Introduction
Total laparoscopic pylorus-preserving
pancreatoduodenectomy (tLPPPD) was first described by Gagner and
Pomp in 1994 (1). Due to the
complicated surgical procedure, tLPPPD is only performed in a few
highly specialized hospitals. For pancreatic malignant diseases
located in the head or uncinate process, tLPPPD has been
demonstrated to be a safe and feasible surgery (2). Previous studies showed a 1.6–1.8% rate
of mortality, perioperatively, in laparoscopic
pancreaticoduodenectomy (LPD) (1,2), which is
similar to the 1% mortality rate associated with tLPPPD (3). Alternatives to tLPPPD include LPD,
robot-assisted pancreaticoduodenectomy and hand-assisted
pancreaticoduodenectomy. tLPPPD provides several advantages,
including minimal invasion, lower blood loss and a shorter hospital
stay, compared with traditional open pancreatoduodenonectomy
(4). tLPPPD is most commonly
performed in non-elderly patients (5). To date, few reports on the outcomes of
tLPPPD performed in elderly patients, particularly those >80
years, have been published (6).
Theoretically, age may be a significant prognostic factor for
patients who undergo such complex surgery. An older age often
indicates a worse tolerance for surgery, worse pre-operative
conditions and a slower recovery. The present study reports a case
of tLPPPD that was performed in an 89-year-old man and shares the
experience of the West China Hospital (Chengdu, Sichuan, China) in
treating such elderly patients.
Case report
An 89-year-old man was admitted to the Department of
Hepatopancreatobiliary Surgery of West China Hospital in January
2014 with a 1-month history of jaundice. The physical examination
was unremarkable, with the exception of skin and sclera jaundice.
Laboratory results showed a total bilirubin (TB) level of 88.7
µmol/l (normal range, 5.0–28.0 µmol/l), a direct bilirubin (DBIL)
level of 81.0 µmol/l (normal range, <8.8 µmol/l), a carbohydrate
antigen 19–9 level of 581.1 U/ml (normal range, <22 U/ml) and a
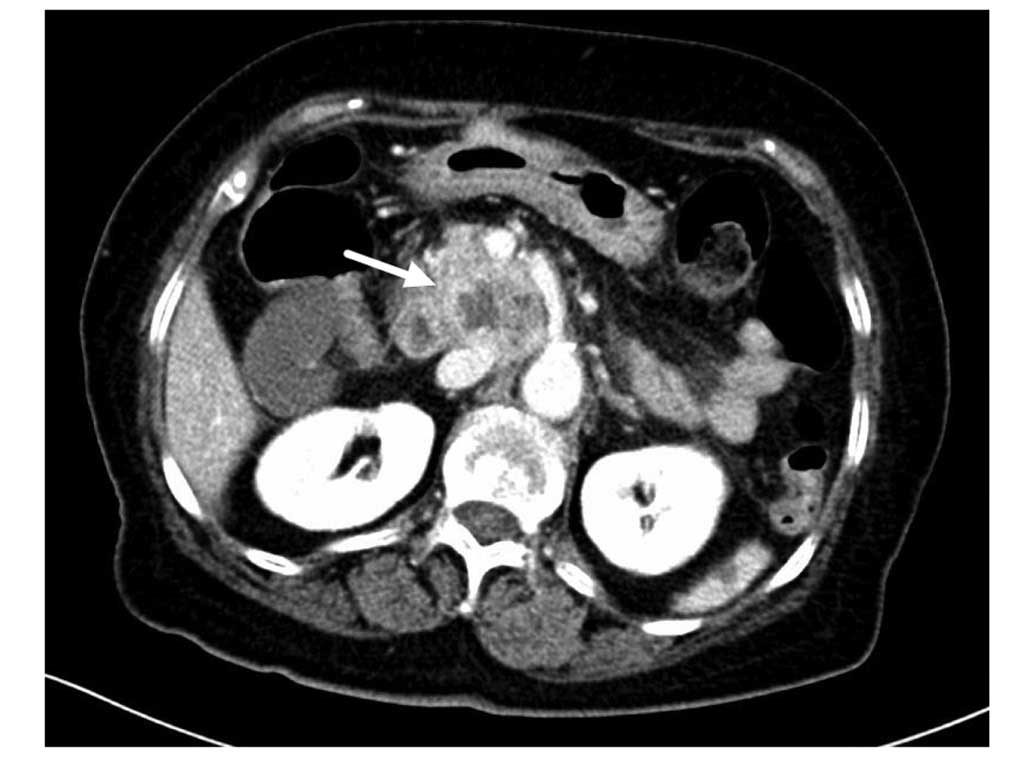
normal coagulation test result. Upper abdominal computed tomography
(Brilliance 64 Slice CT; Philips Medical Systems, Cleveland, OH,
USA) scans showed dilation of the intrahepatic and common bile
ducts. An arterial enhanced 3.5×4.8–cm mass was detected in the
uncinate process, without evidence of superior mesenteric vessel
invasion (Fig. 1). A malignant tumor
of the uncinate process, with obstructive jaundice, was diagnosed
pre-operatively. Due to a 10-year history of hypertension, an
electrocardiogram, cardiac ultrasonography test and pulmonary
function test were adapted to evaluate the patient. An atrial
septal defect and atrial flutter were detected. Moderate
cardiopulmonary impairment was subsequently diagnosed. tLPPPD is
routinely performed for elderly patients >70 years in the West
China Hospital. Considering the high age and unsatisfactory
pre-operative conditions of the present patient, tLPPPD was
performed. For tLPPPD, the patients was placed in supine position
with an anti-Trendelenberg (10–30 cm) position. Abdominal pressure
using CO2 gas insufflation was maintained at 13–14 mmHg
and four trocars were placed under a direct vision scope. Then
resection and reconstruction began For the resection, the
gastrocolic omentum was dissected to allow entry into the lesser
sac. The right gastroepiploic vessels were transected and the
superior mesenteric portal vein was identified at the inferior
border of the pancreas. The duodenum was mobilized and divided to
the pylorus using an endoscopic linear stapler. A cholecystectomy
was performed separately and the common bile duct and common
hepatic artery were dissected. The gastroduodenal artery and the
right gastric artery were transected. The pancreas was divided at
the neck, while the pancreatic duct was identified for
reconstruction. The jejunum was divided 10–15 cm distal to the
Treitz ligament with an endoscopic linear stapler and the uncinate
process was divided from superior mesenteric artery to complete the
resection. For the reconstruction, the pancreaticojejunostomy was
carried out using the duct-to-mucosa method (2). A laparoscopic choledochojejunostomy and
gastrojejunostomy were performed with running suturing. During the
surgery, ~50 ml of pale yellow ascites was observed. No invasion of
the superior mesenteric vessels and no metastasis to the abdominal
organs was detected. Only mild swelling in the head of pancreas was
present. A tLPPPD R0 resection and lymphadenectomy were
successfully achieved.
At post-operative day 1 (POD 1), the laboratory
results showed a TB level of 53.5 µmol/l and a DBIL level of 50.2
µmol/l. The drainage amylase test reached a peak level of 1583 IU/l
(normal range, ≤3 times level of serum amylase) with normal vital
signs at POD 2. The TB level had decreased to a normal level of
27.5 µmol/l at POD 10, with a low level of drainage amylase of 130
IU/l at POD 4. According to the Clavien grading system (7), no fatal complications, including heart
failure, pulmonary infection, hemorrhage, pancreatic leakage and
bile leakage, were observed, with the exception of grade I
pancreatic leakage at POD 2. The post-operative pathological
examination revealed a moderately-differentiated adenocarcinoma
involving the pancreatic parenchyma (8), and negative findings in the lymph nodes.
The tissues were sent to a pathologist at the West China Hospital,
Sichuan University, for assessment by immunohistochemical staining.
Immunohistochemical staining with hematoxylin and eosin revealed
that the adenocarcinoma cells originated from pancreatic ductal
epithelial cells, due to testing positive for the S100 protein and
maspin and negative for CD10. The patient was uneventfully
discharged at POD 12 with a diagnosis of pancreatic uncinate
adenocarcinoma [T2N0M0, stage IB, according to the Clavien grading
system (9)]. During 2 years of
follow-up, abdominal enhanced magnetic resonance imaging and blood
tumor markers revealed that the patient had no tumor recurrence or
metastasis.
Discussion
Despite its complexity, tLPPPD has been reported to
be a safe and feasible surgery following improvements in
laparoscopic technology and greater surgical experience (5). Previous studies have shown a 1.6–8.0%
rate of perioperative mortality (10,11). While
for low-grade malignant pancreatic head disease cases, the
mortality rate for tLPPPD is comparable with the historical data
for patients who underwent open pancreatoduodenectomy (5). The majority of studies with large series
of patients with advanced periampullary malignant diseases present
comparable findings in the oncological outcomes between tLPPPD and
open pancreatodudenectomy (2).
Palanivelu et al (10)
reported a mean of 13 lymph nodes harvested and a 5-year survival
rate of 32% for all patients. In addition, these authors noted a
5-year survival rate of 31.7% for periampullary adenocarcinoma,
33.3% for pancreatic cystadenocarcinoma, 19.1% for pancreatic head
adenocarcinoma and 50.0% for common bile duct adenocarcinoma. For
45 patients with advanced periampullary malignancies, Kendrick and
Cusati (2) reported the retrieval of
15 median lymph nodes with an 89% margin-negative resection, a 16%
rate for hepatic or pulmonary recurrence within a mean period of
7.4 months, and no port-site recurrence. Additional details
concerning studies that have reported patients treated with tLPPPD
are revealed in Table I.
 | Table I.Previous studies that treated patients
with total laparoscopic pylorus-preserving
pancreatoduodenectomy. |
Table I.
Previous studies that treated patients
with total laparoscopic pylorus-preserving
pancreatoduodenectomy.
| Authors | n | Conversion, % | Mortality, n | Operation time,
min | Pancreatic fistula,
% | Hospital stay,
days | Negative-margin
resection, % | Reference |
|---|
| Palanivelu et
al, 2007 | 75 | 0 | 1 | 357 | 7 | 8 | 97 | (10) |
| Dulucq et al,
2006 | 13 | NA | 1 | 295 | 8 | 16 | 100 | (11) |
| Zureikat et
al, 2011 | 14 | 14.0 | 1 | 456 | 36 | 8 | 100 | (3) |
| Kendrick and Cusati,
2010 | 65 | 4.6 | 1 | 368 | 18 | 7 | 89 | (2) |
| Kim et al,
2013 | 105 | 4.7 | 1 | 474 | 6 | 11 | 100 | (5) |
In the past, an age of >80 years may have been
considered as a contradiction for complex surgeries, such as
pancreatoduodenonectomy, hepatectomy and organ transplantations.
Elderly patients theoretically have a lower capability to tolerate
complex procedures. The impairment of heart and pulmonary reserve
function often leads to a high risk of post-operative
cardiopulmonary complications. Additionally, with a soft pancreas
and small pancreatic duct, this group of patients may experience
pancreatic leakage, which is extremely detrimental. In the present
case, due to an early diagnosis and mild jaundice, a soft pancreas
and nearly normal pancreatic duct were detected during the surgery,
and an end-to-side pancreaticojejunostomy was successfully
performed. A slight increase in the drainage amylase level at POD 2
quickly decreased to a normal level at POD 4. This may have been a
result of the surgeon's experience with the applied technology,
which extended to >50 tLPPPD cases. The surgical duration was
6.5 h and no blood transfusion was necessary. From experience of
another 4 successful cases of tLPPPD performed early last year in
patients >75 years old (Table
II), and despite the pre-operative impairment of
cardiopulmonary function, we hypothesize that four potential
factors may be responsible for the good outcome of the present
89-year-old patient: i) Experience in the relevant surgical skills;
ii) a short surgical duration; iii) advanced post-operative
cardiopulmonary management, and iv) similar to previous studies
(5,11), a moderately-differentiated
adenocarcinoma that is not a contraindication for tLPPPD. In
conclusion, tLPPPD is safe and feasible in selective elderly
patients. Use of this technique may expand the number of patients
who can undergo surgery and provide benefits to these patients.
| Table II.Elderly patients treated with total
laparoscopic pylorus-preserving pancreatoduodenectomy at the West
China Hospital, Sichuan University (Chengdu, China). |
Table II.
Elderly patients treated with total
laparoscopic pylorus-preserving pancreatoduodenectomy at the West
China Hospital, Sichuan University (Chengdu, China).
| Patient | Age, years | Conversion | Mortality | Operation time,
min | Pancreatic
fistula | Hospital stay,
days | Margin-negative
resection | Blood
transfusion |
|---|
| 1 | 77 | No | No | 488 | No | 12 | Yes | No |
| 2 | 78 | No | No | 436 | No | 10 | Yes | No |
| 3 | 81 | No | No | 420 | No | 13 | Yes | No |
| 4 | 83 | No | No | 408 | No | 10 | Yes | No |
| 5 | 89 | No | No | 420 | No | 12 | Yes | No |
Glossary
Abbreviations
Abbreviations:
|
tLPPPD
|
total laparoscopic pylorus-preserving
pancreatoduodenectomy
|
|
POD
|
post-operative day
|
References
|
1
|
Gagner M and Pomp A: Laparoscopic
pylorus-preserving pancreatoduodenectomy. Surg Endosc. 8:408–410.
1994. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kendrick ML and Cusati D: Total
laparoscopic pancreaticoduodenectomy: Feasibility and outcome in an
early experience. Arch Surg. 145:19–23. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Zureikat AH, Breaux JA, Steel JL and
Hughes SJ: Can laparoscopic pancreaticoduodenectomy be safely
implemented? J Gastrointest Surg. 15:1151–1157. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Asbun HJ and Stauffer JA: Laparoscopic vs.
Open pancreaticoduodenectomy: Overall outcomes and severity of
complications using the Accordion Severity Grading System. J Am
Coll Surg. 215:810–819. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kim SC, Song KB, Jung YS, Kim YH, Park Do
H, Lee SS, Seo DW, Lee SK, Kim MH, Park KM and Lee YJ: Short-term
clinical outcomes for 100 consecutive cases of laparoscopic
pylorus-preserving pancreatoduodenectomy: Improvement with surgical
experience. Surg Endosc. 27:95–103. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tee MC, Croome KP, Shubert CR, Farnell MB,
Truty MJ, Que FG, Reid-Lombardo KM, Smoot RL, Nagorney DM and
Kendrick ML: Laparoscopic pancreatoduodenectomy does not completely
mitigate increased perioperative risks in elderly patients. HPB
(Oxford). 17:909–918. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Clavien PA, Camargo CA Jr, Croxford R,
Langer B, Levy GA and Greig PD: Definition and classification of
negative outcomes in solid organ transplantation. Application in
liver transplantation. Ann Surg. 220:109–120. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hruban RH, Adsay NV, Albores-Saavedra J,
Compton C, Garrett ES, Goodman SN, Kern SE, Klimstra DS, Klöppel G,
Longnecker DS, et al: Pancreatic intraepithelial neoplasia: A new
nomenclature and classification system for pancreatic duct lesions.
Am J Surg Pathol. 25:579–586. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Clavien PA, Camargo CA Jr..Croxford R,
Langer B, Levy GA and Greig PD: Definition and classification of
negative outcomes in solid organ transplantation. Application in
liver transplantation. Ann Surg. 220:109–120. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Palanivelu C, Jani K, Senthilnathan P,
Parthasarathi R, Rajapandian S and Madhankumar MV: Laparoscopic
pancreaticoduodenectomy: Technique and outcomes. J Am Coll Surg.
205:222–230. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Dulucq JL, Wintringer P and Mahajna A:
Laparoscopic pancreaticoduodenectomy for benign and malignant
diseases. Surg Endosc. 20:1045–1050. 2006. View Article : Google Scholar : PubMed/NCBI
|