Introduction
Primary central nervous system (CNS) germ cell
tumors (GCTs) are a rare heterogeneous group of lesions located in
the CNS (1). CNS GCTs occur primarily
in children and adolescents, with ~90% of cases arising before the
age of 20 years (2). Pathological
classification of CNS GCTs, according to the World Health
Organization criteria, comprises germinoma, teratoma, yolk sac
tumor, embryonal carcinoma, choriocarcinoma and mixed GCT (3). Although CNS GCTs are considered to be
one of the most treatable types of malignant brain tumor, and may
be treated using neoadjuvant therapy in combination with
pre/post-chemoradiotherapy, a subset of patients remain resistant
to standard chemotherapy agents, primarily due to the clinical and
histological heterogeneity of CNS GCTs (4). Therefore, the development of an
understanding of the detailed molecular mechanisms underlying CNS
GCTs is imperative, in order to discover novel potential treatments
for tumors that demonstrate resistance to traditional therapeutic
strategies.
The proto-oncogene c-Kit encodes a
transmembrane tyrosine kinase (TK) receptor, containing an
extracellular domain with five immunoglobulin-like repeats (D1
distal-D5 juxtamembrane), a transmembrane domain, a juxtamembrane
domain, and TK 1 and 2 domains (5).
The natural c-Kit ligand, stem cell factor (SCF), binds
distal D1, D2 and D3 domains and activates downstream signaling,
including Src family kinase, phosphoinositide 3-kinase and
mitogen-activated protein kinase signaling pathways, promoting cell
migration, proliferation and apoptosis resistance (6). SCF/KIT signaling has a significant role
in a number of normal tissues, including germ cells, melanocytes,
mast cells and interstitial cells of Cajal (7–10). The
absence of KIT or SCF expression in mice results in death,
suggesting an irreplaceable role of SCF/KIT signaling during
embryonic or perinatal death (11).
In addition, human c-Kit mutations in exons 8, 9, 11, 13 and
17 have been identified in 75–80% of gastrointestinal stromal
tumors (GISTs) (12). c-Kit
mutations have additionally been frequently identified in 30% of
GCTs, including testicular seminoma, ovarian dysgerminoma and
mediastinal seminoma (13–15).
It has been observed that there is significant
genetic variation for the same disease among certain ethnic groups
(16). Considering the fact that
mutation of c-Kit in CNS GCTs has been reported in a number
of studies (17,18), and no study to the best of our
knowledge has focused on Chinese populations, the present study
investigated 4 mutant hot spots of the c-Kit gene (exons 9, 11, 13
and 17) using polymerase chain reaction (PCR) amplification and
direct sequencing, to identify the presence, frequency and location
of c-Kit mutations. In addition, KIT protein expression was
detected using immunohistochemistry, and its correlation with
patient clinicopathological data was analyzed.
Materials and methods
Patients and specimens
Between January 1994 and October 2014, 21 male and 9
female Chinese patients (male:female ratio, 2.3:1), diagnosed with
primary intracranial GCTs at Ren Ji Hospital, School of Medicine,
Shanghai Jiao Tong University (Shanghai, China) were enrolled in
the present study. None of the patients had received chemotherapy
or radiotherapy prior to surgery. A total of 39 formalin-fixed
paraffin-embedded tumor tissue samples, and one fresh tumor tissue,
were collected from primary intracranial GCT patients. All tumor
samples were reviewed by two pathologists in order to verify the
diagnosis. The basic clinical characteristics of patients are
presented in Table I. The present
study was approved by the Ethics Committee of Ren Ji Hospital,
School of Medicine, Shanghai Jiao Tong University (Shanghai,
China). Written informed consent for the use of patient tissue
specimens in the present study was obtained from all patients.
 | Table I.Clinicopathological data, c-Kit gene
mutations and c-Kit IHC staining in 23 intracranial germ cell
tumors. |
Table I.
Clinicopathological data, c-Kit gene
mutations and c-Kit IHC staining in 23 intracranial germ cell
tumors.
| Case number | Age, years | Gender | Location | Histological
type | Size, cm | c-Kit IHC | c-Kit mutation |
|---|
| 1 | 12 | F | Sellar | G | 3.5 | 2+ | Wild-type |
| 2 | 14 | M | Pineal | G | 1.5 | 4+ | Wild-type |
| 3 | 9 | M | Pineal | G | 5.0 | 3+ | Wild-type |
| 4 | 17 | M | Third
ventricle | G | 2.5 | 3+ | Wild-type |
| 5 | 7 | M | Third
ventricle | IT | 2.5 | – | Wild-type |
| 6 | 15 | M | Pineal | G | 3.0 | 4+ | 557,558 |
| 7 | 16 | M | Hypothalamus | G | 5.0 | 3+ | Wild-type |
| 8 | 30 | M | Sellar | G | 2.0 | 2+ | Wild-type |
| 9 | 17 | F | Hypothalamus | G | 3.0 | 4+ | Wild-type |
| 10 | 8 | M | Basal ganglia | G | 5.5 | 2+ | Wild-type |
| 11 | 13 | F | Sellar | G | 3.0 | 2+ | Wild-type |
| 12 | 11 | F | Suprasellar | G | 3.0 | 1+ | Wild-type |
| 13 | 11 | F | Sellar | G | 4.5 | 3+ | Wild-type |
| 14 | 16 | M | Sellar | G | 2.0 | – | Wild-type |
| 15 | 18 | M | Hypothalamus | G | 3.0 | 4+ | Wild-type |
| 16 | 30 | M | Hypothalamus | G | 2.5 | 3+ | Wild-type |
| 17 | 25 | M | Third
ventricle | G | 5.0 | 3+ | Wild-type |
| 18 | 31 | M | Pineal | MT | 3.0 | – | Wild-type |
| 19 | 18 | M | Hypothalamus | MT | 5.0 | – | Wild-type |
| 20 | 24 | M | Pineal | MGCT | 3.0 | 2+ | Wild-type |
| 21 | 11 | M | Pineal | G | 3.0 | 4+ | Wild-type |
| 22 | 9 | F | Pineal | MGCT | 3.5 | 1+ | Wild-type |
| 23 | 12 | F | Sellar | EC | 4.0 | – | Wild-type |
Immunohistochemistry and staining
evaluation
Surgical specimens were fixed in 10% formalin
(Guanghua Sci-Tech Co., Ltd., Guangdong, China) and embedded in
paraffin. Sections (4-µm) were cut and stained by hematoxylin and
eosin (Sangon Biotech Co., Ltd., Shanghai, China). Additional 4-µm
sections were deparaffinized using xylene and rehydrated in a
graded series of ethanol. The deparaffinized sections were
subsequently incubated with 3% H2O2 to
inhibit any endogenous peroxidase activity, followed by microwave
treatment for antigen retrieval prior to incubation with primary
antibody, using a two-step polymer method (EnVision™; Dako,
Glostrup, Denmark). The sections were incubated in a humidified
chamber at 4°C overnight, following addition of polyclonal rabbit
anti-human c-Kit (A4502; Dako) at working dilutions of
1:100. Subsequently, secondary antibody (anti-rabbit IgG; cat no.
A042301; Dako) was added following rinsing with phosphate-buffered
saline. The sections were incubated at room temperature for 30 min,
subsequently immunoreactivity was detected using
3,3-diaminobenzidine (Sangon Biotech Co., Ltd.) for 15 min, and
finally counterstained using hematoxylin. GIST tissues were
obtained from Ren Ji Hospital (School of Medicine, Shanghai Jiao
Tong University) and utilized as a positive control for staining.
Negative controls were prepared using blocking serum instead of
primary antibody. c-Kit expression was assessed based on the
intensity and extent of membranous staining. The semi-quantitative
scoring system was based on the immunoreactive score (IRS), which
was defined as the product of percentage of positive cells (PP) and
staining intensity (SI). PP was scored as follows: 0, no staining;
1+, 1–25% stained; 2+; 26–50% stained;
3+, 51–75%, stained; and 4+, >75% stained.
An IRS of 0, 1+ and 2+ were defined as weak
expression and an IRS of ≥3+ as strong expression. SI
was scored from 0–3 according to staining colour: 0, no staining;
1, faint yellow; 2, yellow-brown; 3, sepia. The cells were veiwed
under a microscope (CX31; Olympus Corporation, Tokyo, Japan).
DNA extraction
Genomic DNA was extracted from paraffin-embedded
tumor specimens using a QIAamp DNA mini kit (Qiagen GmbH, Hilden,
Germany) according to the manufacturer's protocols. The quality and
concentration of DNA was assessed using a spectrophotometer
(NanoDrop™ 2000; Thermo Fisher Scientific, Waltham, MA, USA) and
resolved on a 0.8% TBE gel (Thermo Fisher Scientific).
The amplified DNA fragments were purified using a
GFX PCR DNA and Gel Band Purification kit (GE Healthcare Life
Sciences, Chalfont, UK) DNA fragments that aligned with exons 9,
11, 13 and 17 were amplified by PCR, using various primers from
Invitrogen (Thermo Fisher Scientific; Table II). Each PCR reaction consisted of 5
µl 10X PCR buffer, 5 µl magnesium chloride (25 mmol/l), 1 µl 10
mmol/l deoxynucleotide triphosphates, 0.5 units Taq DNA
polymerase (Bio-Rad Laboratories, Inc., Hercules, CA, USA), 2 µl
genomic DNA and 1 µl of each primer (10 µmol/l), in a final volume
of 50 µl. The cycling conditions were as follows: 94°C for 5 min,
35 cycles at 94°C for 30 sec, at 60°C for 30 sec and 72°C for 30
sec, with a final extension step at 72°C for 10 min. The amplified
fragments were purified using a EZ-10 Spin Column PCR Products
Purification kit (Bio Basic Canada, Inc., Markham, ON, Canada) and
direct sequencing was performed using an ABI Prism® 3100
genetic analyzer (Applied Biosystems; Thermo Fisher Scientific).
The sequencing results were analyzed using Chromas Lite software
(version 2.1.1; Technelysium Pty Ltd., Brisbane, Australia), with a
signal to noise ratio of >98%. Each sample was sequenced at ≥2
times.
| Table II.Summary of primer sequences utilized
for amplification and sequencing of c-Kit exons 9, 11, 13 and
17. |
Table II.
Summary of primer sequences utilized
for amplification and sequencing of c-Kit exons 9, 11, 13 and
17.
| Exon | Primer | Sequence 5→3 | Annealing
temperature, °C | Fragment size,
bp |
|---|
| c-Kit 9 | F |
TCCTAGAGTAAGCCAGGGCTT | 54 | 284 |
|
| R |
TGGTAGACAGAGCCTAAACATCC |
|
|
| c-Kit 11 | F |
CTGAGACAATAATTATTAAAAGGTGA | 55 | 227 |
|
| R |
TTATGTGTACCCAAAAAGGTGACA |
|
|
| c-Kit 13 | F |
GCTTGACATCAGTTTGCCAG | 54 | 193 |
|
| R |
AAAGGCAGCTTGGACACGGCTTTA |
|
|
| c-Kit 17 | F |
TACAAGTTAAAATGAATTTAAATGGT | 53 | 228 |
|
| R |
AAGTTGAAACTAAAAATCCTTTGC |
|
|
Statistical analysis
Statistical analyses were performed using SPSS for
Windows (version 17.0; SPSS, Inc., Chicago, IL, USA). The
χ2 or Fishers exact tests were used for categorical and
ordinal variables. P<0.05 was considered to indicate a
statistically significant difference, and all reported P-values
were two-sided.
Results
Variable clinical characteristics of
the patients
The mean age of diagnosis of intracranial GCTs was
17.2 years (range, 7–31 years). The duration of symptoms prior to
diagnosis ranged from 5 days to 5 years, with a mean duration of
9.7 months. A total of 23 patients (76.7%), including all of the
female patients investigated in the present study, were younger
than 20 years at diagnosis. Intracranial GCT sites included the
sellar region, pineal gland, hypothalamus, third ventricle, basal
ganglia and others. The sellar region and pineal gland were the
most common sites for intracranial GCT occurrence. Clinical
presentations were dependent on the location and size of the tumor
in the intracranial region. Symptoms varied at diagnosis, and
included headaches, visual disturbances, signs of increased
intracranial pressure and endocrine abnormalities (Table I).
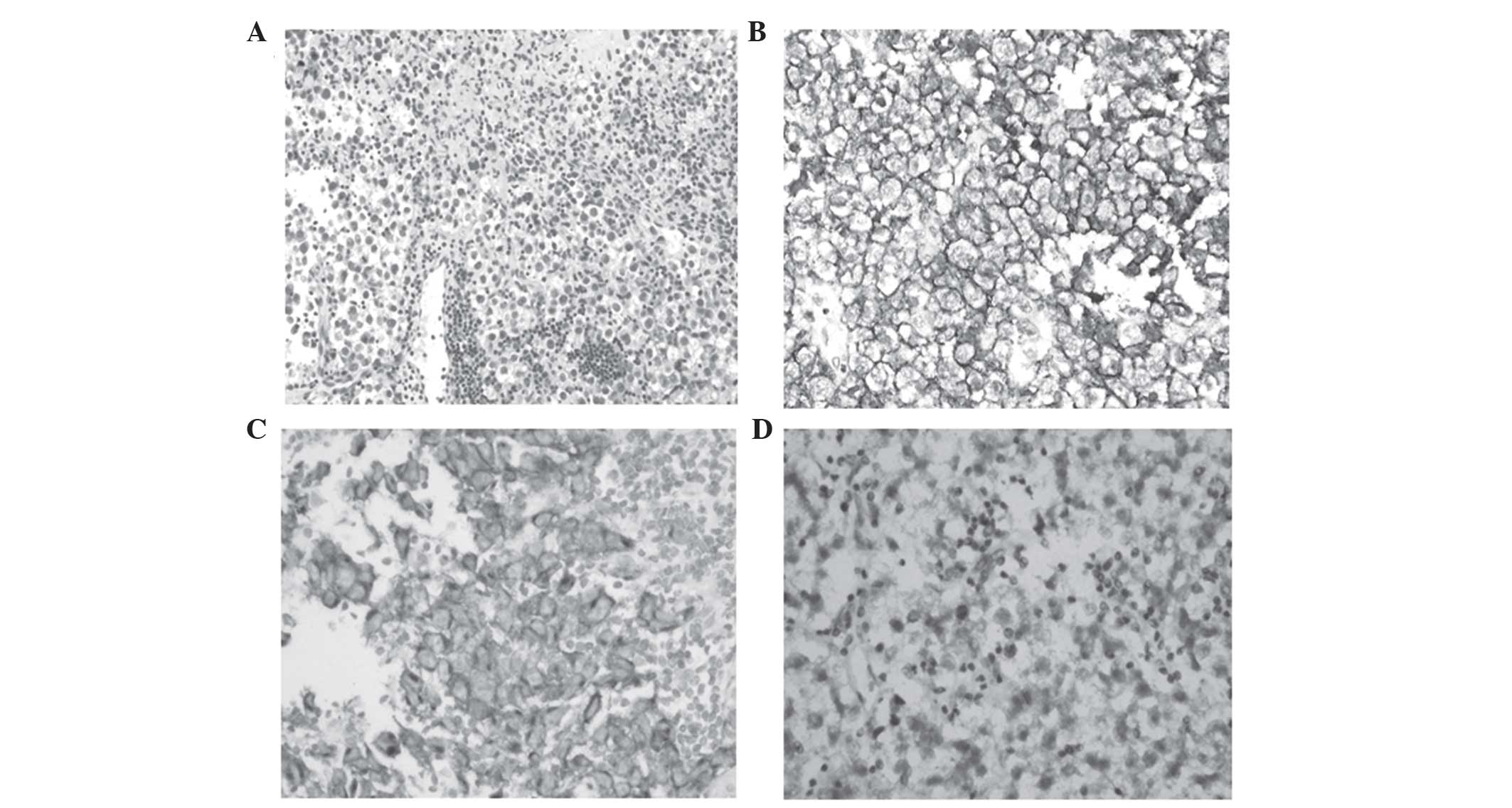
KIT protein is expressed in
intracranial GCT
KIT protein, which was primarily expressed in the
cytoplasmic membrane, was detected in 21/22 germinoma (95.5%) and
2/2 mixed GCT cases. However, expression of KIT protein was not
observed in any of the teratoma (4/4), embryonal carcinoma (1/1) or
choriocarcinoma (1/1) cases. High levels of staining were observed
in 13/22 (59.1%; 66.7% in males and 42.9% in females) germinoma
cases (Fig. 1). As presented in
Table III KIT protein expression
did not correlate with mutation of the c-Kit gene or any
patient clinicopathological parameters, including age, gender,
tumor size, tumor location and prognosis.
| Table III.Comparison of clinicopathological
data between germinoma patients with high and low KIT protein
expression. |
Table III.
Comparison of clinicopathological
data between germinoma patients with high and low KIT protein
expression.
|
| KIT expression |
|
|---|
|
|
|
|
|---|
| Variable | High, n=13 | Low, n=9 | P-value |
|---|
| Median age
(range) | 17 (9–30) | 15 (8–30) | 1 |
| Gender
(male:female) | 10:3 | 5:4 | 0.376 |
| Maximum size,
cm | 3.45 ± 1.21 | 3.17 ± 1.29 | 0.611 |
| Location |
|
|
|
|
Sellar | 1 | 4 |
|
|
Pineal | 4 | 1 |
|
| Third
ventricle | 2 | 1 |
|
|
Hypothalamus | 4 | 1 | 0.395 |
| Basal
ganglia | 1 | 1 |
|
|
Suprasella | 1 | 1 |
|
| Alive and well | 13 | 9 |
|
| c-Kit mutation | 1 | 0 | 1 |
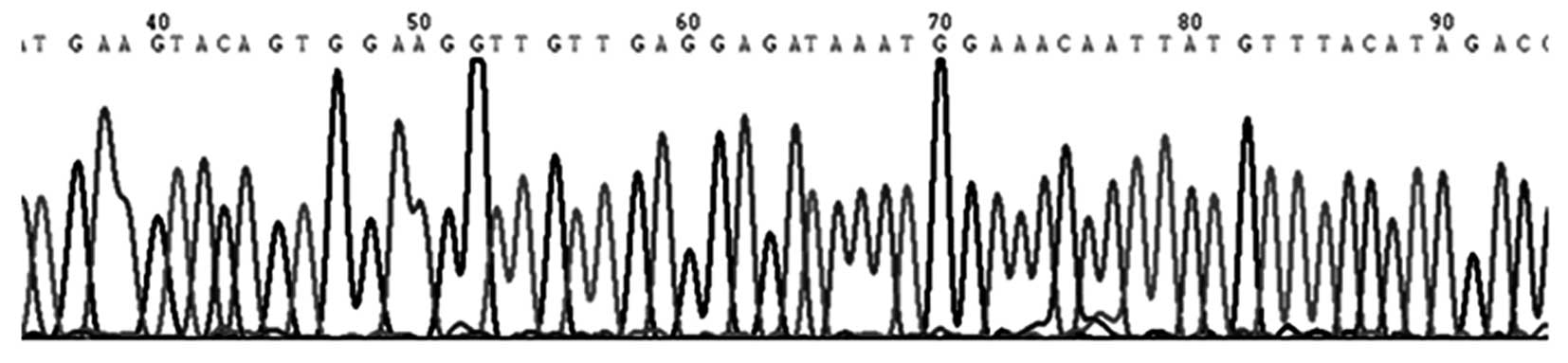
c-Kit gene mutation was observed in a
single germinoma patient
A total of 23 specimens (17 germinoma and 5
non-germinomatous cases) were screened for mutations in the
c-Kit gene. Among 17 intracranial germinoma cases, no gene
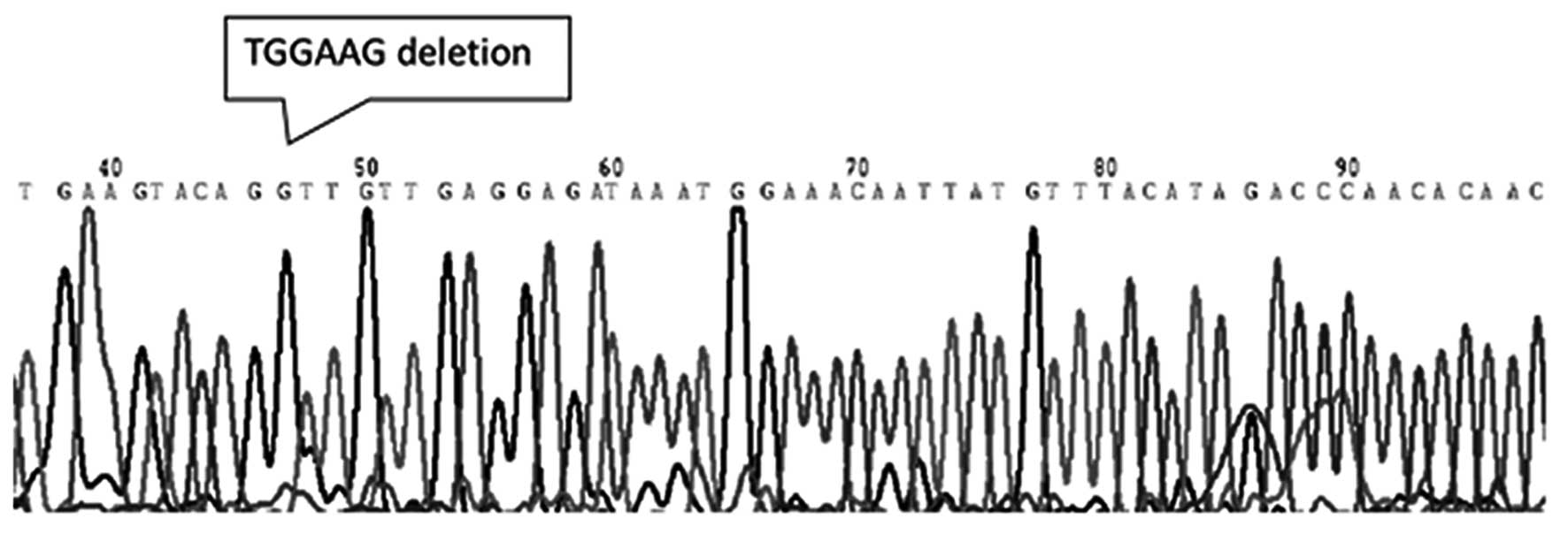
mutations was identified in 16 patients (Fig. 2) and only one c-Kit gene
mutation was identified in one patient (5.9%). The observed
mutation was located in exon 11, which encodes the juxtamembrane,
and was classified as an in-frame deletion at codon 557–558 WK
[Tryptophan (Trp)-Lysine (Lys)]. The mutation was considered to a
be gain-of-function type (Fig. 3).
None of the investigated germinoma cases exhibited mutations in
exons 9, 13 or 17 of the c-Kit gene. No mutations were
detected in exons 9, 11, 13 or 17 of the c-Kit gene in any
of the non-germinomatous GCT cases, including 3 teratomas and 2
mixed GCTs, in the present study.
Discussion
Due to significant advances in treatment options for
CNS germinoma patients, it has become essential to develop novel
therapeutic strategies for patients that achieve no response to
standard chemotherapeutic agents. Due to its expression and
mutation in CNS GCTs, c-Kit is a significant potential
therapeutic target (18). KIT protein
expression in intracranial germinoma cases has been reported in a
number of previous studies (17,18).
Sakuma et al (17) identified
that 100% of intracranial germinoma cases investigated demonstrated
membranous KIT protein expression. Similar to these previous
findings, the results of the present study revealed that KIT
protein expression was detectable in 95.5% of intracranial
germinoma cases. However, KIT protein expression was not observed
to significantly correlate with c-Kit gene mutation or
patient clinicopathological parameters, including age, gender,
tumor size, tumor location and prognosis, which was in accordance
with multiple types of tumors with the exceptions of the GISTs
(19).
In the present study, no mutations were detected in
exons 9, 11, 13, and 17 of the c-Kit gene in non-germinomatous GCT
cases, including 3 teratomas and 2 mixed GCTs, which was a similar
finding to the results of a number of previous studies (5,20–22). The present study identified that 1/17
(5.88%) CNS germinoma cases exhibited a c-Kit gene mutation
in exon 11, which encodes the juxtamembrane, and this mutation was
classified as an in-frame deletion at codon 557–558 WK (Trp-Lys).
The results of the present study differed from previous studies,
which reported that c-Kit mutations were identified in 4/16
(25%) and 3/13 (23%) Japanese patients exhibiting germinomas
(17,18). In addition, these previous studies
demonstrated that 75% of germinoma cases exhibiting mutations
possessed a point mutation at exon 17 (D816V, D820V and N822Y), and
only 25% of gene mutations were observed to occur at exon 11
(17,18). There may be several reasons for the
discrepancy observed between the results of the present and
previous studies. The present study was performed on a cohort of
Chinese patients, while the previous studies were performed on
Japanese patient cohorts (17,18).
Therefore, the differences between these populations may be one of
the most plausible explanations underlying the discrepancy observed
between the results of the present study and previous studies.
Furthermore, as CNS GCTs are rare tumors, it is often only possible
to study small sample sizes, which may also be responsible for the
inconsistencies in results. Therefore, studies aiming to enroll
increased numbers of CNS GCT patients are required, and the
association between population factors and c-Kit gene
mutations in CNS GCTs requires further investigation.
Gain-of-function mutations of c-Kit have been
identified in a number of neoplasms, including GIST (23), mastocytosis (24) and hematologic malignancies (25). In addition, GIST patients exhibiting
c-Kit mutations in exon 11, which encodes the juxtamembrane
domain, have been reported to exhibit unfavorable prognosis
(26). In agreement with the results
of a number of previous studies, in the present study, the patient
exhibiting a c-Kit mutation encountered recurrence 8 months
subsequent to primary surgical excision, which suggested that
c-Kit mutation may be a gain-of-function type mutation
responsible for refractory intracranial germinomas. However, there
was no statistically significant correlation observed between
c-Kit protein expression and gene mutation in the present
study.
Imatinib, a TK inhibitor, has been utilized in order
to block the activated c-Kit receptor TK (27). A previous study has demonstrated that
imatinib is able to exert a significant suppressive effect on the
activation of the mutational c-Kit gene (28). CNS GCT cases exhibiting a mutant
c-Kit gene within exon 11 have been reported to demonstrate
sensitivity to imatinib treatment (29). However, other studies identified that
a mutant c-Kit gene, which exhibited a codon 816 mutation at
exon 17, resulted in resistance to imatinib treatment in GISTs
(27,30). Therefore, it is possible that
sensitivity to imatinib may depend on the type and site of the
c-Kit mutation, implying that imatinib may not be a suitable
treatment for certain patients exhibiting intracranial GCT. In the
present study, a missense mutation in exon 11 of the c-Kit
gene was detected in a CNS GCT patient. This patient was diagnosed
with germinoma exhibiting no notable clinicopathological features,
and experienced recurrence 8 months subsequent to primary surgical
excision. As the patient was harboring an activated mutation, they
may have demonstrated resistance to traditional anticancer therapy
and sensitivity to treatment with imatinib. Germinoma patients
exhibiting high levels of KIT protein expression may benefit from
gene mutation analysis, which may assist in determination of
whether imatinib treatment is appropriate.
In conclusion, KIT protein expression was detected
in 95.5% of germinoma cases and was not observed to correlate with
c-Kit gene mutation or clinicopathological parameters. In
addition, the present study identified that 1/17 (5.9%) patients
possessed mutations at exon 11 of the c-Kit gene, which differed
from the results of a number of previous studies based on Japanese
patient cohorts (17,18). No mutations were detected in
non-germinomatous GCT cases. To the best of our knowledge, the
present study was the first investigation into the expression and
mutation of c-Kit in Chinese patients exhibiting CNS GCTs.
Additional studies investigating increased numbers of intracranial
GCT patients are required, and whole exome sequencing of c-Kit may
additionally be conducted in order to identify additional mutant
locations.
Acknowledgements
The authors would like to thank the Science and
Technology Commission of Shanghai Municipality (grant no.
134119a9502) for providing the funding for the present study.
References
|
1
|
Thakkar JP, Chew L and Villano JL: Primary
CNS germ cell tumors: Current epidemiology and update on treatment.
Med Oncol. 30:4962013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Dufour C, Guerrini-Rousseau L and Grill J:
Central nervous system germ cell tumors: An update. Curr Opin
Oncol. 26:622–626. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Louis DN, Ohgaki H, Wiestler OD, Cavenee
WK, Burger PC, Jouvet A, Scheithauer BW and Kleihues P: The 2007
WHO classification of tumours of the central nervous system. Acta
Neuropathol. 114:97–109. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Subbiah V, Meric-Bernstam F, Mills GB,
Shaw KR, Bailey AM, Rao P, Ward JF and Pagliaro LC: Next generation
sequencing analysis of platinum refractory advanced germ cell tumor
sensitive to Sunitinib (Sutent®) a
VEGFR2/PDGFRβ/c-kit/FLT3/RET/CSF1R inhibitor in a phase II trial. J
Hematol Oncol. 7:522014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sakuma Y, Sakurai S, Oguni S, Hironaka M
and Saito K: Alterations of the c-kit gene in testicular germ cell
tumors. Cancer Sci. 94:486–491. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cruse G, Metcalfe DD and Olivera A:
Functional deregulation of KIT: Link to mast cell proliferative
diseases and other neoplasms. Immunol Allergy Clin North Am.
34:219–237. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Rossi P: Transcriptional control of KIT
gene expression during germ cell development. Int J Dev Biol.
57:179–184. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yamada T, Hasegawa S, Inoue Y, Date Y,
Yamamoto N, Mizutani H, Nakata S, Matsunaga K and Akamatsu H:
Wnt/β-catenin and kit signaling sequentially regulate melanocyte
stem cell differentiation in UVB-induced epidermal pigmentation. J
Invest Dermatol. 133:2753–2762. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Reber LL, Marichal T and Galli SJ: New
models for analyzing mast cell functions in vivo. Trends
Immunol. 33:613–625. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Huizinga JD, Thuneberg L, Klüppel M,
Malysz J, Mikkelsen HB and Bernstein A: W/kit gene required for
interstitial cells of Cajal and for intestinal pacemaker activity.
Nature. 373:347–349. 1995. View
Article : Google Scholar : PubMed/NCBI
|
|
11
|
Broudy VC: Stem cell factor and
hematopoiesis. Blood. 90:1345–1364. 1997.PubMed/NCBI
|
|
12
|
Rammohan A, Sathyanesan J, Rajendran K,
Pitchaimuthu A, Perumal SK, Srinivasan U, Ramasamy R, Palaniappan R
and Govindan M: A gist of gastrointestinal stromal tumors: A
review. World J Gastrointest Oncol. 5:102–112. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Coffey J, Linger R, Pugh J, Dudakia D,
Sokal M, Easton DF, Bishop Timothy D, Stratton M, Huddart R and
Rapley EA: Somatic KIT mutations occur predominantly in seminoma
germ cell tumors and are not predictive of bilateral disease:
Report of 220 tumors and review of literature. Genes Chromosomes
Cancer. 47:34–42. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Hoei-Hansen CE, Kraggerud SM, Abeler VM,
Kaern J, Rajpert-De Meyts E and Lothe RA: Ovarian dysgerminomas are
characterised by frequent KIT mutations and abundant expression of
pluripotency markers. Mol Cancer. 6:122007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Terada T: Mediastinal seminoma with
multiple KIT gene mutations. Pathology. 41:695–697. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yuan F, Shi M, Ji J, Shi H, Zhou C, Yu Y,
Liu B, Zhu Z and Zhang J: KRAS and DAXX/ATRX gene mutations are
correlated with the clinicopathological features, advanced
diseases, and poor prognosis in Chinese patients with pancreatic
neuroendocrine tumors. Int J Biol Sci. 10:957–965. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sakuma Y, Sakurai S, Oguni S, Satoh M,
Hironaka M and Saito K: c-kit gene mutations in intracranial
germinomas. Cancer Sci. 95:716–720. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kamakura Y, Hasegawa M, Minamoto T,
Yamashita J and Fujisawa H: C-kit gene mutation: Common and widely
distributed in intracranial germinomas. J Neurosurg. 104(Suppl):
173–180. 2006.PubMed/NCBI
|
|
19
|
Miettinen M and Lasota J: KIT (CD117): A
review on expression in normal and neoplastic tissues, and
mutations and their clinicopathologic correlation. Appl
Immunohistochem Mol Morphol. 13:205–220. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
McIntyre A, Summersgill B, Grygalewicz B,
Gillis AJ, Stoop J, van Gurp RJ, Dennis N, Fisher C, Huddart R,
Cooper C, et al: Amplification and overexpression of the KIT gene
is associated with progression in the seminoma subtype of
testicular germ cell tumors of adolescents and adults. Cancer Res.
65:8085–8089. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Willmore-Payne C, Holden JA, Chadwick BE
and Layfield LJ: Detection of c-kit exons 11- and 17-activating
mutations in testicular seminomas by high-resolution melting
amplicon analysis. Mod Pathol. 19:1164–1169. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Cheng L, Roth LM, Zhang S, Wang M, Morton
MJ, Zheng W, Karim Abdul FW, Montironi R and Lopez-Beltran A: KIT
gene mutation and amplification in dysgerminoma of the ovary.
Cancer. 117:2096–2103. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Lennartsson J and Rönnstrand L: Stem cell
factor receptor/c-Kit: From basic science to clinical implications.
Physiol Rev. 92:1619–1649. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Bodemer C, Hermine O, Palmérini F, Yang Y,
Grandpeix-Guyodo C, Leventhal PS, Hadj-Rabia S, Nasca L,
Georgin-Lavialle S, Cohen-Akenine A, et al: Pediatric mastocytosis
is a clonal disease associated with D816V and other activating
c-KIT mutations. J Invest Dermatol. 130:804–815. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Corbin AS, O'Hare T, Gu Z, Kraft IL,
Eiring AM, Khorashad JS, Pomicter AD, Zhang TY, Eide CA, Manley PW,
et al: KIT signaling governs differential sensitivity of mature and
primitive CML progenitors to tyrosine kinase inhibitors. Cancer
Res. 73:5775–5786. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Calibasi G, Baskin Y, Alyuruk H, Cavas L,
Oztop I, Sagol O, Atila K, Ellidokuz H and Yilmaz U: Molecular
analysis of the KIT gene in gastrointestinal stromal tumors with
novel mutations. Appl Immunohistochem Mol Morphol. 22:37–45. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Heinrich MC, Corless CL, Demetri GD,
Blanke CD, von Mehren M, Joensuu H, McGreevey LS, Chen CJ, Van den
Abbeele AD, Druker BJ, et al: Kinase mutations and imatinib
response in patients with metastatic gastrointestinal stromal
tumor. J Clin Oncol. 21:4342–4349. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Corless CL, Ballman KV, Antonescu CR,
Kolesnikova V, Maki RG, Pisters PW, Blackstein ME, Blanke CD,
Demetri GD, Heinrich MC, et al: Pathologic and molecular features
correlate with long-term outcome after adjuvant therapy of resected
primary GI stromal tumor: the ACOSOG Z9001 trial. J Clin Oncol.
32:1563–1570. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Hou YY, Tan YS, Sun MH, Wei YK, Xu JF, Lu
SH, A-Ke-Su SJ, Zhou YN, Gao F, Zheng AH, et al: C-kit gene
mutation in human gastrointestinal stromal tumors. World J
Gastroenterol. 10:1310–1314. 2004.PubMed/NCBI
|
|
30
|
Tetzlaff ED and Davey MP: Optimizing
adherence to adjuvant imatinib in gastrointestinal stromal tumor. J
Adv Pract Oncol. 4:238–250. 2013.PubMed/NCBI
|