Introduction
Hepatocellular carcinoma (HCC) is reportedly the
fifth most common type of cancer and third most common cause of
tumor-related mortality worldwide, with an annual incidence of
500,000–1,000,000 (1). Radiofrequency
ablation (RFA) is now widely used to treat HCC and hepatic
metastasis, as it is minimally invasive, effective and relatively
safe. Several clinical studies have demonstrated that RFA may
achieve an overall survival rate similar to that of surgical
resection in patients with small HCC (2,3); however,
due to the growing number of patients undergoing the procedure and
the increasing number of lesions manifesting in precarious
locations, such as the subcapsular region, hepatic dome, peri-hilum
area, and areas close to the bile duct and intestinal tract, a
number of post-RFA complications have been reported (3–7). Common
complications include subcapsular hematoma, hepatic abscess,
biloma, pneumothorax and pleural effusion. Rare complications, such
as diaphragmatic necrosis and abscesso-colonic and biliopleural
fistula have also been reported (1,8).
The present study reports a case of delayed
bronchobiliary fistula (BBF), caused by the rupture of a biloma as
a rare complication of RFA in a patient with HCC. The biloma and
BBF were resolved by percutaneous biloma drainage and an extensive
surgical intervention, including hepatolobectomy,
choledocholithotomy and T-tube drainage. Written informed consent
was obtained from the patient for publication of the present study
and accompanying images.
Case report
A 57-year-old male patient with chronic hepatitis B
(HB), who was suspected to have HCC located in segment VIII
following detection of a lesion by Doppler Ultrasound (GE Voluson
730 Expert; GE Healthcare Bio-Sciences, Pittsburgh, PA, USA) during
a routine examination, was admitted to The Third Affiliated
Hospital of Sun Yat-sen University (Guangzhou, China) on 21
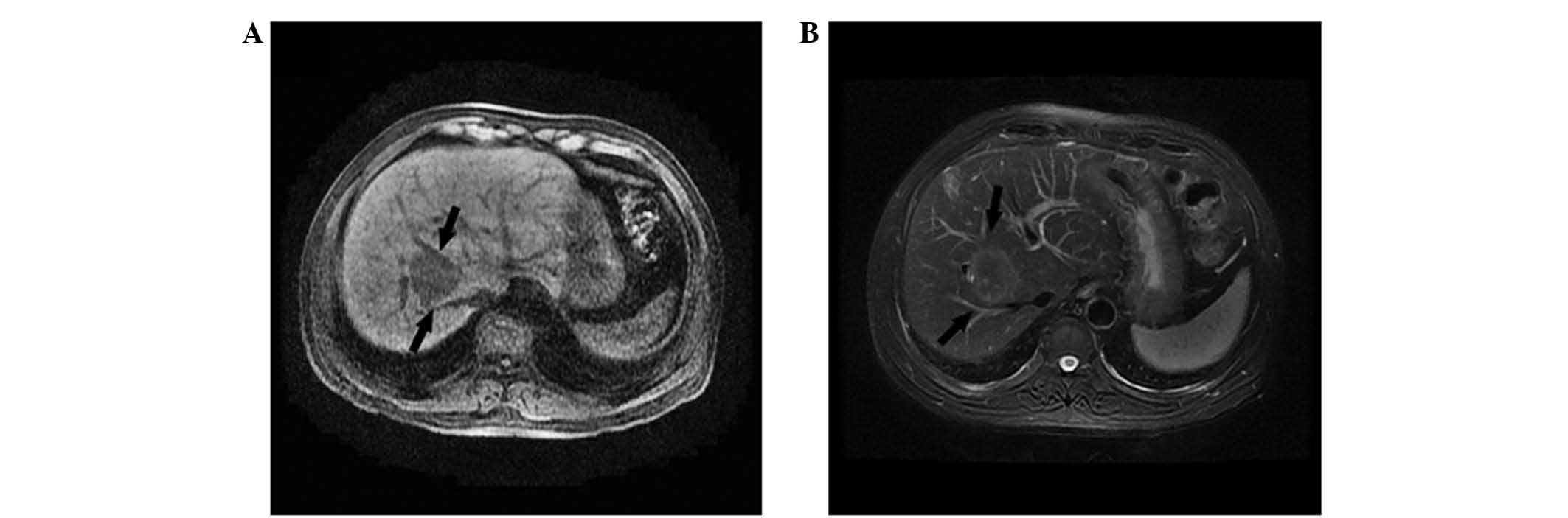
September, 2010. An MRI scan (Signa Excite 1.5T TwinSpeed; GE
Healthcare Bio-Sciences) revealed a tumor in segment VIII, which
measured 44×34 mm and was in close proximity to the right and
middle hepatic veins and right anterior portal vein branch
(Fig. 1). The laboratory examinations
revealed an α-fetoprotein level of 10.27 ng/ml (normal range, ≤20
ng/ml) and HB virus-DNA quantification results of
7.56×103 IU/ml (normal range, <100 IU/ml).
Hematological and biochemical test results for complete blood cell
count, prothrombin time, aspartate aminotransferase (AST), alanine
aminotransferase (ALT), total bilirubin (TBIL), serum albumin and
creatinine, were all normal. AST was measured as 18/U/l (normal
range, 15–40 U/l), ALT as 20 U/l (normal range, 3–35 U/l) and TBIL
as 12.4 µmol/l (normal range, 4–23.9 µmol/l). The patient also had
a history of type 2 diabetes mellitus, chronic coronary heart
disease and cerebral infarction; therefore, surgical resection was
not considered.
A combined therapy of transcatheter arterial
chemoembolization (TACE) and percutaneous RFA was adopted. TACE was
performed by superselective catheterization of the tumor-feeding
artery. An emulsion of 6 ml lipiodol (Guerbet, Aulnay-sous-Bois,
France) and 30 mg doxorubicin hydrochloride (Pfizer, Inc., Wuxi,
China) was infused into the artery, which was followed by an
embolization of gelatin sponge particles (Hangzhou AILIKANG
Medicine Technology Co. Ltd., Hangzhou, China). At 11 days after
TACE, the RFA procedure was performed with ultrasonography guidance
under general anesthesia using a 10-cm long cool-tip electrode with
a 2-cm active tip and a 200-W RF generator (Radionics, Inc.,
Burlington, MA, USA). A total of 8 overlapping ablations, each
lasting 12 min, were performed.
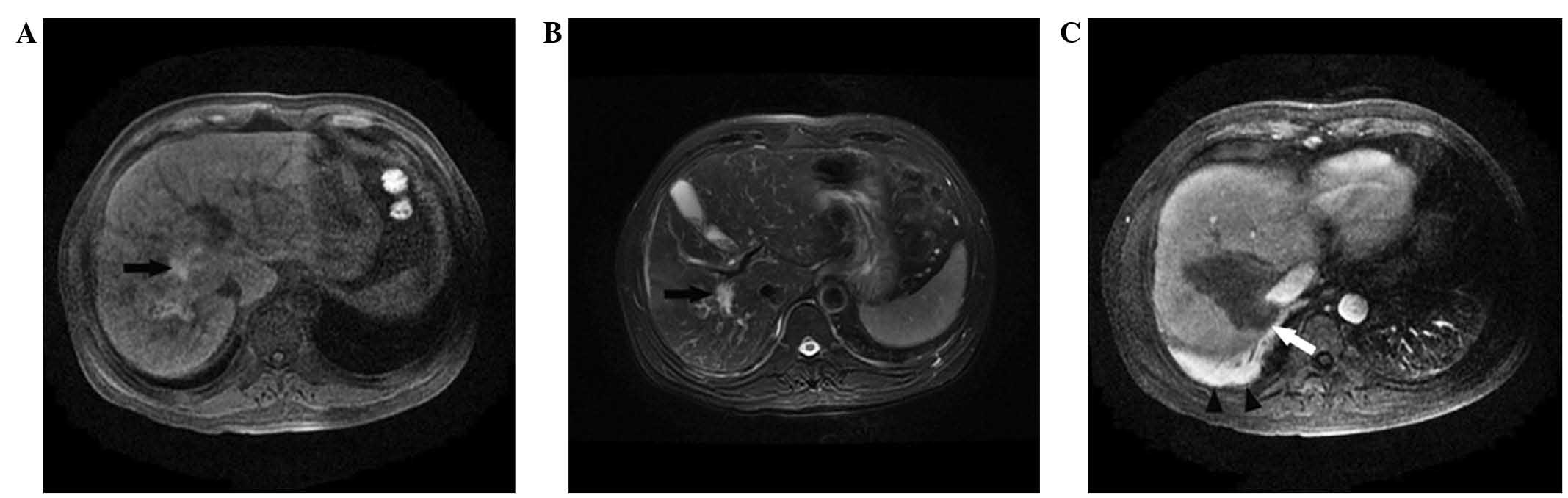
Abdominal MRI performed 1 month after RFA revealed
an ablation zone of 75×54 mm reaching the right diaphragm, and a
small amount of right pleural effusion (Fig. 2). At 17 months after RFA, the patient
was re-admitted to the hospital after presenting with fever and an
irritating cough lasting for 1 week. The laboratory findings were
as follows: AST, 64 U/l; ALT, 20 U/l; TBIL, 57.8 µmol/l. The
light-yellow sputum was confirmed by laboratory biochemical testing
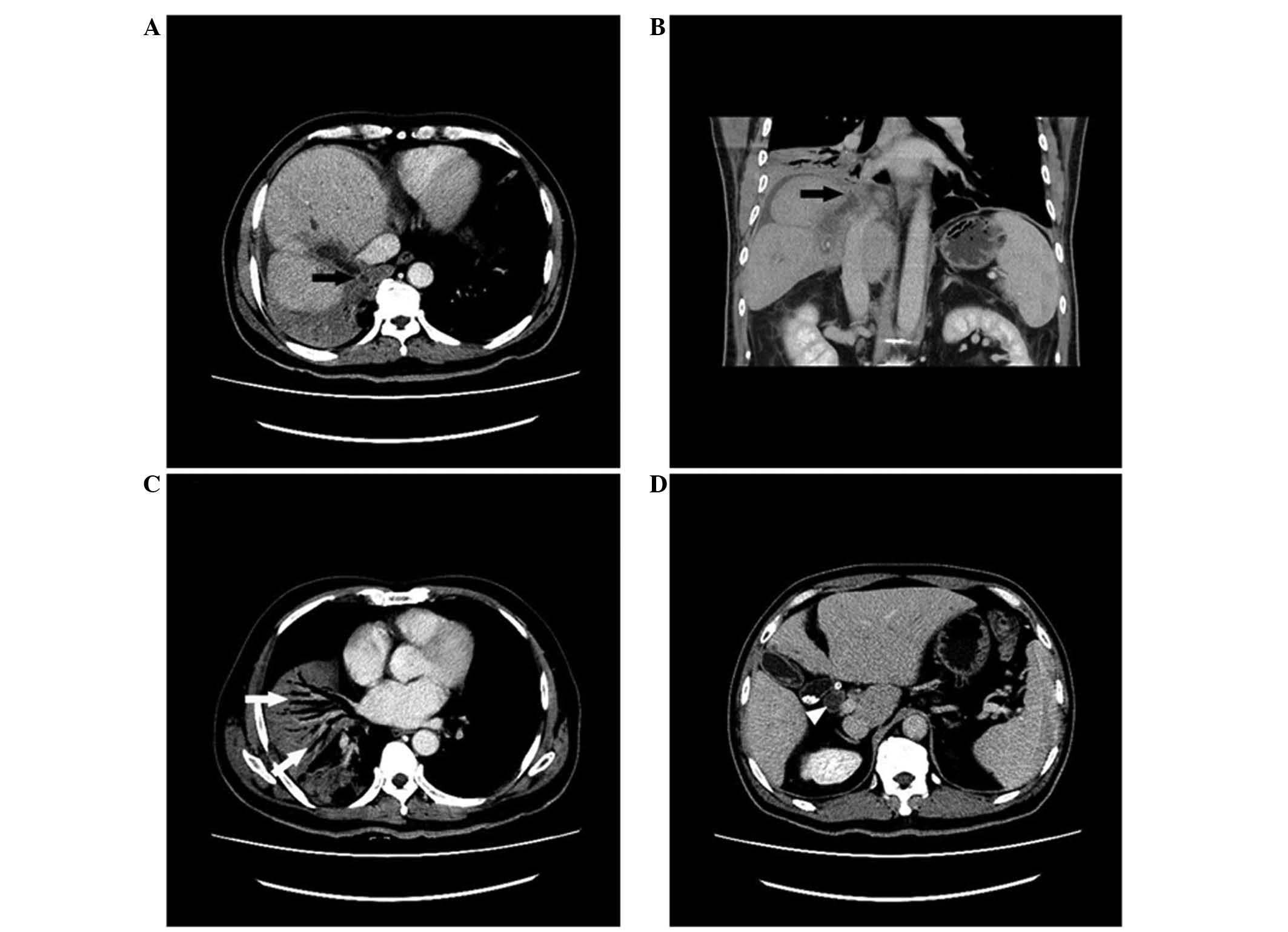
to have bile components. Computed tomography (CT) scans (AQUILION
ONE™; Toshiba Medical Systems, Otawara, Japan) of the chest and
abdomen revealed a biloma at the ablation zone, which ruptured into
the thoracic and abdominal cavities. In addition, pneumonia and
atelectasis were observed in the right lower lung lobe, and a small
right pleural effusion, as well as biliary sludge and small biliary
calculi, were detected in the dilated bile duct (Fig. 3).
Ultrasonography-guided percutaneous transhepatic
biloma drainage was performed using an 8-French pigtail catheter.
The fluid that was aspirated from the biloma during the procedure
contained yellow bile and brown biliary sludge, in which
Escherichia coli was identified following bacterial culture.
BBF was further suggested by an injection of 2 ml methylene blue
solution into the biloma through the drainage catheter, following
which the methylene blue solution was expectorated from the mouth.
X-ray angiography performed through the drainage catheter showed
that the biloma communicated with the biliary system, with multiple
small biliary calculi found in the dilated bile ducts.
One month after the biloma drainage, the cough had
subsided but the fever persisted. Chest and abdominal CT scans
demonstrated the improvement of pneumonia and right pleural
effusion; however, the biliary sludge and small biliary calculi
endured in the dilated bile duct. Despite repeated drainage and
treatment with antibiotics for 1 month, the fever did not resolve.
The cause of the fever was considered to be a biliary system
infection that had not been controlled by the percutaneous biloma
drainage, and an extensive surgical intervention including
hepatolobectomy, choledocholithotomy and T-tube drainage was
performed. Intraoperatively, an active leak was detected at the
start of the right hepatic ducts, which allowed for communication
between the biloma and the biliary system. In addition, a large
volume of dark brown biliary sludge and calculi, which had led to
biliary obstruction, dilatation and infection were detected. The
biloma and BBF were successfully treated and the patient was
discharged 40 days after the surgery. On 10 March, 2014, tumor
recurrence was detected in segment II by MRI. RFA was successfully
performed on March 14, 2014; A total of 2 overlapping ablations,
each lasting 12 min, were performed. To date, no further tumor
recurrence has been detected during follow-up examinations, in
addition to no recurrence of biloma or BBF.
Discussion
BBF is a rare disease that was first reported by
Peacock in 1850 (9). BBF is an
abnormal communication between the bile duct and the bronchial
tree, and can arise from hydatid disease, trauma, bile duct
obstruction, tumor invasion and iatrogenic injuries caused by
procedures such as TACE and RFA (10,11). The
complication rate of RFA for HCC is 0.6–10% (4,12);
however, only sporadic cases of BBF as a complication of RFA have
been reported (13–15). To the best of our knowledge, this is
the first reported case of delayed BBF caused by biloma rupture
following RFA.
The most specific symptom of BBF is expectoration of
yellow, bile-tinged sputum (13).
Biochemical examination of the sputum may identify BBF based on the
presence of bile components. CT scan is used as the first-line
imaging technique. Despite the fact that it may not directly
display the fistula tract, it can reveal indirect findings, such as
pneumonia, subphrenic fluid collection, pleural effusion, liver
abscess, biloma and bile duct calculi (8,11,14). Contrast-enhanced magnetic resonance
cholangiopancreatography is a non-invasive technique that may be
used to diagnose BBF and can directly detect the fistula tract
(16). Invasive examinations, such as
percutaneous transhepatic cholangiography or endoscopic retrograde
cholangiopancreatography, can reveal the abnormal fistula tract
between the biliary system and the bronchial tree, which is
considered to be the most direct evidence to suggest BBF (8,12). In the
present case, the patient's sputum was confirmed to contain bile
components by biochemical examination, and methylene blue solution
was injected into the biloma through the drainage catheter and was
later expectorated from the mouth. Both examinations are able to
confirm the diagnosis of BBF.
In the present case, the delayed BBF following RFA
was most likely a joint result of various factors, such as the
formation of the biloma, the damage to the diaphragm abutting the
biloma, biliary infection and bile duct obstruction.
The damage to the diaphragm and the formation of a
biloma may be predominantly attributed to the thermal effects of
RFA on the diaphragm and bile duct. A large tumor, close to the
hilum or hepatic dome, has been found to be a predisposing factor
of BBF following RFA (8,11). In the present case, a liver tumor
measuring 44×34 mm, which was located near the right hepatic bile
duct and dome, was treated with RFA, and the ablation zone was
found to have reached a size of 75×54 mm on MRI at 1 month after
RFA. The ablation zone margin was found to reach the diaphragm and
a small amount of right pleural effusion was observed on the MRI
scan (Fig. 2), suggesting the
possibility of diaphragmatic injury. Although no active biliary
fistula leak was directly detected by MRI scan at 1 month after
RFA, bile leakage was observed (Fig.
2). The hepatectomy performed later also confirmed that the
biliary fistula originated from the right hepatic bile duct, which
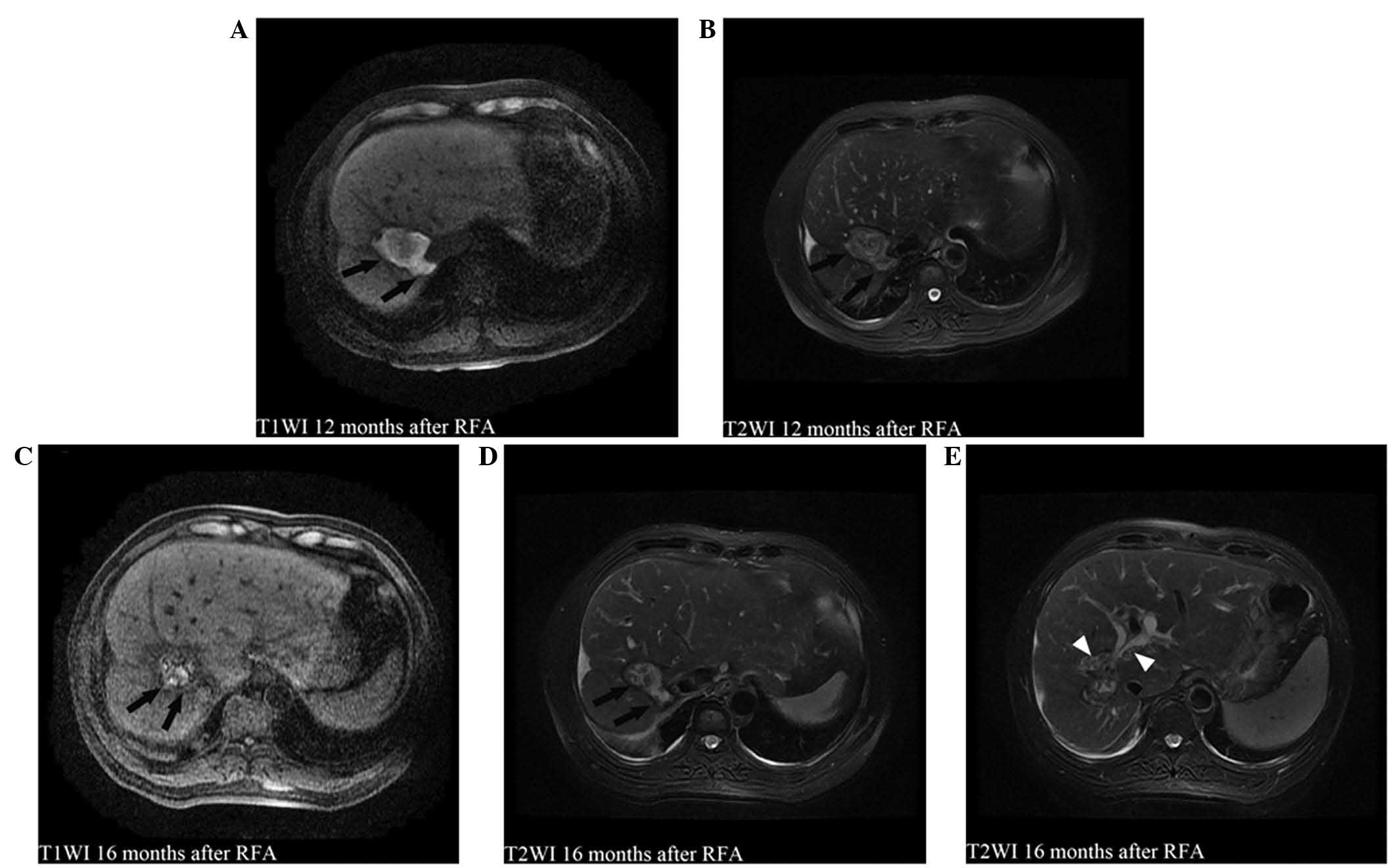
directly communicated with the biloma. In addition, the bile duct
obstruction, which had been caused by a large volume of biliary
sludge and stones, could have contributed to the rising pressure of
the biloma and its later rupture, as the increase in bile leakage,
biliary sludge and stones and bile duct dilation (Fig. 4) were detected on the follow-up MRI
scan prior to the rupture of the biloma. The existence of a biloma
might have also caused the repeated biliary infection, which was
responsible for the fever that persisted even after percutaneous
biloma drainage was performed; therefore, in the present case,
various pathological conditions could have simultaneously
contributed to the formation of a delayed BBF.
The primary treatment for BBF is relief of the bile
duct obstruction and drainage of the subphrenic or hepatic
abscesses and biloma. Less invasive treatment procedures include
endoscopic or percutaneous biliary drainage or percutaneous biloma
drainage (8,13). Most BBFs can be resolved by drainage
and biliary tract decompression; however, certain BBFs persist,
requiring surgical intervention (9).
The surgical approach often adopted by clinicians involves
thoracicoabdominal exploration, including hepatolobectomy,
resection of the fistula tract, pulmonary lobectomy and
cholangioenterostomy, alone or as a combination of various surgical
approaches. In the present case, after the patient underwent
percutaneous biloma drainage, the pneumonia and subphrenic and
pleural effusions were nearly resolved; however, the persistent
fever was not resolved, which could have been due to insufficient
drainage of the biloma by percutaneous drainage alone. Bile duct
obstruction, which was caused by a large volume of biliary sludge
and stones, contributed to the insufficient drainage, which, in
turn, caused repeated biliary infection and persistent fever. An
extensive surgical intervention was required in order to resect the
biloma and remove the biliary sludge and stones.
Had the biloma and its enlargement been identified
early on, during the follow-up MRI scan, and the percutaneous
biloma drainage been performed in a timely manner, the development
of BBF and subsequent surgical intervention could have been
prevented. In fact, the biloma was present 1–16 months after RFA,
before the patient presented with fever and coughing up of
bile-tinged sputum. The biloma was retrospectively observed on a
review of the MRI scan performed 1 month after RFA (Fig. 2). In addition, on the follow-up MRI
scans at 3, 6, 12 and 16 months after RFA, biloma enlargement, bile
duct obstruction, caused by a large volume of biliary sludge and
stones, and bile duct dilation were detected (Fig. 4). The bile duct obstruction led to an
increase in the bile leakage and pressure of the biloma, prior to
the rupture of the biloma. These results were supported by the
hepatolobectomy that was later performed. The findings of the
present study suggested that, when biloma enlargement is observed
on follow-up MRI scans, timely percutaneous biloma drainage should
be performed to prevent its rupture and the development of BBF.
In conclusion, for patients with large tumors close
to the hepatic dome and hilum, RFA should be cautiously performed,
in order to prevent thermal injury to the diaphragm and bile duct.
In addition, regular follow-up MRI scans after RFA are required for
the early detection of biloma, and percutaneous biloma drainage
should be performed as soon as an enlarging biloma is detected by
MRI scan, for the prevention of biloma rupture and BBF
development.
Acknowledgments
This study was supported by the National Natural
Science Foundation of China (grant no. 81371655) and the Science
and Technology Planning Project of Guangdong Province, China (grant
no. 2010B031600211).
References
|
1
|
Kim JY, Kwon YH, Lee SJ, Jang SY, Yang HM,
Jeon SW and Kweon YO: Abscesso-colonic fistula following
radiofrequency ablation therapy for hepatocellular carcinoma: A
case successfully treated with histoacryl embolization. Korean J
Gastroenterol. 58:270–274. 2011.(In Korean). View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Peng ZW, Lin XJ, Zhang YJ, Liang HH, Guo
RP, Shi M and Chen MS: Radiofrequency ablation versus hepatic
resection for the treatment of hepatocellular carcinoma 2 cm or
smaller: A retrospective comparative study. Radiology.
262:1022–1033. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Solbiati L, Ahmed M, Cova L, Ierace T,
Brioschi M and Goldberg SN: Small liver colorectal metastases
treated with percutaneous radiofrequency ablation: Local response
rate and long-term survival with up to 10-year follow-up.
Radiology. 265:958–968. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Minami Y and Kudo M: Radiofrequency
ablation of hepatocellular carcinoma: Current status. World J
Radiol. 2:417–424. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Teratani T, Yoshida H, Shiina S, Obi S,
Sato S, Tateishi R, Mine N, Kondo Y, Kawabe T and Omata M:
Radiofrequency ablation for hepatocellular carcinoma in so-called
high-risk locations. Hepatology. 43:1101–1108. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Chang IS, Rhim H, Kim SH, Kim YS, Choi D,
Park Y and Lim HK: Biloma formation after radiofrequency ablation
of hepatocellular carcinoma: Incidence, imaging feature, and
clinical significance. AJR Am J Roentgenol. 195:1131–1136. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Livraghi T, Solbiati L, Meloni MF, Gazelle
GS, Halpern EF and Goldberg SN: Treatment of focal liver tumors
with percutaneous radiofrequency ablation: Complications
encountered in a multicenter study. Radiology. 226:441–451. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Pende V, Marchese M, Mutignani M, Polinari
U, Allegri C, Greco R and Costamagna G: Endoscopic management of
biliopleural fistula and biloma after percutaneous radiofrequency
ablation of liver metastasis. Gastrointest Endosc. 66:616–618.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Peacock TB: Case in which hydatids were
expectorated and one of suppuration of hydatid cyst of the liver
communicating with the lungs. Edinburgh Med Surg J. 74:33–46.
1850.
|
|
10
|
Liao GQ, Wang H, Zhu GY, Zhu KB, Lv FX and
Tai S: Management of acquired bronchobliary fistula: A systematic
literature review of 68 cases published in 30 years. World J
Gastroentrol. 17:3842–3849. 2011. View Article : Google Scholar
|
|
11
|
Yoon DH, Shim JH, Lee WJ, Kim PN, Shin JH
and Kim KM: Percutaneous management of a bronchobiliary fistula
after radiofrequency ablation in a patient with hepatocellular
carcinoma. Korean J Radiol. 10:411–415. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kong WT, Zhang WW, Qiu YD, Zhou T, Qiu JL,
Zhang W and Ding YT: Major complications after radiofrequency
ablation for liver tumors: Analysis of 255 patients. World J
Gastroenterol. 15:2651–2656. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kim YS, Rhim H, Sung JH, Kim SK, Kim Y,
Koh BH, Cho OK and Kwon SJ: Bronchobiliary fistula after
radiofrequency thermal ablation of hepatic tumor. J Vasc Interv
Radiol. 16:407–410. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Tran T, Hampel H, Qureshi WA and Shaib Y:
Successful endoscopic management of bronchobiliary fistula due to
radiofrequency ablation. Dig Dis Sci. 52:3178–3180. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kim DH, Choi DW, Choi SH, Heo JS, Jeong J
and Rhu J: Surgical treatment of bronchobiliary fistula due to
radiofrequency ablation for recurrent hepatocellular carcinoma.
Korean J Hepatobiliary Pancreat Surg. 17:135–138. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Karabulut N, Cakmak V and Kiter G:
Confident diagnosis of bronchobiliary fistula using
contrast-enhanced magnetic resonance cholangiography. Korean J
Radiol. 11:493–496. 2010. View Article : Google Scholar : PubMed/NCBI
|