL, Dato Actis GM, Ruffini E,
Bretti S, Ozzello F and Mancuso M: Multidisciplinary treatment of
advanced thymic neuroendocrine carcinoma (carcinoid): Report of a
successful case and review of the literature. J Thorac Cardiovasc
Surg. 127:1215–1219. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Detterbeck FC and Parsons AM: Thymic
tumors. Ann Thorac Surg. 77:1860–1869. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kondo K and Monden Y: Therapy for thymic
epithelial tumors: A clinical study of 1,320 patients from Japan.
Ann Thorac Surg. 76:878–884; discussion 884–885. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Moran CA and Suster S: Neuroendocrine
carcinomas (carcinoid tumor) of the thymus. A clinicopathologic
analysis of 80 cases. Am J Clin Pathol. 114:100–110. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chetty R, Batitang S and Govender D: Large
cell neuroendocrine carcinoma of the thymus. Histopathology.
31:274–276. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kim DJ, Yang WI, Choi SS, Kim KD and Chung
KY: Prognostic and clinical relevance of the World Health
Organization schema for the classification of thymic epithelial
tumors: A clinicopathologic study of 108 patients and literature
review. Chest. 127:755–761. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Spaggiari L and Pastorino U: Double
transmanubrial approach and sternotomy for resection of a giant
thymic carcinoid tumor. Ann Thorac Surg. 72:629–631. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
de Perrot M, Spiliopoulos A, Fischer S,
Totsch M and Keshavjee S: Neuroendocrine carcinoma (carcinoid) of
the thymus associated with Cushing's syndrome. Ann Thorac Surg.
73:675–681. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wang DY, Chang DB, Kuo SH, Yang PC, Lee
YC, Hsu HC and Luh KT: Carcinoid tumours of the thymus. Thorax.
49:357–360. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Gal AA, Kornstein MJ, Cohen C, Duarte IG,
Miller JI and Mansour KA: Neuroendocrine tumors of the thymus: A
clinicopathological and prognostic study. Ann Thorac Surg.
72:1179–1182. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Wick MR, Scott RE, Li CY and Carney JA:
Carcinoid tumor of the thymus: A clinicopathologic report of seven
cases with a review of the literature. Mayo Clin Proc. 55:246–254.
1980.PubMed/NCBI
|