Introduction
Lung cancer is the number one cause of
cancer-associated mortality (1). The
high mortality rates associated with lung cancer are largely due to
the poor outcomes of conventional treatments, including the use of
surgical removal combined with adjuvant radiation and chemotherapy
(2). Significant improvements have
been achieved due to increased efforts to determine the molecular
mechanisms underlying tumorigenesis, which has led to the
identification of multiple oncogenic alterations, including those
observed in epidermal growth factor receptor (EGFR)
(3), Kirsten rat sarcoma viral
oncogene homolog (KRAS) (4),
B-Raf proto-oncogene, serine/threonine kinase (BRAF)
(5), anaplastic lymphoma kinase
(ALK) (6), ROS proto-oncogene
1 (7) and ret proto-oncogene
(RET) (7–9). It was previously demonstrated that
patients carrying EGFR mutations exhibited a significant
response to the EGFR tyrosine kinase inhibitors (TKIs) gefitinib
and erlotinib as a first-line therapy (3,10). By
contrast, patients carrying ALK fusions exhibited a poor
response to these drugs (11), but
responded well to the ALK TKI crizotinib (12). Thus, targeted treatment based on the
results of molecular and pathological diagnosis has become a new
standard for the treatment of lung cancer (13).
Although the majority of lung cancer cases are
associated with an extensive history of cigarette smoking, the
prevalence of lung cancer death in non-smokers remains high
(14). In the United States, 10–15%
of lung cancer cases are diagnosed in patients who are considered
never-smokers (15). If listed as a
separate category, lung cancer in never-smokers would rank among
the top 10 most commonly observed fatal cancer cases in the United
States (14,16). This ranking in never-smokers is likely
to rise due to increased public awareness of the life-threatening
hazards caused by cigarette smoking, resulting in a drop in the
population of smokers and thus an increase in the population of
never-smokers (17).
A previous clinical study demonstrated that targeted
therapy in never-smoker lung cancer patients typically produces an
improved response compared with that in smokers (18). It has been suggested that the
molecular profiles of lung cancer cases are likely to vary between
heavy smokers and never-smokers. Accumulating evidence based on
molecular and clinicopathological studies has suggested that
non-small cell lung cancer (NSCLC) in never-smokers should be
considered as a distinct entity (19). Thus, it is critical to determine the
mutation state of NSCLC in never-smokers as a unique type of
cancer, for the purpose of cancer research and clinical
translation. With this aim in mind, the present study performed a
large-scale screen for tumorigenic alterations in the oncogenes
EGFR, KRAS, BRAF ALK and RET in 358
Chinese NSCLC adenocarcinoma patients who were exclusively
never-smokers. The clinicopathological characteristics associated
with these genetic alterations were additionally determined. The
present study may yield a clear picture concerning the molecular
profile of NSCLC in never-smokers, thus providing valuable
information for cancer research and the improvement of targeted
therapies for the treatment of NSCLC.
Materials and methods
Specimen collection
The present study was approved by the Institutional
Review Boards of Shanghai Chest Hospital, Shanghai Jiao Tong
University (Shanghai, China), and Chongqing Cancer Institute
(Chongqing, China). All participants underwent lung resection and
needle aspiration, and provided written informed consent. Samples
were snap-frozen with liquid nitrogen at the time of resection and
stored at −80°C until required. All cases were independently
reviewed by two pathologists during disease diagnosis. Patients
were considered never-smokers if they had never smoked or had
smoked <100 cigarettes in their lifetime (15).
Detection of mutations in EGFR, KRAS
and BRAF
Genomic DNA was extracted with the QIAamp DNA
formalin-fixed paraffin-embedded (FFPE) kit (Qiagen, Inc.,
Valencia, CA, USA) according to the manufacturer's protocols. EGFR,
KRAS and BRAF mutations were detected by amplification refractory
mutation system in multiple quantitative polymerase chain reaction
(ARMS-multi-qPCR) analysis with the Human EGFR Mutation Detection
kit (YuanQi Bio-Pharmaceutical Co., Ltd., Shanghai, China) and the
Human KRAS and BRAF Mutation Detection kit (YuanQi
Bio-Pharmaceutical Co., Ltd.), respectively. The PCR conditions
used were as follows: 42°C for 5 min, 94°C for 3 min, followed by
40 cycles at 94°C for 15 sec and 60°C for 1 min on the 7500
Real-Time PCR System (Applied Biosystems; Thermo Fisher Scientific,
Inc., Waltham, MA, USA). The following primers were used: EGFR-exon
(E)18 forward, 5′-CAAGTGCCGTGTCCTGG-3′ and reverse,
5′-CCTTACCTTATACACCGTGCC-3′; EGFR-E19 forward,
5′-CGGTGCATCGCTGGTAACAT-3′ and reverse, 5′-ATGGACCCCCACACAGC-3′;
EGFR-E20 forward, 5′-CTGGCCACCATGCGAAG-3′ and reverse,
5′-TCCTGGCTCCTTATCTCCC-3′; EGFR-E21 forward,
5′-GCTTCTTCCCATGATGATCTG-3′ and reverse, 5′-CTGGTCCCTGGTGTCAGG-3′;
KRAS forward, 5′-TTTGTATTAAAAGGTACTGGTGG-3′ and reverse,
5′-CCTCTATTGTTGGATCATATTCG-3′; and BRAF forward,
5′-ACTCTTCATAATGCTTGCTCTG-3′ and reverse,
5′-TGAATACTGGGAACTATGAAAATAC-3′. All PCR products were subjected to
direct sequencing to verify mutations in EGFR, KRAS and BRAF. The
following probes were used: for EGFR-E18,
5′-GGTGACCCTTGTCTCTGTGTTC-3′; EGFR-E19, 5′-ATCACTGGGCAGCATGTG-3′;
EGFR-E20, 5′-CCCTGATTACCTTTGCGAT-3′; EGFR-E21,
5′-TGATCTGTCCCTCACAGCAG-3′; KRAS, 5′-TGTATTAAAAGGTACTGGTGGAG-3′;
and BRAF 5′-TGAGACCTTCAATGACTTTCTAG-3′. All primers and
probes were purchased from Sangon Biotech Co., Ltd., Shanghai,
China.
Detection of ALK and RET fusion
variants
Multiplex one-step reverse transcription (RT)-PCR
was performed to detect ALK fusion gene variants. The Human Lung
Cancer Related Fusion Gene Detection kit (YuanQi Bio-Pharmaceutical
Co., Ltd.) was used according to the manufacturer's protocols. In
brief, the mixture for each reaction contained 3 µl total RNA
extracted from the tumor specimen, 12 µl Multiplex RT-PCR buffer,
2.5 µl Multiplex Enzyme mix and 300 nmol/l primers in a total
volume of 25 µl. The PCR conditions used were as follows: 42°C for
30 min, 94°C for 5 min, followed by 40 cycles at 94°C for 15 sec
and 60°C for 1 min on the 7500 Real Time PCR System. A total of two
experiments were performed separately to detect echinoderm
microtubule-associated protein-like 4 (EML4)-ALK fusion or
alternative ALK fusions [transforming growth factor (TGF)-ALK,
kinesin light chain 1 (KLC1)-ALK and kinesin family member 5B
(KIF5B)-ALK]. The following forward primers were used for detecting
EML4-ALK variants: EML4-E2 (V5a and 5b) forward,
5′-GTGGCCTCAGTGAAAAAATC-3′; EML4-E6 (V3a and 3b) forward,
5′-TAAAGATGTCATCATCAACCAAG-3′; EML4-E13 (V1 and 6) forward,
5′-CCTGGGAAAGGACCTAAAG-3′; EML4-E14 (V4b and 7) forward,
5′-GGGAAAGGACCTAAAGGTG-3′; EML4-E15 (V4a) forward,
5′-TGATGGCTTCCAAATAGAAGTAC-3′; EML4-E17 (V9) forward,
5′-ACGGGAATGAACAGCTCTCT-3′; and EML4-E20 (V2) forward,
5′-CGGGAGACTATGAAATATTGTACT-3′. The primers for alternative ALK
fusion variants included: TGF-E3 forward,
5′-GAGAACCAGGACCTTCCACC-3′; KLC1-E9 forward,
5′-ATTCTCACTCGTGCACATGAAA-3′; KIF5B-E15 forward,
5′-AAAAGACCTTGCAGAAATAGGAA-3′; KIF5B-E17 forward,
5′-TCTGTCGATGCCCTCAGTG-3′; and KIF5B-E24 forward,
5′-TCAGGTCAAAGAATATGGCCA-3′. The common reverse primer for all ALK
fusion variants was 5′-GCTTGTACTCAGGGCTCTGC-3′. Multiplex One-step
RT-PCR was additionally used to detect RET fusion variants,
including KIF5B-RET and coiled-coil domain containing 6
(CCDC6)-RET. RET Fusion Gene Detection kit (YuanQi
Bio-Pharmaceutical Co., Ltd.) was used according to the
manufacturer's protocols. All PCR products were subjected to DNA
sequencing with the probe 5′-AGCTCCTGGTGCTTCCGGCG-3′ for all ALK
fusion products. The expression of ALK tyrosine kinase was examined
by immunohistochemistry using the ALK (D5F3) CDx Assay kit (Ventana
Medical Systems, Inc., Tucson, AZ, USA) containing the rabbit
monoclonal antibody against ALK (clone D5F3; catalog no., 790–4796;
dilution, 1:250), which detected endogenous levels of total ALK
protein, as well as ALK fusion proteins. The experiments were
performed on FFPE sections, as described previously (20).
Statistical analysis
P-values were determined by Fisher's exact test or
χ2 test using Prism 6 analysis software (GraphPad
Software, Inc., La Jolla, CA, USA). P<0.05 and P<0.01 were
considered to indicate a statistically significant and highly
significant difference, respectively.
Results
Clinical characteristics of enrolled
patients
Between January 2012 and June 2013, resected lung
adenocarcinoma samples were collected from a total of 358 patients
who had been diagnosed with NSCLC at Shanghai Chest Hospital or
Chongqing Cancer Institute. The cohort consisted of 274 female
patients (76.5%) and 84 male patients (23.5%) (Table I). The median age of the patient
cohort was 57.1 years. While ~36.3% of patients were 50–59 years
old, and 41.6% were ≥60 years, only 22.1% of patients were <50
years old (Table I). All specimens
were selected based on the following criteria: i) Re-review
confirmed a pathological diagnosis of lung adenocarcinoma; ii) the
tumor specimen contained a minimum of 70% tumor cells; iii)
sufficient tissue was available for comprehensive analysis; iv) the
patient was a never-smoker; and v) the patient did not receive any
neoadjuvant treatment. Based on the differentiation level of cancer
cells, the specimens could be divided into three groups, which
comprised poorly-, moderately- or well-differentiated carcinoma.
The number of specimens was similar among these groups, ranging
from 32.1 to 35.8% (Table I).
 | Table I.Clinical characteristics of 358
never-smokers with non-small cell lung cancer. |
Table I.
Clinical characteristics of 358
never-smokers with non-small cell lung cancer.
| Variable | Patients, n
(%) |
|---|
| Gender |
|
|
Male | 84
(23.5) |
|
Female | 274 (76.5) |
| Age, years |
|
|
<40 | 5
(1.4) |
|
40–49 | 74
(20.7) |
|
50–59 | 130 (36.3) |
|
≥60 | 149 (41.6) |
|
Differentiation |
|
|
Poorly | 115 (32.1) |
|
Moderately | 128 (35.8) |
|
Well | 115 (32.1) |
Mutations were detected in EGFR, KRAS,
BRAF, EML4-ALK and KIF5B-RET
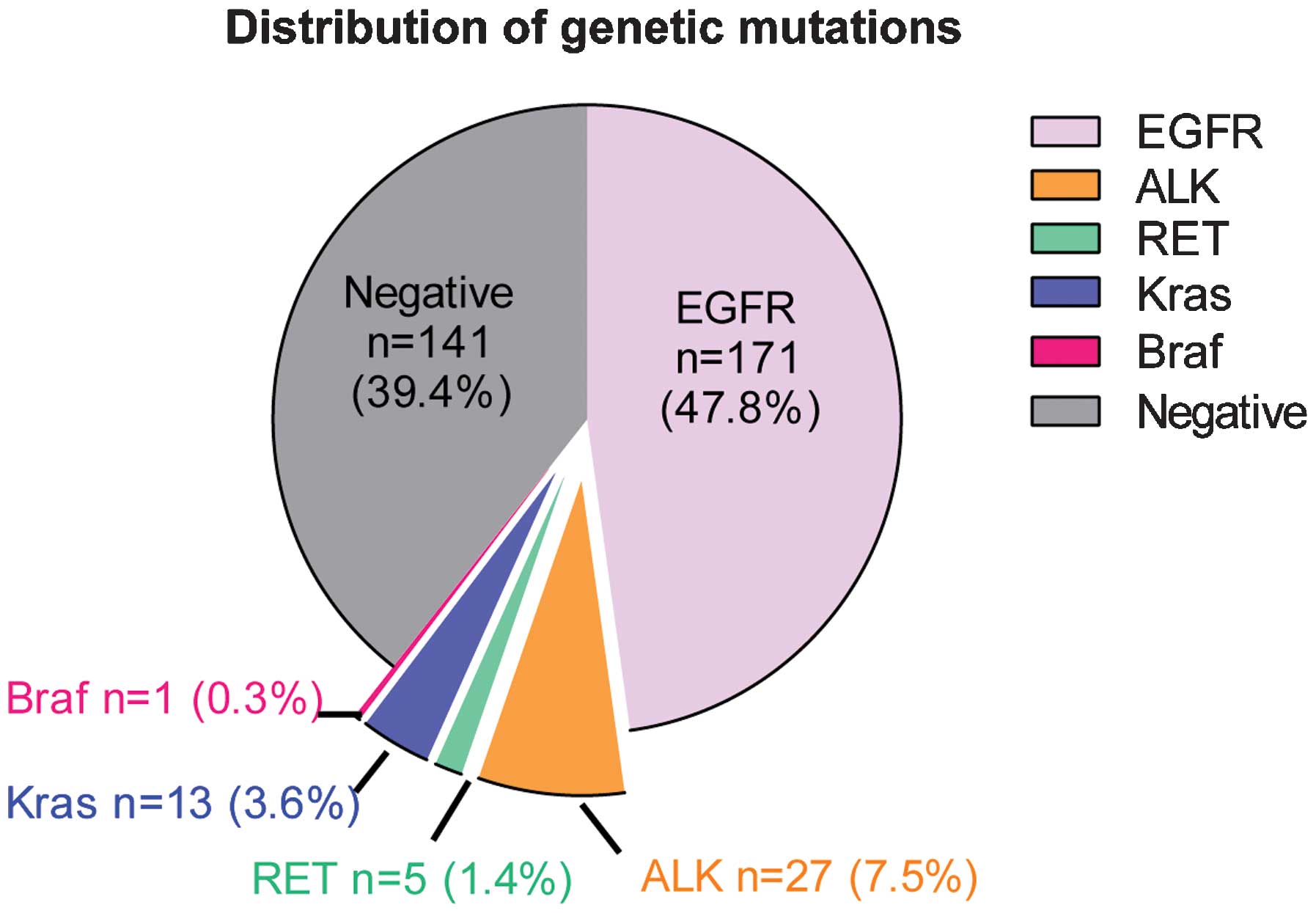
Out of a total of 358 NSCLC patents, genetic
alterations were detected in 217 carcinoma specimens. Among these
positive cases, there were 171 patients carrying EGFR mutations,
accounting for 47.8% of all patients (Fig. 1). A total of 27 patients were detected
as exhibiting EML4-ALK fusion genes, 13 with KRAS mutations, 5 with
KIF5B-RET fusion variants and 1 with BRAF mutations, accounting for
7.5, 3.6, 1.4 and 0.3%, respectively (Fig. 1). No KIF5B-ALK or TFG-ALK fusion
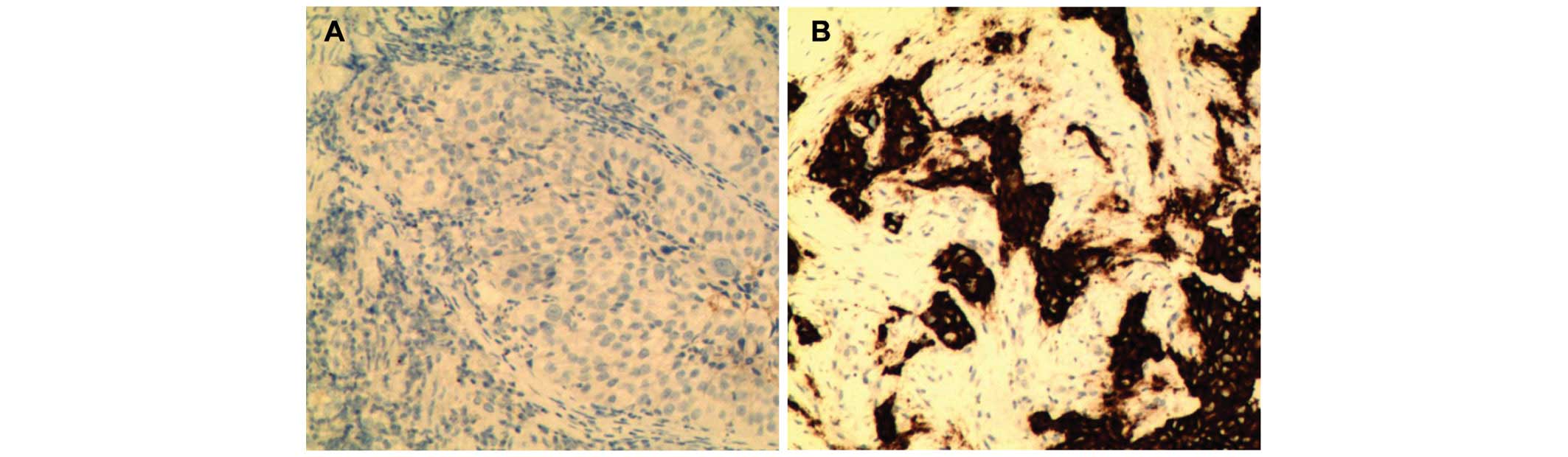
variants were detected in the samples. These results were confirmed
by immunohistochemistry. Representative images revealed that ALK
was absent in EML4-ALK-negative carcinoma cases (Fig. 2A), but was highly expressed in
EML4-ALK-positive samples (Fig. 2B).
None of the specimens carried mutations in >1 gene. However,
there was one patient (>60 years old) who carried two EGFR
mutations (E19 and E21) in their tumor specimen. These results
supported the observation that mutations in the investigated
tumorigenic genes are typically mutually exclusive (21).
EGFR mutations were most prevalent in E19,
with 102 cases, accounting for 28.5% of all patients and 59.6% of
patients exhibiting EGFR mutations (Table II). EGFR mutations were
additionally identified frequently in E21, with 63 cases,
accounting for 17.6% of all patients and 36.8% of patients with
EGFR mutations (Table II).
Markedly fewer cases were detected with mutations in E18 (3 cases;
0.8% of all patients) or E20 (4 cases; 1.1% of all patients),
accounting for <5% of combined patients exhibiting EGFR
mutations (Table II). Detailed data
is listed in Table II according to
gender, age, differentiation and histology.
| Table II.Characterization of EGFR mutations in
358 Chinese never-smokers exhibiting non-small cell lung
cancer. |
Table II.
Characterization of EGFR mutations in
358 Chinese never-smokers exhibiting non-small cell lung
cancer.
|
| All EGFR | E18 | E19 | E20 | E21 |
|---|
|
|
|
|
|
|
|
|---|
| Variable | n | % | n | % | n | % | n | % | n | % |
|---|
| Gender |
|
|
Male | 30 | 35.7 | 0 | 0.0 | 18 | 21.4 | 0 | 0.0 | 12 | 14.3 |
|
Female | 141 | 51.5 | 3 | 1.1 |
84a | 30.7 | 4 | 1.5 |
51a | 18.6 |
| Age, years |
|
|
<40 | 0 |
0.0 | 0 | 0.0 | 0 |
0.0 | 0 | 0.0 | 0 |
0.0 |
|
40–49 | 32 | 43.2 | 1 | 1.4 | 19 | 25.7 | 1 | 1.4 | 11 | 14.9 |
|
50–59 | 60 | 46.2 | 1 | 0.8 | 38 | 29.2 | 2 | 1.5 | 19 | 14.6 |
|
≥60 | 79 | 53.0 | 1 | 0.7 |
45a | 30.2 | 1 | 0.7 |
33a | 22.1 |
| Diff |
|
|
Poorly | 56 | 48.7 | 2 | 1.7 | 36 | 31.3 | 1 | 0.9 | 17 | 14.8 |
|
Mod | 51 | 39.8 | 1 | 0.8 |
28a | 21.9 | 2 | 1.6 |
21a | 16.4 |
|
Well | 64 | 55.7 | 0 | 0.0 | 38 | 33.0 | 1 | 0.9 | 25 | 21.7 |
| Total | 171 | 47.8 | 3 | 0.8 |
102a | 28.5 | 4 | 1.1 |
63a | 17.6 |
Gender may affect the occurrence of
oncogenic mutations
Subgroup analysis was performed in order to uncover
clinical features that were associated with the identified genetic
mutations in the present study (Table
III). In order to determine whether gender affected the
frequency of investigated tumorigenic mutations in the present
patient cohort, subtype analysis was performed according to patient
gender, as shown in Table III. The
percentage of patients who possessed EGFR mutations was 35.7%
(30/84) of male patients and 51.5% (141/274) of female patients.
The difference in the number of patients with or without EGFR
mutations between male (30 vs. 54) and female (141 vs. 133)
patients was markedly significant (P<0.01), suggesting that
gender is an important factor that may affect EGFR mutations in
NSCLC in never-smokers. Thus, EGFR mutations were more likely to be
detected in female patients compared with male patients in the
subset of NSCLC exhibited by never-smokers. Using an identical
analysis method, a significant difference was observed (P<0.05)
in the prevalence of KRAS mutations between male and female
patients. The frequency of KRAS mutations was 7.1% in male patients
and 2.6% in female patients. No significant difference was observed
in the prevalence of mutations for ALK, RET and BRAF genes between
male and female patients, suggesting that gender may have no
significant effect on these mutations in NSCLC in
never-smokers.
| Table III.Characteristics of genetic mutations
in 358 never-smokers with non-small cell lung cancer. |
Table III.
Characteristics of genetic mutations
in 358 never-smokers with non-small cell lung cancer.
|
| EGFR | ALK | KRAS | RET | BRAF |
|---|
|
|
|
|
|
|
|
|---|
| Variable | −, n (%) | +, n (%) | P-value | −, n (%) | +, n (%) | P-value | −, n (%) | +, n (%) | P-value | −, n (%) | +, n (%) | P-value | −, n (%) | +, n (%) | P-value |
|---|
| Frequency | 187 (52.5) | 171 (47.8) |
| 331 (92.5) | 27
(7.5) |
| 345 (96.4) | 13 (3.6) |
| 353 (98.6) | 5 (1.4) |
| 357 (99.7) | 1 (0.3) |
|
| Gender |
|
|
Male | 54
(64.3) | 30
(35.7) | 0.01 | 78
(92.9) | 6
(7.1) | 0.87 | 78
(92.9) | 6 (7.1) | 0.05 | 84
(100.0) | 0 (0.0) | 0.21 | 84
(100.0) | 0 (0.0) | 0.58 |
|
Female | 133 (48.5) | 141 (51.5) |
| 253 (92.3) | 21
(7.7) |
| 267 (97.4) | 7 (2.6) |
| 269 (98.2) | 5 (1.8) |
| 273 (99.6) | 1 (0.4) |
|
| Age, years |
|
|
<40 | 5
(100.0) | 0 (0.0) | 0.04 | 3
(60.0) | 2
(40.0) | 0.0002 | 5
(100.0) | 0 (0.0) | 0.35 | 4
(80.0) | 1 (20.0) | 0.0001 | 5
(100.0) | 0 (0.0) | 0.82 |
|
40–49 | 42
(56.8) | 32 (43.2) |
| 63
(85.1) | 11 (14.9) |
| 73
(98.6) | 1 (1.4) |
| 70
(94.6) | 4 (5.4) |
| 74
(100.0) | 0 (0.0) |
|
|
50–59 | 70
(53.8) | 60 (46.2) |
| 121 (93.1) | 9 (6.9) |
| 124 (95.4) | 6 (4.6) |
| 130 (100.0) | 0 (0.0) |
| 129 (99.2) | 1 (0.8) |
|
|
≥60 | 70
(47.0) | 79 (53.0) |
| 144 (96.6) | 5 (3.4) |
| 143 (96.0) | 6 (4.6) |
| 149 (100.0) | 0 (0.0) |
| 149 (100.0) | 0 (0.0) |
|
| Diff |
|
|
Poorly | 59
(51.3) | 56 (48.7) | 0.05 | 105 (89.7) | 12 (10.3) | 0.004 | 112 (95.7) | 5 (4.3) | 0.75 | 114 (97.4) | 3 (2.6) | 0.24 | 116 (99.1) | 1 (0.9) | 0.36 |
|
Mod | 77
(60.2) | 51 (39.8) |
| 110 (88.7) | 14 (11.3) |
| 119 (96.0) | 5 (4.0) |
| 122 (98.4) | 2 (1.6) |
| 124 (100.0) | 0 (0.0) |
|
|
Well | 51
(44.3) | 64 (55.7) |
| 116 (99.1) | 1 (0.9) |
| 114 (97.4) | 3 (2.6) |
| 117 (100.0) | 0 (0.0) |
| 117 (100.0) | 0 (0.0) |
|
| Avg. age,
years |
| 57.7 |
|
| 54.4 |
|
| 59.3 |
|
| 42.8 |
|
| 58.0 |
Genetic mutations may be affected by
ageing
Subsequently, the effect of ageing on the occurrence
of oncogenic mutations was determined. Consistent with previous
reports (22,23), in the present study, EGFR mutations
were more likely to be identified in older patients compared with
younger patients. This was determined by comparing the distribution
in four age subgroups between patients with and without EGFR
mutations (P<0.04; Table III).
By contrast, mutations in KIF5B-RET and EML4-ALK were more likely
to be detected in younger patients compared with older patients, as
there was a significant difference in the distribution of patients
in four distinct age groups between wild-type and mutated KIF5B-RET
or EML4-ALK, respectively (P<0.001; Table III). The median age was 42.8±1.6
years in KIF5B-RET-positive patients or 54.4±0.6 years in
EML4-ALK-positive patients, compared with 57.9±0.8 years in
mutation-negative patients (Table
III). These results suggested a potential early onset of the
disease in the patients exhibiting KIF5B-RET or EML4-ALK mutations.
No evidence suggested that ageing was a significant factor in the
occurrence of mutations in KRAS and BRAF, as determined by Fisher's
exact test (Table III).
An association is present between
genetic mutations and the level of differentiation in cancer
The differentiation level of carcinoma cases was
examined, and it was identified that those expressing EML4-ALK were
more likely to be poorly- or moderately-differentiated, but not
well-differentiated, compared with mutation-negative patients
(P<0.01; Table III). By
comparing the differentiation level between tumors with and without
EGFR mutations, the cancer cells were more likely to be
well-differentiated in carcinoma exhibiting EGFR mutations compared
with wild-type carcinoma (P<0.05; Table III). The differentiation level of
carcinoma carrying alternative types of gene mutation was not
significantly different from the remaining patients. These results
suggested that ALK fusions activated cancer types that were less
differentiated, but that possessed a more rapid rate of growth and
were more resistant to conventional treatment. By contrast, EGFR
mutations demonstrated the opposite properties for these aspects.
The tumors were well-differentiated, with a slower rate of growth
and possessed an improved response to conventional treatment
(3,10). Therefore, screening for genetic
mutations and determining cell differentiation levels may be
important steps for improving the efficiency of targeted treatments
in NSCLC.
Discussion
Novel discoveries in the molecular genetics of
cancer have revolutionized the treatment of the disease by
replacing traditional methods with customized therapies based on
the clinical pathology and molecular diagnosis of genetic mutations
(13). Thus, it is crucial to
accurately determine tumorigenic alterations for the success of
subsequent treatments. NSCLC in never-smokers has been proposed to
be a distinct disease entity due to its unique molecular and
clinical properties (19). Although
the frequency of oncogenic mutations in never-smokers has been
investigated in a large number of studies, the results have been
varied and unclear, as never-smoker patients are typically included
as a small proportion of the investigated subjects together with a
relatively larger amount of smoker patients. In addition, only one
mutation at a time has been traditionally investigated in the
majority of these previous studies, thus avoiding a direct
comparison between various mutations among the same group of
patients, which may vary compared with other groups of patients in
molecular and clinical characteristics due to differences in race,
region, economy and environment. In order to overcome these
problems, a comprehensive study was performed to determine the
frequency of genetic alterations in five known oncogenes and their
associated clinical features in 358 NSCLC patients who were
exclusively never-smokers. Using this large-scale screen, a precise
molecular profile was generated concerning tumorigenic alterations
in NSCLC adenocarcinoma in never-smokers as a distinct disease
entity.
EGFR and KRAS represent the two most
frequently mutated genes in lung cancer, with a frequency of
>10% in each case (21). However,
the results of the present study indicated that only EGFR
was frequently mutated in never-smoker patients, while KRAS
and all other investigated genes were infrequently (<10%)
altered in this patient cohort. This supported the idea that NSCLC
in never-smokers is a distinct entity in NSCLC, at least with
regard to the state of oncogenic mutations. While the causes of
these de novo mutations remain to be elucidated, it is
agreed that various mutations may have specific impacts on
signaling pathways that regulate cellular proliferation and
survival (24). For research and
clinical purposes, types of cancer with infrequent tumorigenic
mutations, particularly those demonstrating poor responses to EGFR
TKIs and other targeted therapies, may be classified as rare
diseases requiring different attention and treatments. An improved
classification and diagnosis of lung cancer should consider
molecular profiling and pathological characteristics in
patients.
The present study reported that 47.8% of patients
(171/358) in the present cohort exhibited EGFR mutation(s),
which was similar to the results of a previous study reporting a
frequency of 49.8% in never-smoker patients (25). In the present study, there were 102
patients exhibiting EGFR E19 microdeletions and 63 patients
demonstrating E21 mutations, including 58 cases with L858R point
mutations. These numbers were consistent with previous studies
demonstrating that the two most common mutations were located in
E19 and E21 (3,10). Notably, one patient exhibited two
EGFR mutations simultaneously, E19 (E746-A750 DEL) and E21
(L858R). This patient was a female >60 years old who exhibited
adenocarcinoma with moderately-differentiated cells. Subgroup
analyses suggested that the incidence of EGFR mutations was
significantly affected by gender and age. In particular, mutations
were more likely to occur in female patients compared with male
patients and in older patients compared with younger patients. In
addition, it was observed that EGFR mutations were
identified more frequently in well-differentiated tumor cells,
which were typically less aggressive and grew more slowly compared
with less-differentiated cancer cells.
Mutations in KRAS are identified in a wide
range of types of cancer, including cancer of the pancreas, large
intestine and lungs (26). Although
15–25% of NSCLC patients have been observed to exhibit KRAS
mutations in previous studies, only 3.6% of patients in the present
study cohort possessed KRAS mutations, which was consistent
with the idea that the occurrence of this mutation may be
associated with smoking (27–29). In the present study, it was
additionally identified that KRAS mutations were more
frequently detected in male patients compared with female patients,
suggesting the effect of gender on the incidence of KRAS
mutations. The majority of the mutations have been identified in
E12 and less frequently in E13 (30),
and mutations in these exons are able to cause sustained activation
of RAS signaling leading to tumorigenesis (21,31).
However, despite a large sample size in the present study,
mutations were only identified in E12 at positions 12 and 13, and
not in E13, suggesting that the mutation rate in E13 may be low or
undetectable in NSCLC in never-smokers. It was additionally
identified that EGFR and KRAS mutations were mutually
exclusive, as has been reported previously (21). As patients exhibiting KRAS
mutations typically demonstrate a worse response to EGFR TKIs,
including gefitinib or erlotinib, compared to those with wild-type
KRAS (28), KRAS
mutations may be utilized as a negative predictive marker for
responses to EGFR TKI-based therapy (28).
Somatic point mutations in BRAF occur more
frequently in melanoma and thyroid, colon and ovarian cancer
(5). The V600E substitution, which
disrupts an inhibitory interaction between the P-loop and the
activation segment, and leads to constitutive kinase activation,
accounts for ~90% of BRAF missense mutations identified in
human tumors (32,33). Previous studies have reported that the
frequency of BRAF mutation in lung cancer is typically low,
normally below or around 1% (34,35).
Similarly, the present study detected a V600E point mutation in one
patient, accounting for 0.3% of NSCLC in never-smokers in the
present patient cohort.
The ALK gene encodes a receptor tyrosine
kinase, which has been identified in a number of fusion proteins in
cancer (6,36–39).
Adenocarcinoma appears to be the major NSCLC cell type to exhibit
EML4-ALK fusions. Previous studies, primarily involving East
Asian patients, have reported that 3–7% of lung tumors exhibit
EML4-ALK fusions (6,40–43). A
total of 27 cases (7.5%) in the present study demonstrated
EML4-ALK fusions. No other types of ALK fusions were
detected in the current patient cohort. The results of the present
study suggested that the onset age of lung cancer is likely to be
younger in patients possessing ALK fusions compared to those
without. Furthermore, the carcinoma cases were less differentiated
in patients exhibiting ALK fusions compared to those without
ALK fusions. These features may be at least in part
responsible for an observed poor response to EGFR TKIs associated
with ALK fusion (11), but an
improved response to ALK TKI crizotinib (12). In addition to ALK fusion,
KIF5B-RET fusion was detected in 1.4% of patients; however,
no CCDC6-RET fusions were observed in the present study.
Similar to EML4-ALK fusion, KIF5B-RET fusion is
likely to be associated with early disease onset, as it was
identified more frequently in younger patients. No other clinical
features were identified as being significantly associated with
RET mutations. However, this may have been due to the low
frequency of this genetic alteration, which may have required a
larger sample size to reach a statistically significant level.
In conclusion, the present study screened the
genetic mutations in multiple oncogenes and determined clinical
features associated with these mutations in a large cohort of NSCLC
patients who were exclusively never-smokers. It was identified that
EGFR mutations, but not other mutations, frequently occurred
in NSCLC in never-smokers. It was additionally identified that
gender may be associated with mutations in EGFR and
KRAS, differentiation level with EGFR and ALK,
and ageing with EGFR, ALK and RET. The results
of the present study may provide valuable insights for the
enhancement of our knowledge of lung cancer and facilitate the
advancement of tailored therapies that are targeted to tumorigenic
mutations.
Glossary
Abbreviations
Abbreviations:
|
EGFR
|
epidermal growth factor receptor
|
|
ALK
|
anaplastic lymphoma kinase
|
|
RET
|
ret proto-oncogene
|
|
EML4
|
echinoderm microtubule-associated
protein-like 4
|
|
KRAS
|
Kirsten rat sarcoma viral oncogene
homolog
|
|
BRAF
|
B-Raf proto-oncogene, serine/threonine
kinase
|
|
NSCLC
|
non-small cell lung cancer
|
|
TKI
|
tyrosine kinase inhibitor
|
|
RT-PCR
|
reverse transcription-polymerase chain
reaction
|
|
FFPE
|
formalin-fixed paraffin-embedded
|
References
|
1
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Schiller JH, Harrington D, Belani CP,
Langer C, Sandler A, Krook J, Zhu J and Johnson DH: Eastern
Cooperative Oncology Group: Comparison of four chemotherapy
regimens for advanced non-small-cell lung cancer. N Engl J Med.
346:92–98. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lynch TJ, Bell DW, Sordella R,
Gurubhagavatula S, Okimoto RA, Brannigan BW, Harris PL, Haserlat
SM, Supko JG, Haluska FG, et al: Activating mutations in the
epidermal growth factor receptor underlying responsiveness of
non-small-cell lung cancer to gefitinib. N Engl J Med.
350:2129–2139. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Santos E, Martin-Zanca D, Reddy EP,
Pierotti MA, Della Porta G and Barbacid M: Malignant activation of
a K-ras oncogene in lung carcinoma but not in normal tissue of the
same patient. Science. 223:661–664. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Davies H, Bignell GR, Cox C, Stephens P,
Edkins S, Clegg S, Teague J, Woffendin H, Garnett MJ, Bottomley W,
et al: Mutations of the BRAF gene in human cancer. Nature.
417:949–954. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Soda M, Choi YL, Enomoto M, Takada S,
Yamashita Y, Ishikawa S, Fujiwara S, Watanabe H, Kurashina K,
Hatanaka H, et al: Identification of the transforming EML4-ALK
fusion gene in non-small-cell lung cancer. Nature. 448:561–566.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Takeuchi K, Soda M, Togashi Y, Suzuki R,
Sakata S, Hatano S, Asaka R, Hamanaka W, Ninomiya H, Uehara H, et
al: RET, ROS1 and ALK fusions in lung cancer. Nat Med. 18:378–381.
2012. View
Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kohno T, Ichikawa H, Totoki Y, Yasuda K,
Hiramoto M, Nammo T, Sakamoto H, Tsuta K, Furuta K, Shimada Y, et
al: KIF5B-RET fusions in lung adenocarcinoma. Nat Med. 18:375–377.
2012. View
Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lipson D, Capelletti M, Yelensky R, Otto
G, Parker A, Jarosz M, Curran JA, Balasubramanian S, Bloom T,
Brennan KW, et al: Identification of new ALK and RET gene fusions
from colorectal and lung cancer biopsies. Nat Med. 18:382–384.
2012. View
Article : Google Scholar : PubMed/NCBI
|
|
10
|
Paez JG, Jänne PA, Lee JC, Tracy S,
Greulich H, Gabriel S, Herman P, Kaye FJ, Lindeman N, Boggon TJ, et
al: EGFR mutations in lung cancer: Correlation with clinical
response to gefitinib therapy. Science. 304:1497–1500. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Shaw AT, Yeap BY, Mino-Kenudson M,
Digumarthy SR, Costa DB, Heist RS, Solomon B, Stubbs H, Admane S,
McDermott U, et al: Clinical features and outcome of patients with
non-small-cell lung cancer who harbor EML4-ALK. J Clin Oncol.
27:4247–4253. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Thunnissen E, Bubendorf L, Dietel M,
Elmberger G, Kerr K, Lopez-Rios F, Moch H, Olszewski W, Pauwels P,
Penault-Llorca F and Rossi G: EML4-ALK testing in non-small cell
carcinomas of the lung: A review with recommendations. Virchows
Arch. 461:245–257. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Buettner R, Wolf J and Thomas RK: Lessons
learned from lung cancer genomics: The emerging concept of
individualized diagnostics and treatment. J Clin Oncol.
31:1858–1865. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Thun MJ, Hannan LM, Adams-Campbell LL,
Boffetta P, Buring JE, Feskanich D, Flanders WD, Jee SH, Katanoda
K, Kolonel LN, et al: Lung cancer occurrence in never-smokers: An
analysis of 13 cohorts and 22 cancer registry studies. PLoS Med.
5:e1852008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Pomerleau CS, Pomerleau OF, Snedecor SM
and Mehringer AM: Defining a never-smoker: Results from the
nonsmokers survey. Addict Behav. 29:1149–1154. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2013. CA Cancer J Clin. 63:11–30. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
U.S. Department of Health and Human
Services: The Health Consequences of Smoking-50 Years of Progress:
A Report of the Surgeon General. Office of the Surgeon General
(Rockville, MD). 139–351. 2014.
|
|
18
|
Gazdar AF and Thun MJ: Lung cancer, smoke
exposure, and sex. J Clin Oncol. 25:469–471. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Scagliotti GV, Longo M and Novello S:
Nonsmall cell lung cancer in never smokers. Curr Opin Oncol.
21:99–104. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kwak EL, Bang YJ, Camidge DR, Shaw AT,
Solomon B, Maki RG, Ou SH, Dezube BJ, Jänne PA, Costa DB, et al:
Anaplastic lymphoma kinase inhibition in non-small-cell lung
cancer. N Engl J Med. 363:1693–1703. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Karachaliou N, Mayo C, Costa C, Magrí I,
Gimenez-Capitan A, Molina-Vila MA and Rosell R: KRAS mutations in
lung cancer. Clin Lung Cancer. 14:205–214. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Choi YH, Lee JK, Kang HJ, Lee TS, Kim HR,
Kim CH, Koh JS, Baek HJ, Lee JC and Na II: Association between age
at diagnosis and the presence of EGFR mutations in female patients
with resected non-small cell lung cancer. J Thorac Oncol.
5:1949–1952. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ueno T, Toyooka S, Suda K, Soh J, Yatabe
Y, Miyoshi S, Matsuo K and Mitsudomi T: Impact of age on epidermal
growth factor receptor mutation in lung cancer. Lung Cancer.
78:207–211. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Mitsudomi T: Advances in target therapy
for lung cancer. Jpn J Clin Oncol. 40:101–106. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
An SJ, Chen ZH, Su J, Zhang XC, Zhong WZ,
Yang JJ, Zhou Q, Yang XN, Huang L, Guan JL, et al: Identification
of enriched driver gene alterations in subgroups of non-small cell
lung cancer patients based on histology and smoking status. PLoS
One. 7:e401092012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Bos JL: ras oncogenes in human cancer: A
review. Cancer Res. 49:4682–4689. 1989.PubMed/NCBI
|
|
27
|
Thu KL, Vucic EA, Chari R, Zhang W,
Lockwood WW, English JC, Fu R, Wang P, Feng Z, MacAulay CE, et al:
Lung adenocarcinoma of never smokers and smokers harbor
differential regions of genetic alteration and exhibit different
levels of genomic instability. PLoS One. 7:e330032012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Mao C, Qiu LX, Liao RY, Du FB, Ding H,
Yang WC, Li J and Chen Q: KRAS mutations and resistance to
EGFR-TKIs treatment in patients with non-small cell lung cancer: A
meta-analysis of 22 studies. Lung Cancer. 69:272–278. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Le Calvez F, Mukeria A, Hunt JD, Kelm O,
Hung RJ, Tanière P, Brennan P, Boffetta P, Zaridze DG and Hainaut
P: TP53 and KRAS mutation load and types in lung cancers in
relation to tobacco smoke: Distinct patterns in never, former, and
current smokers. Cancer Res. 65:5076–5083. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Brose MS, Volpe P, Feldman M, Kumar M,
Rishi I, Gerrero R, Einhorn E, Herlyn M, Minna J, Nicholson A, et
al: BRAF and RAS mutations in human lung cancer and melanoma.
Cancer Res. 62:6997–7000. 2002.PubMed/NCBI
|
|
31
|
Cataldo VD, Gibbons DL, Pérez-Soler R and
Quintás-Cardama A: Treatment of non-small-cell lung cancer with
erlotinib or gefitinib. N Engl J Med. 364:947–955. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Vakiani E and Solit DB: KRAS and BRAF:
Drug targets and predictive biomarkers. J Pathol. 223:219–229.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wan PT, Garnett MJ, Roe SM, Lee S,
Niculescu-Duvaz D, Good VM, Jones CM, Marshall CJ, Springer CJ,
Barford D and Marais R: Cancer Genome Project: Mechanism of
activation of the RAF-ERK signaling pathway by oncogenic mutations
of B-RAF. Cell. 116:855–867. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Rosell R, Bivona TG and Karachaliou N:
Genetics and biomarkers in personalisation of lung cancer
treatment. Lancet. 382:720–731. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Brustugun OT, Khattak AM, Trømborg AK,
Beigi M, Beiske K, Lund-Iversen M and Helland Å: BRAF-mutations in
non-small cell lung cancer. Lung Cancer. 84:36–38. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Morris SW, Kirstein MN, Valentine MB,
Dittmer KG, Shapiro DN, Saltman DL and Look AT: Fusion of a kinase
gene, ALK, to a nucleolar protein gene, NPM, in non-Hodgkin's
lymphoma. Science. 263:1281–1284. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Palmer RH, Vernersson E, Grabbe C and
Hallberg B: Anaplastic lymphoma kinase: Signalling in development
and disease. Biochem J. 420:345–361. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Coffin CM, Hornick JL and Fletcher CD:
Inflammatory myofibroblastic tumor: Comparison of
clinicopathologic, histologic, and immunohistochemical features
including ALK expression in atypical and aggressive cases. Am J
Surg Pathol. 31:509–520. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Chen Y, Takita J, Choi YL, Kato M, Ohira
M, Sanada M, Wang L, Soda M, Kikuchi A, Igarashi T, et al:
Oncogenic mutations of ALK kinase in neuroblastoma. Nature.
455:971–974. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Inamura K, Takeuchi K, Togashi Y, Nomura
K, Ninomiya H, Okui M, Satoh Y, Okumura S, Nakagawa K, Soda M, et
al: EML4-ALK fusion is linked to histological characteristics in a
subset of lung cancers. J Thorac Oncol. 3:13–17. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Takeuchi K, Choi YL, Soda M, Inamura K,
Togashi Y, Hatano S, Enomoto M, Takada S, Yamashita Y, Satoh Y, et
al: Multiplex reverse transcription-PCR screening for EML4-ALK
fusion transcripts. Clin Cancer Res. 14:6618–6624. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Shinmura K, Kageyama S, Tao H, Bunai T,
Suzuki M, Kamo T, Takamochi K, Suzuki K, Tanahashi M, Niwa H, et
al: EML4-ALK fusion transcripts, but no NPM-, TPM3-, CLTC-, ATIC-,
or TFG-ALK fusion transcripts, in non-small cell lung carcinomas.
Lung Cancer. 61:163–169. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Wong DW, Leung EL, So KK, Tam IY, Sihoe
AD, Cheng LC, Ho KK, Au JS, Chung LP and Wong Pik M: University of
Hong Kong Lung Cancer Study Group: The EML4-ALK fusion gene is
involved in various histologic types of lung cancers from
nonsmokers with wild-type EGFR and KRAS. Cancer. 115:1723–1733.
2009. View Article : Google Scholar : PubMed/NCBI
|