Introduction
Alveolar soft-part sarcoma (ASPS) is an infrequently
encountered type of soft-tissue sarcoma that usually develops in
the soft tissues of the extremities. The tumor accounts for <1%
of soft-tissue sarcomas and predominantly affects teenagers and
young adults (1). ASPS has a high
propensity for metastasis and the lungs are the most frequent site
of metastasis by the hematogenous route. Although prolonged
survival is possible even in patients with metastasis, the
long-term disease specific mortality rate is high. The prognosis of
ASPS is poor due to the high frequency of metastatic disease. A
large study indicated that the median survival time was 3 years if
metastatic disease was present at diagnosis and 11 years without
metastatic disease at presentation (1,2). ASPS is a
rare, aggressive malignancy of uncertain histological origin, with
a predisposition towards vascular invasion and distant metastasis.
ASPS is most commonly observed in the extremities (1), but most commonly in the lower rather
than the upper limbs. A previous study reported that ASPS is most
commonly identified in the lower extremities (44%) and is rarely
seen in the upper extremities (2).
Magnetic resonance imaging (MRI) is the favored
imaging modality for evaluation of this lesion due to its excellent
soft tissue contrast, multiplanar imaging capability and lack of
radiation exposure. Computed tomography (CT) enhancement and CT
angiography clearly showed rich blood vessels within and around the
tumor. The present study reports a case of ASPS of the right
deltoid muscle, with emphasis on the clinical and unique imaging
features that led to a correct diagnosis.
Case report
On April 22, 2014, a 30-year-old woman presented to
Subei People's Hospital (Yangzhou, Jiangsu, China) with a mass on
the right shoulder that had been apparent for 3 years, but that had
rapidly grown in the last month. Physical examination revealed a
well demarcated, soft, non-tender mass on the right shoulder.
Sensory and motor examinations of the right upper limb were
normal.
MRI and CT scanning of the right shoulder were
performed using the 3.0-Tesla MRI scanner (Signa HDxt; GE Medical
Systems, Milwaukee, WI, USA) and CT scanner (Discovery CT750 HD; GE
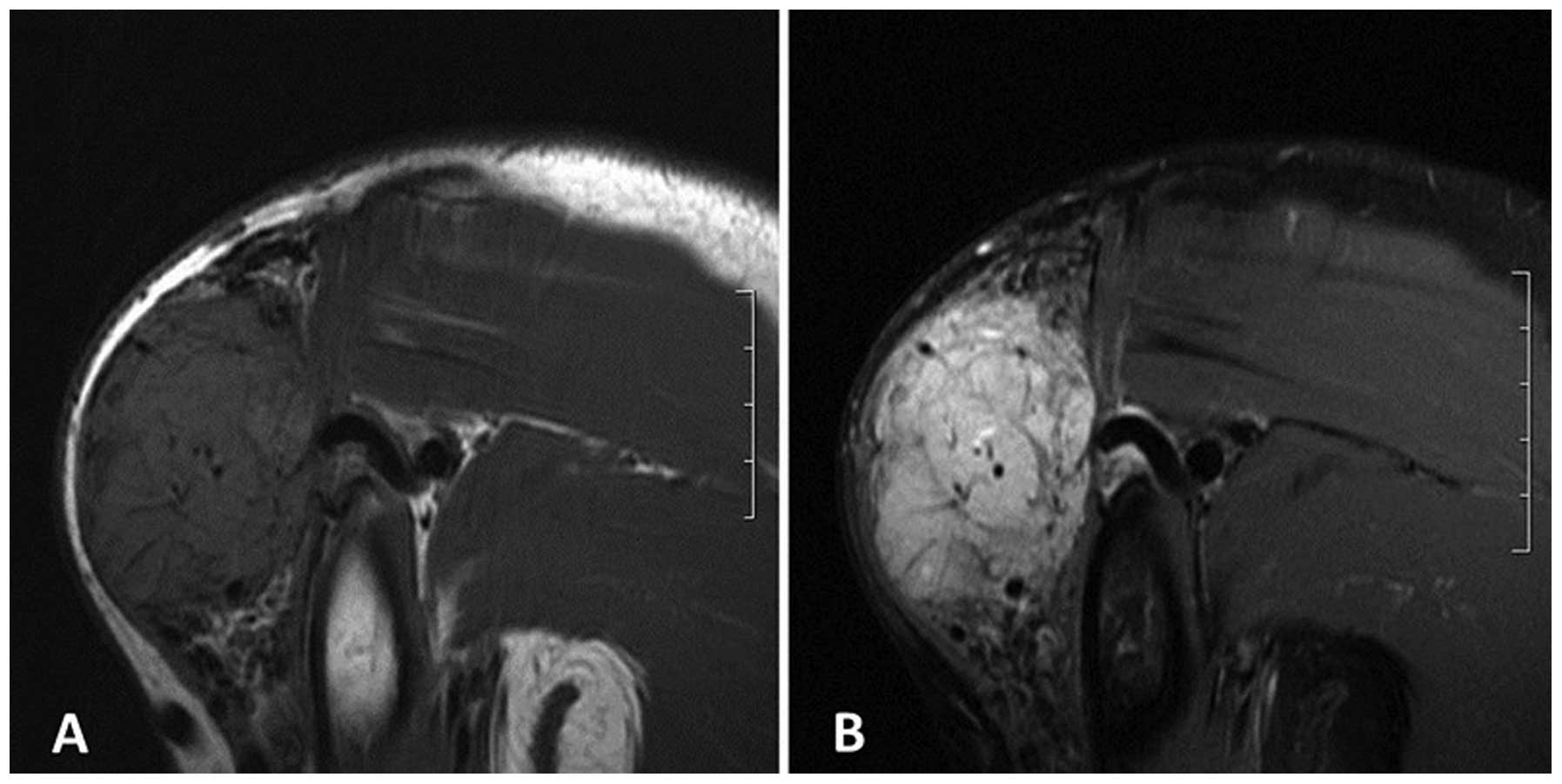
Medical Systems). MRI revealed a hyperintense ovoid mass on the
T2-weighted fat suppression image, and an isointense and
hyperintense mass on the T1-weighted image (T1WI) compared with
surrounding structures, with circuitous flow empty signals within
and around the tumor (Fig. 1A and B).
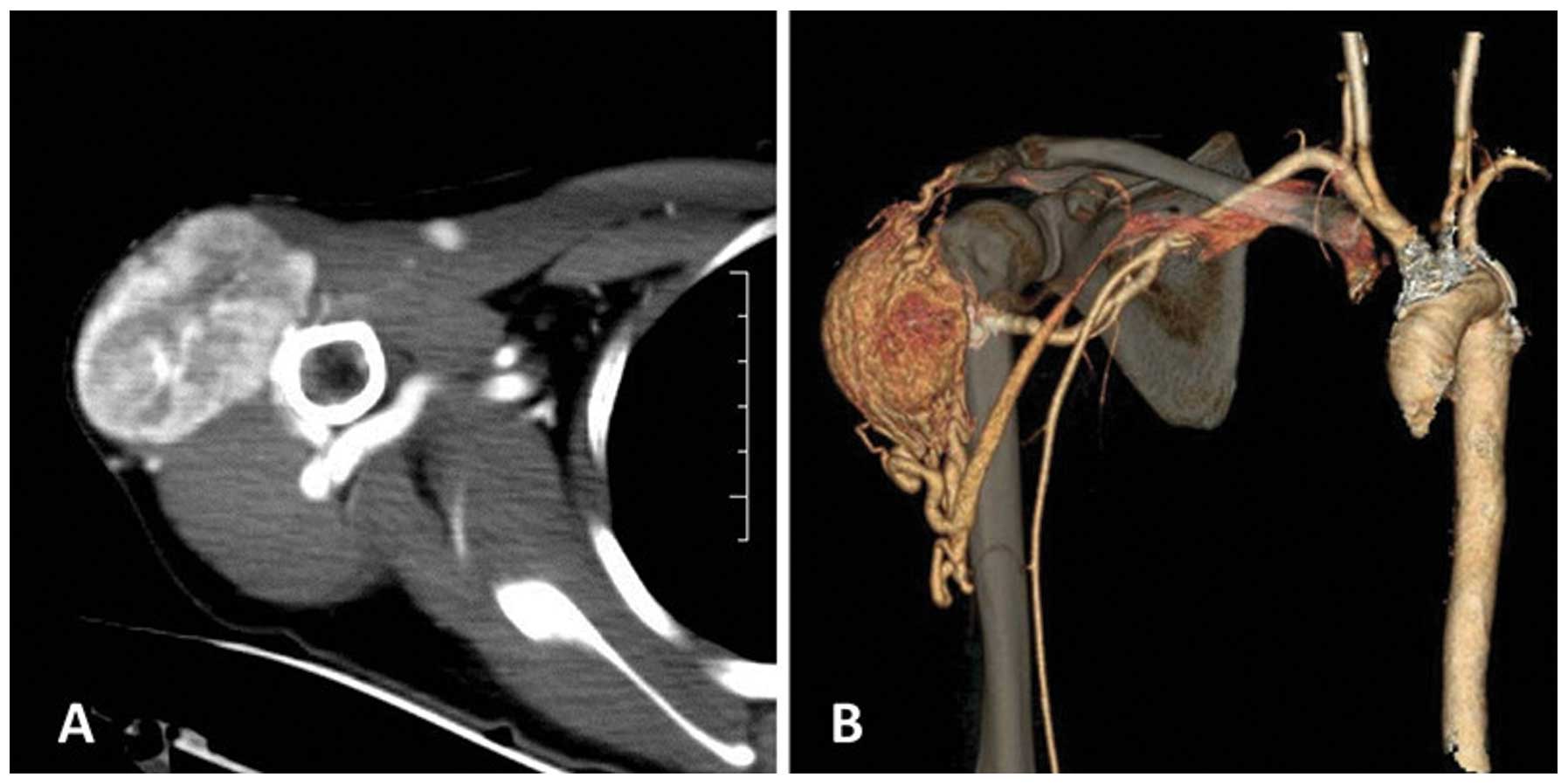
CT enhancement showed a homogeneous enhanced mass (Fig. 2A). CT angiography clearly showed rich
blood vessels within and around a large hypervascular mass that was
predominately supplied from the right subclavian artery, with
venous drainage backflow into the subclavian vein (Fig. 2B). The bone structure of the right
shoulder did not show any abnormalities. A surgical excision of the
tumor was performed. During the procedure, the tumor mass was
observed to be soft, hypervascular and well separated from the
surrounding tissue. Tumor specimens were sent to the Department of
Pathology, Subei People's Hospital, for histological and
immunohistochemical analysis. The specimen was fixed using 10%
formaldehyde, paraffin-embedded, stained with hematoxylin and
eosin, dyed with periodic acid schiff and immunohistochemically
stained for the detection of CD34. All antibodies and reagents are
from Fuzhou Maixin Biotechnology Co., Ltd. (Fuzhou, China). A
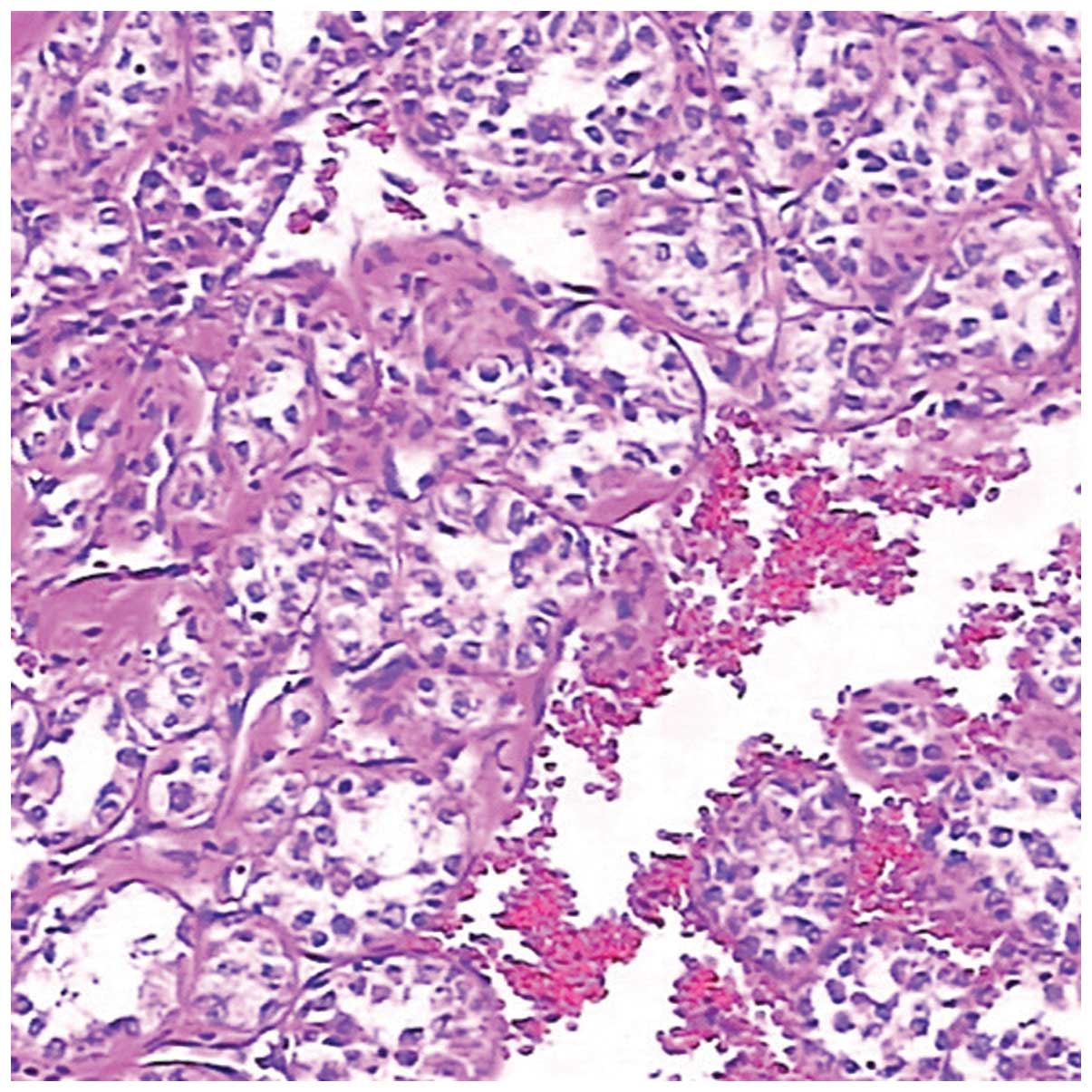
histological examination of the surgical specimens revealed nests
of large granular cells separated by fibrovascular stroma. The
cells were large and round to polygonal in shape, growing in the
classical alveolar pattern (Fig. 3).
Immunohistochemical findings showed that the cells were
periodic-acid Schiff-positive. A final diagnosis of ASPS was
made.
At present, the patient remains alive. An MRI scan
of the right shoulder showed no evidence of local tumor recurrence
at 3, 9 and 12 months following the wide surgical excision. A CT
scan showed no metastatic nodules in either lung during the
follow-up. The patient prognosis is good.
Discussion
ASPS is an extremely rare malignant tumor that
constitutes <1% of all soft-tissue sarcomas. The tumor exhibits
a slight female preponderance in patients ≤30 years old, in
contrast to a male preponderance in patients >30 years old. The
average age of onset falls within the second decade of life
(2,3).
In adults, ASPS is most commonly found in the lower
extremities, followed by the trunk and upper extremities, whereas
in infants and children, the majority of cases occur in the head
and neck (3). The present study of a
case in the upper extremity is relatively rare. The clinical course
of the disease is slow, but with a high frequency of metastases,
usually to the lungs, brain and bones. In the present study, the
tumor occurred in a 30-year-old patient and the primary tumors were
located in the extremity, representing a relatively indolent mass.
These features are consistent with the previously reported
literature, with the exception of a lack of metastasis.
ASPS derives its name from its histological
appearance. Histologically, ASPS is characterized by a nest-like
pattern of large, round to polygonal tumor cells with eosinophilic
cytoplasm, exhibiting the classical alveolar growth pattern
(4). These cells are PAS-positive
with diastase-resistant intracytoplasmic inclusions.
Immunohistochemical staining for CKpan, epithelial membrane
antigen, MyoD1, myoglobin, myogenin, smooth muscle actin, desmin,
CD34, CD10, Syn, chromogranin A and S-100 were negative (5). The present case was consistent with
these histological features.
Regarding the imaging features, it has been noted
that ASPSs mainly present as large and well-defined masses, with
equal or slight hyperintensity on T1WI and hyperintensity on T2WI
compared with the surrounding structures, and frequently occurring
vascular signal voids (6). These
features of a high signal intensity on T1WI and the presence of
vascular signal voids within and around the tumor may represent the
typical MRI features of ASPS (6). The
precise cause of this high signal intensity on T1WI has not yet
been elucidated. It has been hypothesized that this may be
attributed to slow-flowing blood in or around the tumor and blood
sinuses (cavities and separation between the blood vessels) in the
tumor tissues. Vascular signal voids may be associated with rapid
blood flow wash-out (7,8). Non-contrast CT scans show the tumor to
be of slightly high density and can display the location, scope,
form and interior calcification of the tumor. However, they do not
show the components in the tumor as well as MRI. Contrast-enhanced
CT and MRI show intense, heterogeneous enhancement (9). Multi-slice spiral CT angiography can
clearly display a hypervascular mass with multiple, enlarged
tortuous vessels, and arteries and veins supplying blood to the
tumor, which provides guidance for surgery (9). In the present case, the tumor exhibited
a high signal intensity on T1WI and T2WI compared with the
surrounding structures. The tumor was well enhanced on
contrast-enhanced CT and MRI, and exhibited vascular signal voids.
These reliable radiologic findings are well correlated with the
high vascularity of ASPS in pathological specimens (10).
Several imaging features can assist in
distinguishing ASPS from other benign or malignant tumors, such as
hemangiomas and vessel malformations, synovial sarcoma and
malignant fibrous histiocytoma (MFH) (10,11). In
ASPSs, vascular tissues surround the solid tumor tissues and blood
flow wash-out is slow. This is in contrast to a high-flow vascular
malformation, such as an arteriovenous malformation, with pure
vascular tissue but no accompanying tissues, which enables the
differentiation between the two conditions (12). The majority of sarcomas generally grow
quickly, are relatively large and are located deep within the
tissues, therefore, differentiating between them is occasionally
difficult. However, certain imaging findings can assist in the
diagnosis. Cases of synovial sarcoma typically occur in adults in
and around the knee joint and lower leg, and tumor growth is slow
and superficial, without flow voids or signal voids on MRI, but
with calcification, necrosis and hemorrhage often noted on CT.
Malignant fibrous histiocytoma is often observed in older men, and
MRI showing necrosis, cystic regions and edema of the tumor is
common while the blood vessels and nerves around the tumor are
easily damaged. However, these features generally cannot be
observed in ASPS, so recognition of these characteristic CT and MRI
findings may lead to the early diagnosis of ASPS and avoid a
misdiagnosis, which is important in the treatment of a small
primary tumor (12).
According to the present study, when a slow-growing,
painless superficial mass is encountered in the limbs, particularly
the upper limbs, of young adult patients, the possibility of a
sarcoma must be considered after a careful examination that
eliminates all the benign possibilities, such as a ganglion or
lipoma. The CT and MRI features of ASPS assist in providing a
correct diagnosis and will aid surgeons in performing a wide
surgical resection to reduce the risk of local recurrence.
Angiography also adds useful diagnostic information. The ability to
understand the imaging and clinical features of ASPS has certain
value for the pre-operative qualitative diagnosis and clinical
treatment of the tumor.
Glossary
Abbreviations
Abbreviations:
|
ASPS
|
alveolar soft-part sarcoma
|
|
MRI
|
magnetic resonance imaging
|
|
T1WI
|
T1-weighted imaging
|
|
T2WI
|
T2-weighted imaging
|
References
|
1
|
Van Vliet M, Kliffen M, Krestin GP and van
Dijke CF: Soft tissue sarcomas at a glance: Clinical, histological,
and MR imaging features of malignant extremity soft tissue tumors.
Eur Radiol. 19:1499–1511. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Folpe AL and Deyrup AT: Alveolar soft-part
sarcoma: A review and update. J Clin Pathol. 59:1127–1132. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Suh JS, Cho J, Lee SH, Shin KH, Yang WI,
Lee JH, Cho JH, Suh KJ, Lee YJ and Ryu KN: Alveolar soft part
sarcoma: MR and angiographic findings. Skeletal Radiol. 29:680–689.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ladanyi M, Lui MY, Antonescu CR,
Krause-Boehm A, Meindl A, Argani P, Healey JH, Ueda T, Yoshikawa H,
Meloni-Ehrig A, et al: The der (17)t(X;17)(p11;q25) of human
alveolar soft part sarcoma fuses the TFE3 transcription factor gene
to ASPL, a novel gene at 17q25. Oncogene. 20:48–57. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Argani P, Lal P, Hutchinson B, Lui MY,
Reuter VE and Ladanyi M: Aberrant nuclear immunoreactivity for TFE3
in neoplasms with TFE3 gene fusions: A sensitive and specific
immunohistochemical assay. Am J Surg Pathol. 27:750–761. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Vilanova JC, Woertler K, Narváez JA,
Barceló J, Martínez SJ, Villalón M and Miró J: Soft-tissue tumors
update: MR imaging features according to the WHO classification.
Eur Radiol. 17:125–138. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lai YC, Chiou HJ, Wu HT, Chou YH, Wang HK
and Chen PC: Ultrasonographic and MR findings of alveolar soft part
sarcoma. J Chin Med Assoc. 72:336–339. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Iwamoto Y, Morimoto N, Chuman H, Shinohara
N and Sugioka Y: The role of MR imaging in the diagnosis of
alveolar soft part sarcoma: A report of 10 cases. Skeletal Radiol.
24:267–270. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kim HS, Lee HK, Weon YC and Kim HJ:
Alveolar soft-part sarcoma of the head and neck: Clinical and
imaging features in five cases. AJNR Am J Neuroradiol.
26:1331–1335. 2005.PubMed/NCBI
|
|
10
|
Ogura K, Beppu Y, Chuman H, Yoshida A,
Yamamoto N, Sumi M, Kawano H and Kawai A: Alveolar soft part
sarcoma: A single-center 26-patient case series and review of the
literature. Sarcoma. 2012:9071792012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Dobson MJ, Hartley RW, Ashieigh R, Watson
Y and Hawnaur JM: MR angiography and MR imaging of symptomatic
vascular malformations. Clin Radiol. 52:595–602. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Pang LM, Roebuck DJ, Griffith JF, Kumta SM
and Metreweli C: Alveolar soft-part sarcoma: A rare soft-tissue
malignancy with distinctive clinical and radiological features.
Pediatr Radiol. 31:196–199. 2001. View Article : Google Scholar : PubMed/NCBI
|