Introduction
Schwannomas are common intracranial tumors,
accounting for ~8% of all primary brain neoplasms (1). These tumors are benign and slow growing
neoplasms of Schwann cell origin (1),
which mostly affect middle aged (52.4±15.7 years) individuals
(2). The overall 5-year survival rate
is 79.6%, while the post-operative mortality is 0.5% (2). The majority of tumors originate from the
vestibular portion of the auditory nerve at the cerebellopontine
angle (3), while tumors arising from
the trigeminal nerve are less common. Intrasellar schwannomas not
associated with cranial nerves are extremely rare, and, to the best
of our knowledge, only 17 cases have been reported in the English
literature to date (3–17). Intrasellar schwannomas typically
affect middle-aged and elderly individuals ranging from 33–79 years
of age, with no significant gender preferences (3–17).
Surgical resection is currently the leading treatment, and the
majority of patients have a good prognosis. Furthermore, the
majority of previous reports regarding intrasellar schwannomas have
focused on the surgical approaches and immunohistochemical features
of the tumor (4–7,9–12), whereas few studies have reported the
computed tomography (CT) and magnetic resonance imaging (MRI)
features of intrasellar schwannomas in detail. In the present
study, a case of pathologically confirmed intrasellar schwannoma is
presented, and the available literature is reviewed to summarize
the radiological features of this lesion.
Case report
In April 2014, a 50 year-old man presented to The
First Affiliated Hospital of Chongqing Medical University
(Chongqing, China) with decreased visual acuity that had lasted for
5 years, and had been aggravated for 1 week. Visual field
examination did not identify visual field loss. The patient had a
10-year history of hypertension and a 2-year history of diabetes
mellitus, and thus had been taking valsartan and metformin
regularly; this medication was continued throughout the
perioperative period. No abnormal findings were identified on
complete physical and neurological examinations, which included
assessments of the vital signs, muscle strength, muscle tone,
sensory system and reflex system, in addition to cranial nerve
examination. Preoperative endocrinological tests revealed normal
levels of triiodothyronine (T3; patient level, 2.17 pg/ml; normal
range, 2.19–3.90 pg/ml), thyroxine (T4; patient level, 0.91 ng/dl;
normal range, 0.61–1.12 ng/dl), thyroid-stimulating hormone (TSH;
patient level, 1.63 µIU/ml; normal range, 0.35–3.50 µIU/ml),
adrenocorticotropic hormone (ACTH; patient level, 20.97 pg/ml;
normal range, 7.20–63.30 pg/ml), prolactin (PRL; patient level,
6.55 ng/ml; normal range, 2.64–13.13 ng/ml), follicle-stimulating
hormone (FSH; patient level, 21.72 mIU/ml; normal range, 1.27–19.26
mIU/ml), luteinizing hormone (LH; patient level, 2.65 mIU/ml;
normalrange, 1.24–8.62 mIU/ml), growth hormone (GH; patient level,
0.03 ng/ml; normal range, 0.00–5.00 ng/ml), cortisol (patient
level, 169.93 nmol/l; normal range, 118.64–618.02 nmol/l) and
testosterone (patient level, 1.80 ng/ml; normal range, 1.75–7.81
ng/ml).
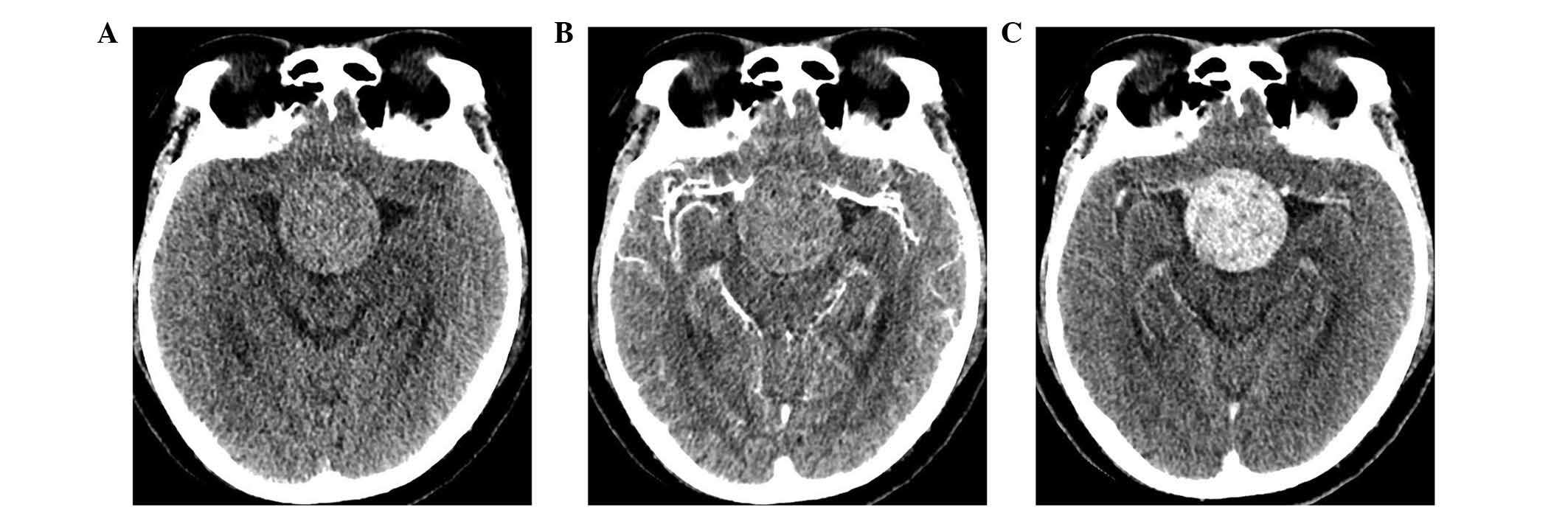
A CT scan (Somatom Definition FLASH CT scanner;
Siemens AG, Munich, Germany) revealed a 3.9×3.8 cm well-demarcated
intrasellar mass with suprasellar extension, without cavernous
sinus invasion (Fig. 1). The lesion
was slightly hyperdense compared to the brain parenchyma, with
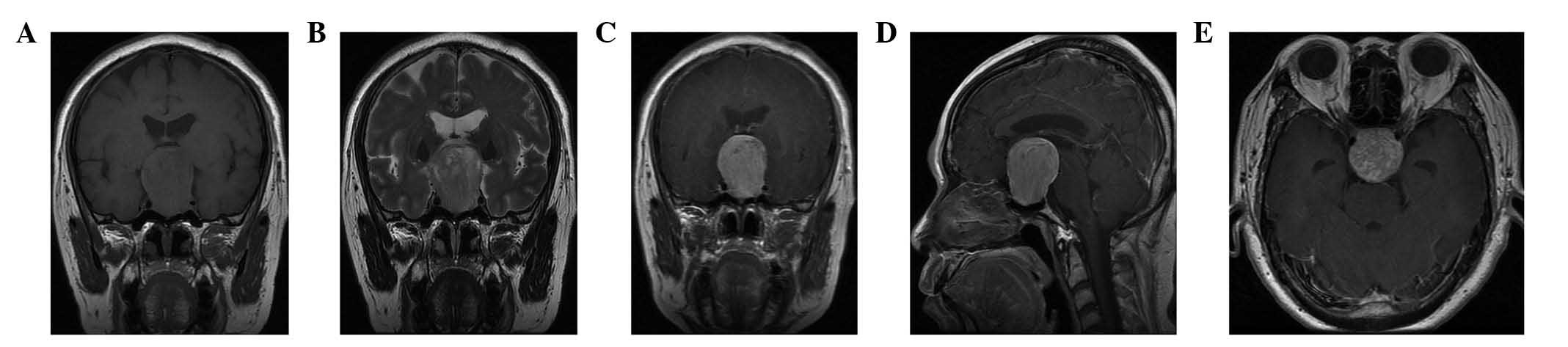
heterogeneous enhancement. On MRI (Signa HDxt 3.0T scanner; GE
Healthcare Bio-Sciences, Pittsburgh, PA, USA), the lesion was
isointense on T1 weighted images (WI), and slightly hyperintense on
T2WI images, with significant heterogeneous enhancement following
the intravenous administration of gadolinium diethylenetriamine
pentaacetic acid (Bayer AG, Leverkusen, Germany) (Fig. 2).
Non-functioning pituitary adenoma was diagnosed
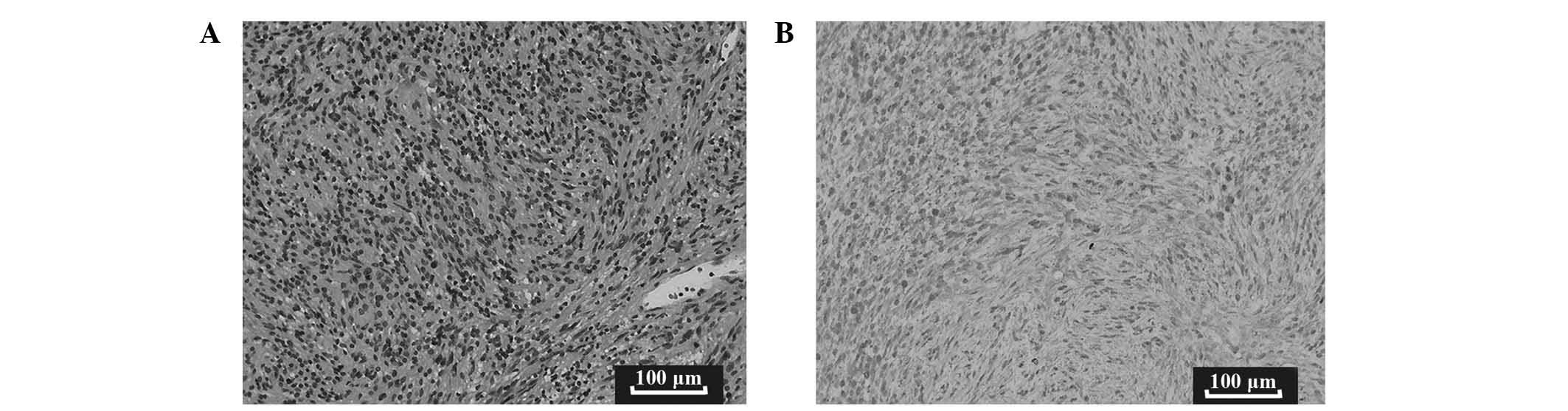
preoperatively. Subsequently, the patient underwent gross total
resection via an endonasal transsphenoidal approach. The resected
mass was soft, grayish and hypervascular. Microscopic examination
(using a XSG-111L microscope; Shunyu, Zhejiang, China) revealed a
tumor composed of cells arranged in a spindle (Fig. 3). Immunocytochemistry was performed on
the tumor cells by the Pathology Department at The First Affiliated
Hospital of Chongqing Medical University (Chongqing, China), which
revealed positivity for S100, and negativity for glial fibrillary
acidic protein and epithelial membrane antigen. Consequently,
schwannoma was diagnosed. Postoperative endocrinological tests
revealed panhypopituitarism. The results of the tests were as
follows: T3, 1.79 pg/ml (normal range, 2.19–3.90 pg/ml), T4, 0.90
ng/dl (normal range, 0.61–1.12 ng/dl), TSH, 0.12 µIU/ml (normal
range, 0.35–3.50 µIU/ml), ACTH, 6.86 pg/ml (normal range,
7.20–63.30 pg/ml), PRL, 3.27 ng/ml (normal range, 2.64–13.13
ng/ml), FSH, 8.43 mIU/ml (normal range, 1.27–19.26 mIU/ml), LH,
2.53 mIU/ml (normal range, 1.24–8.62 mIU/ml), GH, 0.12 ng/ml
(normal range, 0.00–5.00 ng/ml), cortisol, 265.13 nmol/l (normal
range, 118.64–618.02 nmol/l) and testosterone, 0.36 ng/ml (normal
range, 1.75–7.81 ng/ml).
The patient underwent replacement therapy with
hydrocortisone (30 mg once per day) and Euthyrox (25 µg once per
day, which were administered orally. MRI performed on follow-up
examination 3 months following surgery revealed no evidence of
tumor recurrence. Further MRI was planned at 6 month and 1 year
follow-ups. Written informed consent was obtained from the
patient.
To identify relevant studies, database searches of
all literature published prior to November 26, 2014 on PubMed
(Medline; www.ncbi.nlm.nih.gov/pubmed/) and Web of Science
(www.webofknowledge.com/) were performed,
using the search terms ‘pituitary fossa’, ‘intrasellar’, ‘sellar’
and ‘schwannoma’. All searches were limited to English language
publications. Suprasellar and parasellar schwannomas that did not
affect the intrasellar regions were excluded. A manual search of
the references of the retrieved articles was conducted
subsequently. The search yielded 15 articles corresponding to 17
cases, in addition to the present case, which are all presented in
Table I.
 | Table I.Intrasellar schwannomas: Literature
review. |
Table I.
Intrasellar schwannomas: Literature
review.
|
|
|
|
|
|
| CT findings | MRI findings |
|
|---|
|
|
|
|
|
|
|
|
|
|
|---|
| First author,
year | Case, no. | Gender | Age, years | Clinical
symptoms | Endocrine status | Density | Enhancement | T1 | T2 | Enhancement | (Ref.) |
|---|
| Perone, 1984 | 1 | M | 39 | Headache for 6
years | Normal | Iso | Homo | NA | NA | NA | (17) |
| Wilberger, 1989 | 2 | F | 62 | Visual loss for
several years |
Panhypopituitarism | NA | Homo | NA | NA | NA | (16) |
| Civit, 1997 | 3 | M | 41 | Bitemporal
hemianopsia | Normal | NA | NA | NA | NA | Homo | (15) |
| Bhagat, 2002 | 4 | M | 51 | Erectile impotence,
fatigue and lethargy for 5 years |
Panhypopituitarism | NA | NA | NA | NA | Homo | (14) |
| Bhagat, 2002 | 5 | M | 68 | Visual loss for 2
years |
Panhypopituitarism | NA | Homo | NA | NA | NA | (14) |
| Whee, 2002 | 6 | M | 39 | Decreased visual
acuity for 10 months |
Panhypopituitarism | NA | NA | Iso | ↑ | Homo | (13) |
| Maartens, 2003 | 7 | F | 33 | Headache for 6
months, decreased visual acuity, amenorrhea | Elevated prolactin,
hypothyroidism | NA | NA | NA | NA | Hetero | (12) |
| Maartens, 2003 | 8 | F | 56 | Bitemporal
hemianopia, ataxia | Hypopituitarism | NA | NA | NA | NA | NA | (12) |
| Esposito, 2004 | 9 | M | 73 | Lipothymia,
bitemporal hemianopia |
Panhypopituitarism | NA | NA | Iso | NA | Homo | (11) |
| Perez, 2004 | 10 | F | 71 | Bitemporal
quadrantanopia for 2 months | Normal | NA | Homo | Iso | NA | Homo | (10) |
| Honegger, 2005 | 11 | F | 79 | Syncope, headache
for 6 months | Hypothyroidism | NA | NA | NA | NA | Homo | (9) |
| Moreland, 2006 | 12 | M | 41 | Headache for 3
years | Normal | NA | NA | NA | NA | Homo | (8) |
| Krayenbühl,
2007 | 13 | M | NA | Headache, left
superior temporal quadrantanopia |
Panhypopituitarism | NA | NA | NA | NA | Hetero | (7) |
| Koutourousiou,
2009a | 14 | NA | 38 | Acromegaly | Elevated GH | NA | NA | NA | NA | NA | (6) |
| Park, 2009 | 15 | F | 49 | Headache, vomiting
and bitemporal hemianopsia | Normal | NA | NA | Iso | Slightly↑ | Homo | (5) |
| Mohammed, 2010 | 16 | F | 45 | Headache for 2
years, facial pain | Elevated prolactin,
decreased FSH and LH | NA | NA | NA | NA | Homo | (4) |
| Cugati, 2012 | 17 | M | 42 | Headache and visual
loss for 1 year | Normal | Iso | NA | Iso | Slightly↑ | Hetero | (3) |
| Present study | 18 | M | 50 | Decreased visual
acuity for 5 years | Normal | Slightly↑ | Hetero | Iso | Slightly↑ | Hetero | – |
Discussion
Pituitary adenomas account for the majority of
intrasellar tumors (8). The most
common non-pituitary-derived tumors of the sella tunica include
craniopharyngioma, glioma, meningioma and chordoma (4). As intrasellar schwannomas are extremely
rare (4), they are not usually
considered in the differential diagnosis of sellar tumors.
To date, only 18 cases of intrasellar schwannomas,
including the present case, comprising of 10 males and 7 females
(the gender of one case is not reported), with an average age of
51.6 years (range, 33–79 years) have been reported in the
literature (3–17). In 12 of the 18 cases (66.7%), patients
reported visual changes (particularly bitemporal hemianopsia), and
8 of the 18 cases (44.4%) suffered from headache. Less common
clinical presentations included personality changes, erectile
impotence, amenorrhea, syncope, vomiting and facial pain.
Only 3 cases (3,17)
described plain CT scan features of intrasellar schwannomas, 2 of
which appeared as an isodense mass, while the mass in the present
case was slightly hyperdense. A total of 4 reported cases (10,14,15,17)
exhibited enhanced CT features, all of which were reported to be
homogeneously enhanced. However, the mass in the present case
exhibited slight heterogeneous enhancement. Notably, marked cystic
changes, intratumoral hemorrhage, calcification and necrosis were
not identified in any of the 18 cases. All the 13 cases (3–5,7–15) that
reported MRI features presented an isointense signal on T1WI and
slightly hyperintense signal on T2WI, and the majority of these
cases (9/13; 69.2%) showed homogeneous enhancement. In addition,
the majority of cases exhibited a well-demarcated mass without
cavernous sinus invasion. By contrast, a large number of pituitary
adenomas invade the cavernous sinus (18). However, intrasellar schwannomas cannot
be distinguished from pituitary adenomas based on such features
alone (13).
In the present case, no specific nerve of origin was
identified, similarly to the majority of reported cases, and thus,
the origin of the intrasellar schwannoma remains unclear. However,
three histopathogenetic hypotheses exist regarding the origin of
intrasellar schwannoma. Firstly, Bleys et al (19) reported the existence of the lateral
sellar nerve plexus within the cavernous sinus, which is a
distribution center for visceromotor and sensory nerves innervating
cerebral arteries, orbital structures and the dura mater. Notably,
Dietemann et al (20) have
revealed that there is not a clear separation between the pituitary
fossa and the cavernous sinus, so there is a potential deficiency
in the medial wall of the cavernous sinus. Certain authors
(4,12)
propose that tumors originating from the lateral sellar nerve
plexus may extend through the the medial wall of the cavernous
sinus to form an intrasellar schwannoma. However, the majority of
reported cases do not involve the cavernous sinus (4–9). Secondly,
it has been suggested that perivascular Schwann cells may be the
source of intrasellar schwannomas (13). Small cerebral arteries of 10–15 µm in
diameter are known to be accompanied by a perivascular nerve
plexus, where Schwann cells may be located (21). Notably, intracerebral schwannomas
originating from the perivascular nerve plexus have been reported
(22,23). Therefore, it may be hypothesized that
intrasellar schwannomas may originate from the perivascular nerve
plexus of the inferior hypophyseal artery. Thirdly, Russell and
Rubinstein (1) have suggested that
intracerebral schwannomas may arise from ectopic Schwann cells;
therefore, this theory may also explain the origin of intrasellar
schwannomas.
In conclusion, intrasellar schwannomas are rare
sellar tumors, which are commonly misdiagnosed as pituitary
adenomas (13). Intrasellar
schwannomas usually affect middle-aged and elderly individuals
ranging from 33–79 years of age, with no significant gender
preferences (3). The most common
clinical presentations are visual changes and headache (3). On CT images, the majority of cases
appear as a well-demarcated isodense intrasellar mass with
homogeneous enhancement, without marked cystic change, intratumoral
hemorrhage, calcification or necrosis (3,10,14,16,17). The
majority of cases appear isointense on T1WI and slightly
hyperintense on T2WI, with homogeneous or heterogeneous enhancement
(3–5,7–15). The involvement of the cavernous sinus
in intrasellar schwannomas is less frequent than that observed in
pituitary adenomas (4,5,8,18). However, intrasellar schwannomas are
usually indistinguishable from pituitary adenomas. Therefore, the
final diagnosis is dependent on histology. Therefore, schwannomas
should be included in the differential diagnosis of an intrasellar
lesion.
Acknowledgements
The present study was supported by the National Key
Clinical Specialties Construction Program of China (Beijing, China;
grant no. 2013-544).
References
|
1
|
Russell DS and Rubinstein LJ: Pathology of
Tumours of the Nervous System (5th). London: Edward Arnold.
533–589. 1989.
|
|
2
|
Woehrer A, Hackl M, Waldhör T, Weis S,
Pichler J, Olschowski A, Buchroithner J, Maier H, Stockhammer G,
Thomé C, et al: Relative survival of patients with non-malignant
central nervous system tumours: A descriptive study by the Austrian
Brain Tumour Registry. Br J Cancer. 110:286–296. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Cugati G, Singh M, Symss NP, Pande A,
Yasha TC, Vasudevan MC and Ramamurthi R: Primary intrasellar
schwannoma. J Clin Neurosci. 19:1584–1585. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Mohammed S, Kovacs K, Munoz D and Cusimano
MD: A short illustrated review of sellar region schwannomas. Acta
Neurochir (Wien). 152:885–891. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Park HW, Jung S, Jung TY and Moon KS:
Intra-suprasellar schwannoma originating from the diaphragma
sellae. J Korean Neurosurg Soc. 45:375–377. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Koutourousiou M, Seretis A and
Kontogeorgos G: Intra-sellar schwannoma co-existing with
GH-secreting pituitary adenoma. Acta Neurochir (Wien).
151:1693–1697. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Krayenbühl N, Heppner F, Yonekawa Y and
Bernays RL: Intrasellar malignant peripheral nerve sheath tumor
(MPNST). Acta Neurochir (Wien). 149:201–206. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Moreland DB: Intrasellar pituitary
schwannoma. J Clin Neurosci. 13:771–774. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Honegger J, Koerbel A, Psaras T, Petrick M
and Mueller K: Primary intrasellar schwannoma: Clinical,
aetiopathological and surgical considerations. Br J Neurosurg.
19:432–438. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Perez MT, Farkas J, Padron S, Changus JE
and Webster EL: Intrasellar and parasellar cellular schwannoma. Ann
Diagn Pathol. 8:142–150. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Esposito F, Cappabianca P, Del Basso De,
Caro M, Cavallo LM, Rinaldi C and De Divitiis E: Endoscopic
endonasal transsphenoidal removal of an intra-suprasellar
schwannoma mimicking a pituitary adenoma. Minim Invasive Neurosurg.
47:230–234. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Maartens NF, Ellegala DB, Vance ML, Lopes
MB and Laws ER Jr: Intrasellar schwannomas: Report of two cases.
Neurosurgery. 52:1200–1206. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Whee SM, Lee JI and Kim JH: Intrasellar
schwannoma mimicking pituitary adenoma: A case report. J Korean Med
Sci. 17:147–150. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Bhagat S, Smith C, Teasdale GM and
McFadzean RM: Nerve sheath tumors of the sellar region. J
Neuroophthalmol. 22:275–278. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Civit T, Pinelli C, Klein M, Auque J,
Baylac F and Hepner H: Intrasellar schwannoma. Acta Neurochir
(Wien). 139:160–161. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wilberger JE Jr: Primary intrasellar
schwannoma: Case report. Surg Neurol. 32:156–158. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Perone TP, Robinson B and Holmes SM:
Intrasellar schwannoma: Case report. Neurosurgery. 14:71–73. 1984.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Chang CYI, Luo CB, Teng MM, Guo WY, Chen
SS, Lirng JF and Chang FC: Computed tomography and magnetic
resonance imaging characteristics of giant pituitary adenomas. J
Formos Med Assoc. 99:833–838. 2000.PubMed/NCBI
|
|
19
|
Bleys RL, Janssen LM and Groen GJ: The
lateral sellar nerve plexus and its connections in humans. J
Neurosurg. 95:102–110. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Dietemann JL, Kehrli P, Maillot C, Diniz
R, Reis M Jr, Neugroschl C and Vinclair L: Is there a dural wall
between the cavernous sinus and the pituitary fossa? Anatomical and
MRI findings. Neuroradiology. 40:627–630. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Penfield W: Intracerebral vascular nerves.
Arch Neurol Psychiatry. 21:92–94. 1958.
|
|
22
|
Wong ST, Moes G, Ernest K, Zovickian J,
Kim JY and Pang D: Innervation of the brain, intracerebral Schwann
cells and intracerebral and intraventricular schwannomas. Childs
Nerv Syst. 30:815–824. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ishihara M, Miyagawa-Hayashino A,
Nakashima Y, Haga H, Takahashi JA and Manabe T: Intracerebral
schwannoma in a child with infiltration along perivascular spaces
resembling meningioangiomatosis. Pathol Int. 59:583–587. 2009.
View Article : Google Scholar : PubMed/NCBI
|