Introduction
Pancreatic cancer is a malignancy with a
particularly poor prognosis (1).
Pancreatic ductal adenocarcinoma (PDAC) accounts for 85% of all
cases of pancreatic cancer, and is the most frequently observed
type of malignancy derived primarily from pancreatic cells
(2). It is equally common in men and
women, and mainly involves the head of the pancreas (2). In the majority of cases, the tumor
already infiltrates the adjacent structures at the time of
diagnosis, including the common bile duct, duodenum and ampulla
(1). Lesions are typically
irreversible, and the 5-year survival rate is 1–2% (1). The low percentage of survival in
pancreatic cancer cases results principally from the weak response
of cancer cells to treatment, which is mainly due to their high
level of resistance to apoptotic stimuli (1).
Apoptosis, also known as programmed cell death, is
involved in the physiological maintenance of normal cell
homeostasis, as well as having a role in pathological lesions that
accompany the course of various diseases (3,4). The
caspase activation mechanism is a major signaling pathway leading
to apoptosis (1). Caspases constitute
a group of cysteine proteases that occur in an inactive and an
activated form (4). They become
activated via the action of proteases, including their mutual
activation. Caspases may be divided into effectors (caspase-3, −6
and −7) and initiators (caspase-8 and −9) (4). Two mechanisms that lead to the
activation of the caspase initiators have been proposed: i) A
mechanism by which the inactive form of caspase-8 is activated upon
binding of its death receptor to a protein containing a death
domain, and whereby the activated protein directly stimulates
effector caspases such as caspase-3 (1,3,4); ii) and an alternative B-cell lymphoma 2
(Bcl-2) family-dependent mechanism that involves the cytosol and is
associated with the permeabilization of the mitochondrial outer
membrane and subsequent release of cytochrome c, apoptotic
protease activating factor 1 and additional apoptotic agents. This
leads to the formation of apoptosomes that activate caspase-9,
which subsequently triggers a cascade of effector caspases
(caspase-3 and −7) that induce the process of apoptosis (5). Disorders in these signaling pathways are
associated with cancer cell immortality (5).
Therefore, the aim of the present study was the
immunohistochemical assessment of the expression of caspase-8 and
the inactive and cleaved (active) forms of caspase-3 in the tissues
of patients exhibiting PDAC, and the subsequent analysis of the
association of caspase expression in these patients with specific
clinicopathological parameters.
Materials and methods
Patients and tumors
The present study group comprised 29 patients
exhibiting PDAC, who underwent surgery at the Department of General
Surgery and Gastroenterology at the Medical University of Białystok
(Białystok, Poland). The present study included 6 female and 23
male patients, whose ages ranged from 41 to 75 years. Sections
(4-µm) were cut from paraffin blocks and stained using hematoxylin
and eosin. Routine histopathological assessment of the sections
referred to the histological type, malignancy grade (G),
clinicopathological TNM status, regional lymph node involvement and
presence of distant metastases. Pancreatic adenocarcinomas were
moderately differentiated (G2) in 25/29 cases and poorly
differentiated (G3) in 4/29 cases. Adenocarcinomas were classified
as mucinous in 3/29 cases and non-mucinous in 26/29 cases. Lymph
node involvement was noted in 12/29 cases and metastasis to distant
organs (including liver and intestine) was observed in 9/29 cases.
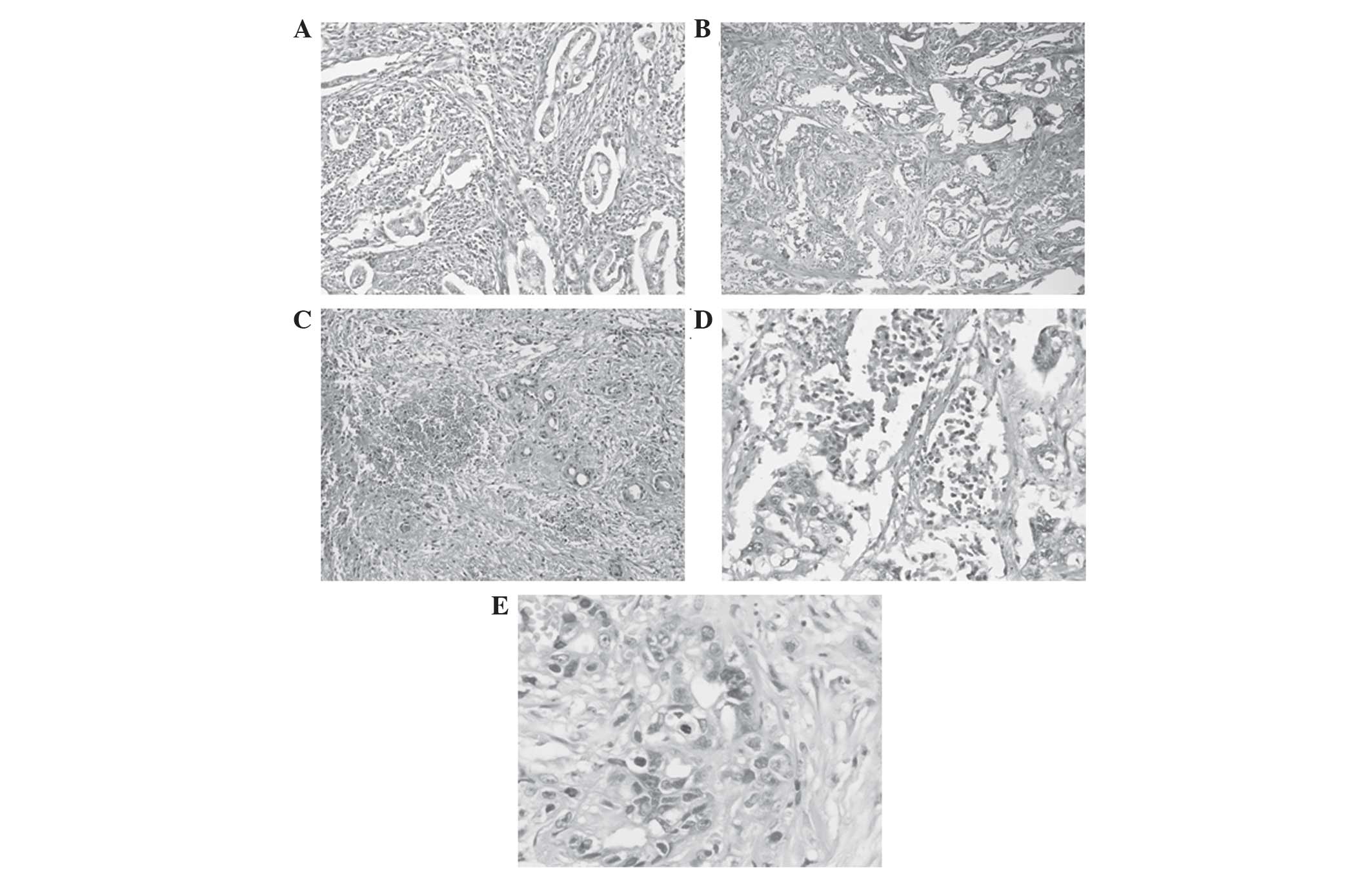
In addition, the degrees of inflammation, desmoplasia, necrosis and
foci of hemorrhage were assessed. A weak inflammatory response was
observed in 9 cases, a moderate response in 10 cases and a strong
response in 10 cases. Numerous foci of hemorrhage were observed in
5 cases, a single focus of hemorrhage was observed in 10 cases and
foci of hemorrhage were absent in 14 cases. Pancreatic
adenocarcinoma was associated with weak or moderate necrosis in 14
cases. Low- and high-grade desmoplastic tumors were noted in 12 and
17 cases, respectively. The histological features of pancreatic
adenocarcinoma are presented in Fig.
1.
The present study was performed in accordance with
the Declaration of Helsinki for human experimentation and received
approval from the local bioethics committee of the Medical
University of Białystok.
Mitotic index (MI) and apoptotic
bodies examination
MI was counted as the number of mitotic figures/10
high-power fields (magnification, ×40), and samples were
categorized into two groups with cut-off values of <5 and >5
MI. Apoptotic bodies were identified as fragmented nuclear debris
with cytoplasmic vacuoles, and counted as described above for MI.
Samples were classified into two groups with cut-off values of
<5 and >5 apoptotic bodies.
Immunohistochemical analysis
Formalin-fixed and paraffin-embedded tissue
specimens were cut on a microtome into 4-µm sections, which were
subsequently deparaffinized with xylene (Chempur, Piekary Śląskie,
Poland) and hydrated in graded alcohol (Chempur). In order to
visualize the antigens of pro-caspase-3 and caspase-8, the sections
were heated in a microwave oven (LAZNIE-WLS-084; Adverti, Lodz,
Poland) for 20 min in citrate buffer (pH 6.0; Sigma-Aldrich, St.
Louis, MO, USA). The antigen of cleaved caspase-3 was visualized by
heating the sections for 20 min in ethylenediaminetetraacetic acid
buffer (pH 9.0; Sigma-Aldrich). Sections were incubated with 3%
hydrogen peroxide solution (Chempur) for 20 min in order to block
endogenous peroxidase activity. Subsequently, incubation was
performed with rabbit monoclonal antibody against human
pro-caspase-3 (cat. no. ab32150; Abcam, Cambridge, UK; incubated
for 1 h, dilution, 1:500), rabbit polyclonal immunoglobulin G
against human/mouse cleaved caspase-3 (cat. no. AF835; R&D
Systems, Inc., Minneapolis, MN, USA; incubated for 30 min,
dilution, 1:400) and rabbit monoclonal antibody against human
caspase-8 (cat. no. sc-56070; Santa Cruz Biotechnology, Inc.,
Dallas, TX, USA; incubated for 1 h; dilution, 1:60). The reaction
was performed using Novostain Super ABC Kit (universal) (Leica
Microsystems, Inc.) at room temperature. A color reaction for
peroxidase was developed with DAB Chromogen Solution (Dako,
Glostrup, Denmark). Negative control sections were incubated
without primary antibody in citrate buffer. All sections were
counterstained with hematoxylin.
Immunohistochemical staining was evaluated by two
independent pathologists who were blinded to the clinical
information. The expression of the investigated proteins was
observed in the cytoplasm of normal ductal epithelial and tumor
cells in all the cases analyzed. Caspase-8, pro-caspase-3 and
cleaved caspase-3 expression was determined using a
semiquantitative method, and was defined in relation to the
intensity of staining (0, absent; 1, weak; 2, moderate; and 3,
strong) and the percentage of positive tumor cells. H-score was
derived by adding the percentages of stained cells at each
intensity and multiplying by the weighted intensity of staining,
according to the following formula: H-score = (% unstained cells ×
0) + (% weakly stained cells × 1) + (% moderately stained cells ×
2) + (% strongly stained cells × 3). Scores ranged from 0 to 300.
The study group was divided into negative (H-score <150) and
positive cases (H-score >150).
Statistical analysis
Statistical analysis was performed using STATISTICA
version 10.0 software (StatSoft, Inc., Tulsa, OK, USA).
Correlations between the clinicopathological parameters and the
expression levels of caspases exhibited by the patients were
calculated using the Spearman's rank correlation test. P<0.05
was considered to indicate a statistically significant difference.
Missing data were removed in pairs when one of the
clinicopathological parameters were unavailable.
Results
Expression of caspase-8, pro-caspase-3
and cleaved caspase-3 is observed in normal pancreas and cancerous
cells
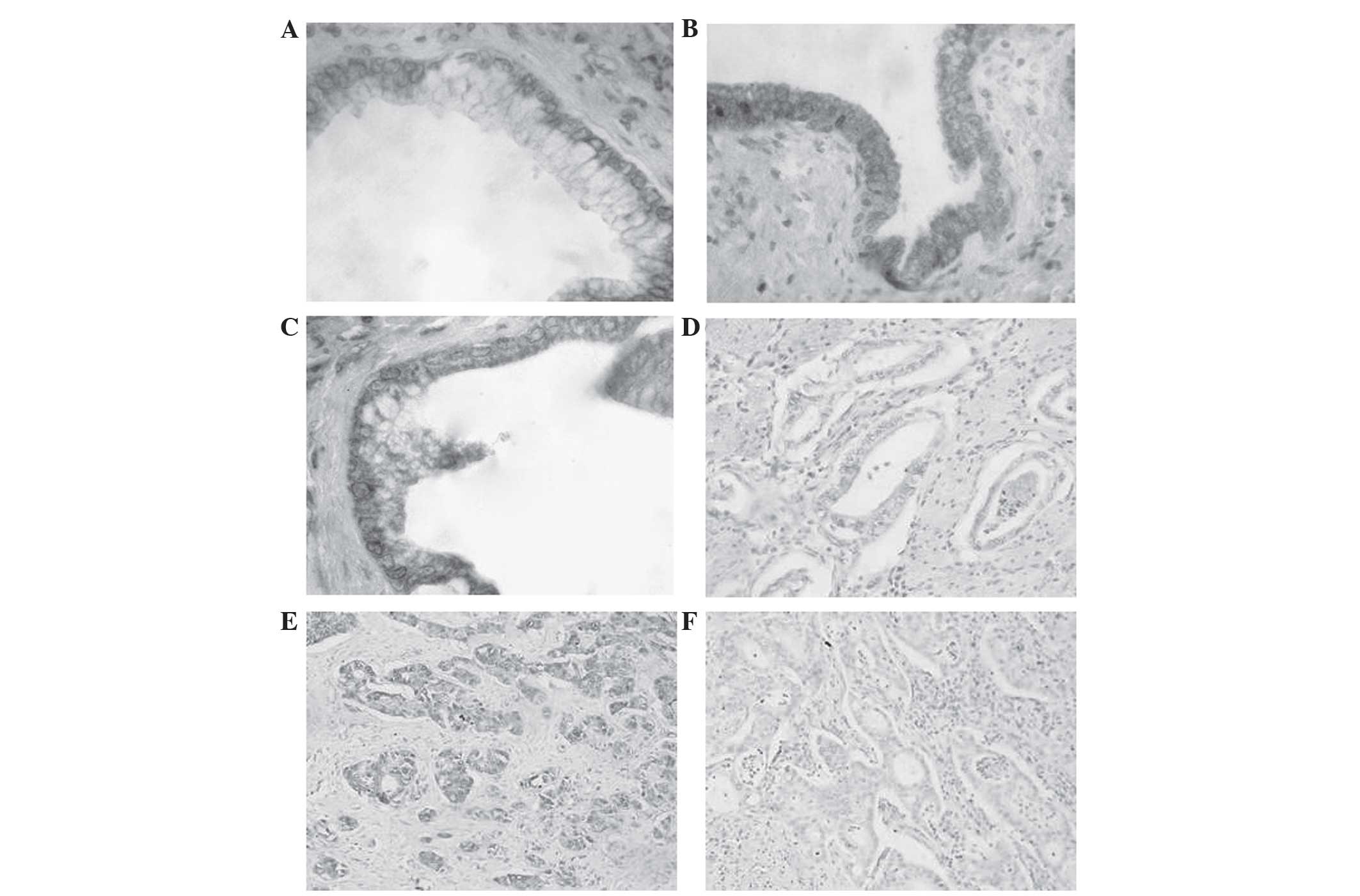
Color reaction corresponding to positive protein
expression of caspase-8, pro-caspase-3 and active caspase-3 was
detected in the cytoplasm of normal pancreatic cells (including
ductal epithelial, lobular and single pancreatic cells of the
islets of Langerhans) and in PDAC cells. Due to the origin of PDAC,
only the normal glandular epithelium of the ducts was precisely
analyzed and used in the statistical analysis. Furthermore, no
expression of the investigated proteins was identified in normal
pancreatic stroma.
The expression of caspase-8 in normal cells was
negative in 17.2% and positive in 82.8% of cases. However, PDAC
cells demonstrated positivity for caspase-8 expression in ~50% of
cases. All cases demonstrated pro-caspase-3 expression in normal
pancreatic cells, compared with 93.1% of cancer cells. Activated
caspase-3 was expressed in normal tissue in 27 cases, compared with
only 10 cases in PDAC cells. A substantial decrease was observed in
the expression of caspase-8 and active caspase-3 in cancer cells,
compared with the high expression levels of these proteins in
normal pancreatic cells. The expression of caspase-8, pro-caspase-3
and active caspase-3 in normal and cancerous cells is summarized in
Table I and Fig. 2.
 | Table I.Immunohistochemical characteristics of
caspase expression in normal and pancreatic tumor cells. |
Table I.
Immunohistochemical characteristics of
caspase expression in normal and pancreatic tumor cells.
|
| Normal ductal cells,
n (%) | Pancreatic ductal
cancer cells, n (%) |
|---|
|
|
|
|
|---|
| Protein
expression | Negative | Positive | Negative | Positive |
|---|
| Caspase-8 | 5 (17.2) | 24 (82.8) | 14 (48.3) | 15 (51.7) |
| Pro-caspase-3 | 0 (0.0) | 29 (100.0) | 2 (6.9) | 27 (93.1) |
| Active caspase-3 | 2 (6.9) | 27 (93.1) | 19 (65.5) | 10 (34.5) |
A correlation exists between the
protein expression levels of the investigated caspases and certain
clinicopathological parameters
Statistical analysis revealed a strong positive
correlation between the expression of caspase-8 and active
caspase-3 in cancer cells (P<0.002). A reduction in caspase-8
expression was accompanied by a decrease in the levels of active
caspase-3. Expression of caspase-3 was identified to correlate with
inflammatory peritumoral infiltration (P<0.015). No correlation
was observed between the expression levels of the investigated
proteins and any other clinicopathological parameters of the
patients, including gender, age, type of cancer, malignancy grade,
presence of metastasis to lymph nodes or distant organs, grade of
desmoplasia, foci of hemorrhage, necrosis, MI and apoptotic bodies
(Table II).
| Table II.Clinicopathological characteristics of
patients exhibiting pancreatic ductal adenocarcinoma. |
Table II.
Clinicopathological characteristics of
patients exhibiting pancreatic ductal adenocarcinoma.
|
|
| Caspase-8 | Pro-caspase-3 | Active caspase-3 |
|---|
|
|
|
|
|
|
|---|
| Parameter | Patients, n (%) | R | P-value | R | P-value | R | P-value |
|---|
| Age, years |
|
|
|
|
|
|
|
| ≤60 | 14 (48.3) |
|
|
|
|
|
|
|
>60 | 15 (51.7) | −0.017 | 0.890 | −0.165 | 0.678 | 0.188 | 0.342 |
| Gender |
|
|
|
|
|
|
|
| Male | 23 (79.3) |
|
|
|
|
|
|
|
Female | 6 (20.7) | 0.215 | 0.574 | −0.016 | 0.076 | 0.199 | 0.886 |
| Adenocarcinoma
type |
|
|
|
|
|
|
|
|
Non-mucinous | 26 (89.7) |
|
|
|
|
|
|
|
Mucinous | 3 (10.3) | 0.193 | 0.295 | 0.135 | 0.512 | −0.079 | 0.637 |
| Grade of
malignancy |
|
|
|
|
|
|
|
| G2 | 25 (86.2) |
|
|
|
|
|
|
| G3 | 4 (13.8) | −0.013 | 0.985 | 0.159 | 0.439 | −0.095 | 0.578 |
| Lymph node
metastasis |
|
|
|
|
|
|
|
|
Absent | 17 (58.6) |
|
|
|
|
|
|
|
Present | 12 (41.4) | 0.036 | 0.873 | 0.079 | 0.701 | 0.008 | 0.863 |
| Distant
metastasis |
|
|
|
|
|
|
|
|
Absent | 20 (69.0) |
|
|
|
|
|
|
|
Present | 9 (31.0) | −0.083 | 0.661 | 0.023 | 0.911 | −0.146 | 0.389 |
| Inflammation in
peritumoral stroma |
|
|
|
|
|
|
|
|
Absent | 2 (6.9) |
|
|
|
|
|
|
|
Weak | 9 (31.0) |
|
|
|
|
|
|
|
Moderate | 10 (34.5) |
|
|
|
|
|
|
|
Strong | 8 (27.6) | 0.320 | 0.082 | 0.143 | 0.195 | 0.404 | <0.015 |
| Grade of
desmoplasia |
|
|
|
|
|
|
|
|
Low | 12 (41.4) |
|
|
|
|
|
|
|
High | 17 (58.6) | −0.242 | 0.193 | −0.128 | 0.679 | −0.316 | 0.068 |
| Foci of
hemorrhage |
|
|
|
|
|
|
|
|
Absent | 14 (48.3) |
|
|
|
|
|
|
|
Single | 10 (34.5) |
|
|
|
|
|
|
| Numerous | 5 (17.2) | 0.134 | 0.487 | 0.032 | 0.868 | 0.008 | 0.964 |
| Necrosis |
|
|
|
|
|
|
|
|
Absent | 16 (55.2) |
|
|
|
|
|
|
|
Weak | 7 (24.1) |
|
|
|
|
|
|
|
Moderate | 6 (20.7) |
|
|
|
|
|
|
|
Strong | 0 (0.0) | −0.040 | 0.837 | −0.294 | 0.121 | 0.089 | 0.643 |
| Mitotic index |
|
|
|
|
|
|
|
|
<5 | 27 (93.1) |
|
|
|
|
|
|
|
>5 | 2 (6.9) | 0.248 | 0.735 | −0.087 | 0.970 | 0.130 | 0.873 |
| Apoptotic
bodies |
|
|
|
|
|
|
|
|
<5 | 25 (86.2) |
|
|
|
|
|
|
|
>5 | 4 (13.8) | 0.146 | 0.267 | −0.093 | 0.927 | −0.034 | 0.055 |
| Protein expression
in cancer cells |
|
|
|
|
|
|
|
|
Caspase-8 | 27 (93.1) | . – | – | 0.195 | 0.308 | 0.542 | <0.002 |
|
Pro-caspase-3 | 26 (86.7) | 0.195 | 0.308 | . – | – | −0.212 | 0.269 |
| Active
caspase-3 | 21 (72.4) | 0.542 | <0.002 | −0.212 | 0.269 | . – | – |
Discussion
Normal pancreatic cells, identical to other body
cells, undergo the physiological process of controlled cell death,
known as apoptosis (6). This
mechanism conditions normal cell function and enables maintenance
of homeostasis (7). The process of
apoptosis involves the Bcl-2 family-dependent signaling pathway and
the caspase-regulated signaling pathway (7). It has been previously demonstrated that
the action of these proteins is disrupted in pancreatic cells
affected by various pathologies (6–8).
In normal pancreatic tissue, positive expression of
caspase-8 has been identified in the cytoplasm of glandular cells,
single islets of Langerhans and ductal epithelial cells (8). The results of the present study are
consistent with the observations reported by Virkajärvi et
al (9), who described the
expression of caspase-8 in all types of structural cells in the
pancreas, as well as strong expression of caspase-8 in inflamed
areas surrounding the islets of Langerhans. Analysis of caspase-8
expression in cancer cells confirmed its presence in 74% of
patients exhibiting pancreatic adenocarcinoma, and strong
expression was observed in a small percentage of cases (9). In the present study, ~93% of cases
exhibiting PDAC demonstrated positive expression of caspase-8.
Similar results have been reported in other gastrointestinal
tumors, including gastric or colorectal cancer. Sträter et
al (10) reported moderate or
strong caspase-8 expression in the cancer cells of a small number
of colon tumors. Shintani et al (11) observed immunopositive cells for
caspase-8 in ~50% of gastric and colorectal adenocarcinoma cases.
Previous studies have indicated that this may be due to
disturbances in apoptosis induction within the Fas/Fas ligand
system, or alternative death ligands, including tumor necrosis
factor (TNF) or TNF-related apoptosis-inducing ligand, which may
cause dysfunction in initiator caspases such as caspase-8 and
inhibition of apoptosis during its initial stage (12,13).
The present study additionally focused on the
expression of caspase-3 in its precursor and activated forms in
normal pancreatic and cancer cells. A positive pro-caspase-3 color
reaction was identified by immunohistochemistry in the cytoplasm of
normal and cancerous cells in the majority of cases analyzed. Thus,
it was speculated that PDAC cells may retain the potential to
produce the precursor form of caspase-3. To the best of our
knowledge, the present study is the first to assess the expression
of the two forms of caspase-3 separately. Virkajärvi et al
(9) evaluated the expression of the
precursor and active forms of caspase-3 using one antibody.
Expression of caspase-3 was observed in 80% of patients exhibiting
pancreatic adenocarcinoma. However, no correlation was identified
between apoptotic index and caspase-3 expression, which may
indicate the expression of the inactive form of caspase-3 in the
cancer cells of these patients (9).
Satoh et al (14) observed
high expression levels of caspase-3 in PDAC cells in the majority
of cases evaluated, and suggested that the precursor form of
caspase-3 may have contributed to the color observed upon
immunohistochemical staining (14).
In that study, caspase-3 expression was assessed in the cytoplasm
and nuclei of PDAC cells, and a correlation was observed between
cytoplasmic expression of caspase-3 and malignant tumor stage. In
addition, an association was observed between nuclear reaction and
benign tumor phenotype (14).
The present study particularly focused on the
expression of activated caspase-3. More frequent expression of
cleaved caspase-3 was observed in normal pancreatic cells, compared
with pancreatic duct cell tumors. In the present study, a
statistically significant correlation was identified between
caspase-8 and active caspase-3 expression in the tumor mass. A
decrease in the expression levels of caspase-8 or −3 caused a
reduction in the expression levels of the other, which confirmed
the involvement of these two proteins in the common apoptotic
signaling pathway of PDAC cells. Meggiato et al (15) noted an increased percentage of
positive expression of cleaved caspase-3 in the cytoplasm of tumor
cells, compared with the cytoplasm of epithelial cells that lined
the pancreatic ducts. It was suggested that the strong expression
of active caspase-3 in pancreatic tumor cells, as opposed to normal
ductal cells, indicated stimulation of the apoptosis-inducing
mechanisms (15). Similarly, Luo
et al (16) reported an
increase in the expression of cleaved caspase-3 in PDAC tissue
(43.9%), compared with normal tissue (3.5%). Furthermore,
statistically significant correlations were noted between caspase-3
expression and high tumor grade, tumor location in the head of the
pancreas, cyclin D1 gene amplification and presence of polysomy of
chromosome 11 (16). A detailed
analysis of these patients additionally revealed an association
between positive expression of active caspase-3 and shorter
survival time in patients exhibiting PDAC, and the expression of
active caspase-3 was identified as an independent risk factor
(16). In contrast to PDAC, high
expression levels of cleaved caspase-3 have been associated with
positive prognosis in patients diagnosed with colorectal cancer
(17). The previously mentioned
reports are not consistent with the results of the present study,
which may be due to the small size of the current patient cohort.
However, reduced expression of effector cleaved caspase-3 may be
associated with a lack of adequate agents to trigger the activation
of the protein, including caspase-8, or may result from disorders
in the Bcl-2 family-dependent signaling pathway of apoptosis, which
conditions the levels of cytochrome c present in the cytosol
(18). In contrast with normal cells,
pancreatic cancer cells demonstrate a reduced ability to activate
caspases via cytochrome c (18). It has been suggested that cancer cells
may require increased levels of cytochrome c in order to
activate the apoptotic signaling pathway of caspases (1). The reduced capacity of caspase-3
stimulation in PDAC cells may induce their resistance to apoptosis,
as well as determining their longevity and invasiveness (18). In consequence, PDAC belongs to a group
of tumors characterized by short survival times and poor prognoses
(18).
Despite the small size of the patient cohort in the
current study, the findings of the present study suggest that
pancreatic cancer may involve disturbances to the initiation of
cancer cell apoptosis via a decrease in the expression of
caspase-8, which may cause dysregulation in the activation of
effector caspase-3. Therefore, assessment of the expression of
caspase-8 and cleaved caspase-3 in the tissues of patients
exhibiting PDAC may aid the determination of the degree of
apoptotic activity in pancreatic cancer cells. This may be utilized
in the future to develop targeted therapies for the treatment of
PDA using activators of the proteins investigated in the present
study.
References
|
1
|
Gukovskaya AS and Pandol SJ: Cell death
pathways in pancreatitis and pancreatic cancer. Pancreatology.
4:567–586. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Reid MD, Bagci P and Adsay NV:
Histopathologic assessment of pancreatic cancer: Does one size fit
all? J Surg Oncol. 107:67–77. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Adams JM: Ways of dying: Multiple pathways
to apoptosis. Genes Dev. 17:2481–2495. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Schultz DR and Harrington WJ Jr:
Apoptosis: Programmed cell death at a molecular level. Semin
Arthritis Rheum. 32:345–369. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Li P, Nijhawan D, Budihardjo I,
Srinivasula SM, Ahmad M, Alnemri ES and Wang X: Cytochrome c
and dATP-dependent formation of Apaf-1/caspase-9 complex initiates
an apoptotic protease cascade. Cell. 91:479–489. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Steer ML: Early events in acute
pancreatitis. Baillieres Best Pract Res Clin Gastroenterol.
13:213–225. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tomita T: Cleaved caspase-3
immunocytochemical staining for pancreatic islets and pancreatic
endocrine tumors: A potential marker for biological malignancy.
Islets. 2:82–88. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Butler AE, Janson J, Bonner-Weir S, Ritzel
R, Rizza RA and Butler PC: Beta-cell deficit and increased
beta-cell apoptosis in humans with type 2 diabetes. Diabetes.
52:102–110. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Virkajärvi N, Pääkkö P and Soini Y:
Apoptotic index and apoptosis influencing proteins bcl-2, mcl-1,
bax and caspases 3, 6 and 8 in pancreatic carcinoma.
Histopathology. 33:432–439. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sträter J, Herter I, Merkel G, Hinz U,
Weitz J and Möller P: Expression and prognostic significance of
APAF-1, caspase-8 and caspase-9 in stage II/III colon carcinoma:
Caspase-8 and caspase-9 is associated with poor prognosis. Int J
Cancer. 127:873–880. 2010.PubMed/NCBI
|
|
11
|
Shintani M, Sangawa A, Yamao N, Miyake T
and Kamoshida S: Immunohistochemical analysis of cell death
pathways in gastrointestinal adenocarcinoma. Biomed Res.
32:379–386. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kornmann M, Ishiwata T, Kleeff J, Beger HG
and Korc M: Fas and Fas-ligand expression in human pancreatic
cancer. Ann Surg. 231:368–379. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tsuji S, Hosotani R, Yonehara S, Masui T,
Tulachan SS, Nakajima S, Kobayashi H, Koizumi M, Toyoda E, Ito D,
et al: Endogenous decoy receptor 3 blocks the growth inhibition
signals mediated by Fas ligand in human pancreatic adenocarcinoma.
Int J Cancer. 106:17–25. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Satoh K, Kaneko K, Hirota M, Toyota T and
Shimosegawa T: The pattern of CPP32/caspase-3 expression reflects
the biological behavior of the human pancreatic duct cell tumors.
Pancreas. 21:352–357. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Meggiato T, Calabrese F, De Cesare CM,
Baliello E, Valente M and Del Favero G: C-JUN and CPP32 (CASPASE 3)
in human pancreatic cancer: Relation to cell proliferation and
death. Pancreas. 26:65–70. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Luo Y, Qiu Z, Tian L, Zhu G, Feng Y, Yi M,
Chen X, Wang L, Li C and Huang Q: Identification of novel
predictive markers for the prognosis of pancreatic ductal
adenocarcinoma. Hum Pathol. 44:69–76. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Noble P, Vyas M, Al-Attar A, Durrant S,
Scholefield J and Durrant L: High levels of cleaved caspase-3 in
colorectal tumour stroma predict good survival. Br J Cancer.
108:2097–2105. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Vaquero EC, Edderkaoui M, Nam KJ, Gukovsky
I, Pandol SJ and Gukovskaya AS: Extracellular matrix proteins
protect pancreatic cancer cells from death via mitochondrial and
nonmitochondrial pathways. Gastroenterology. 125:1188–1202. 2003.
View Article : Google Scholar : PubMed/NCBI
|