Introduction
Sclerosing stromal tumor (SST) of the ovary is a
rare benign tumor that has been classified as a sex cord-stromal
tumor and is predominantly observed in young women (1,2). SSTs
account for 1.5% of all ovarian tumors (1). The tumor usually occurs in the second
and third decades of life (mean age, 21 years). The most common
presenting symptoms are menstrual irregularity, abdominal pain and
a lower abdominal mass (1,2). Microscopically, the tumor is
characterized by pseudo-lobulation of cellular areas, marked
vascularity and significant variation in cellular size and shape,
and sclerosis is common (1,3). Surgical removal is curative and no local
or distant recurrences have been reported following surgery
(2,3).
To the best of our knowledge, there have been numerous reports
regarding the microscopic, ultrastructural and immunohistochemical,
but not imaging, findings associated with this tumor (3). The present study describes the computed
tomography (CT) findings of 2 patients with ovarian SST, and
confirms the correlation between imaging and pathological findings,
as well as the reliability of imaging in preoperative
characterization. The study was approved by the Ethics Committee of
Subei People's Hospital of Jiangsu Province (Yangzhou, China) and
the patients provided written informed consent for the publication
of the present study.
Case report
Case 1
An 18-year-old Chinese female patient was admitted
to Subei People's Hospital of Jiangsu Province in July 2012 with
menstrual irregularities for 6 months. The blood test results for
blood cell count, biochemistry and tumor markers, including cancer
antigen (CA)19-9 (3.57 KU/l; normal range, <35.00 KU/l),
carcinoembryonic antigen CA125 (5.15 KU/l; normal range, <35.00
KU/l) and α-fetoprotein (3.57 ng/ml; normal range, <20.00 ng/ml)
were all normal. The levels of serum hormones, including estradiol
(60 ng/ml; normal range, 22–144 ng/ml), progesterone (8.13 ng/ml;
normal range, 5.16–18.56 ng/ml) and testosterone (12.3 ng/ml;
normal range, 10.0–75.0 ng/ml), were also normal.
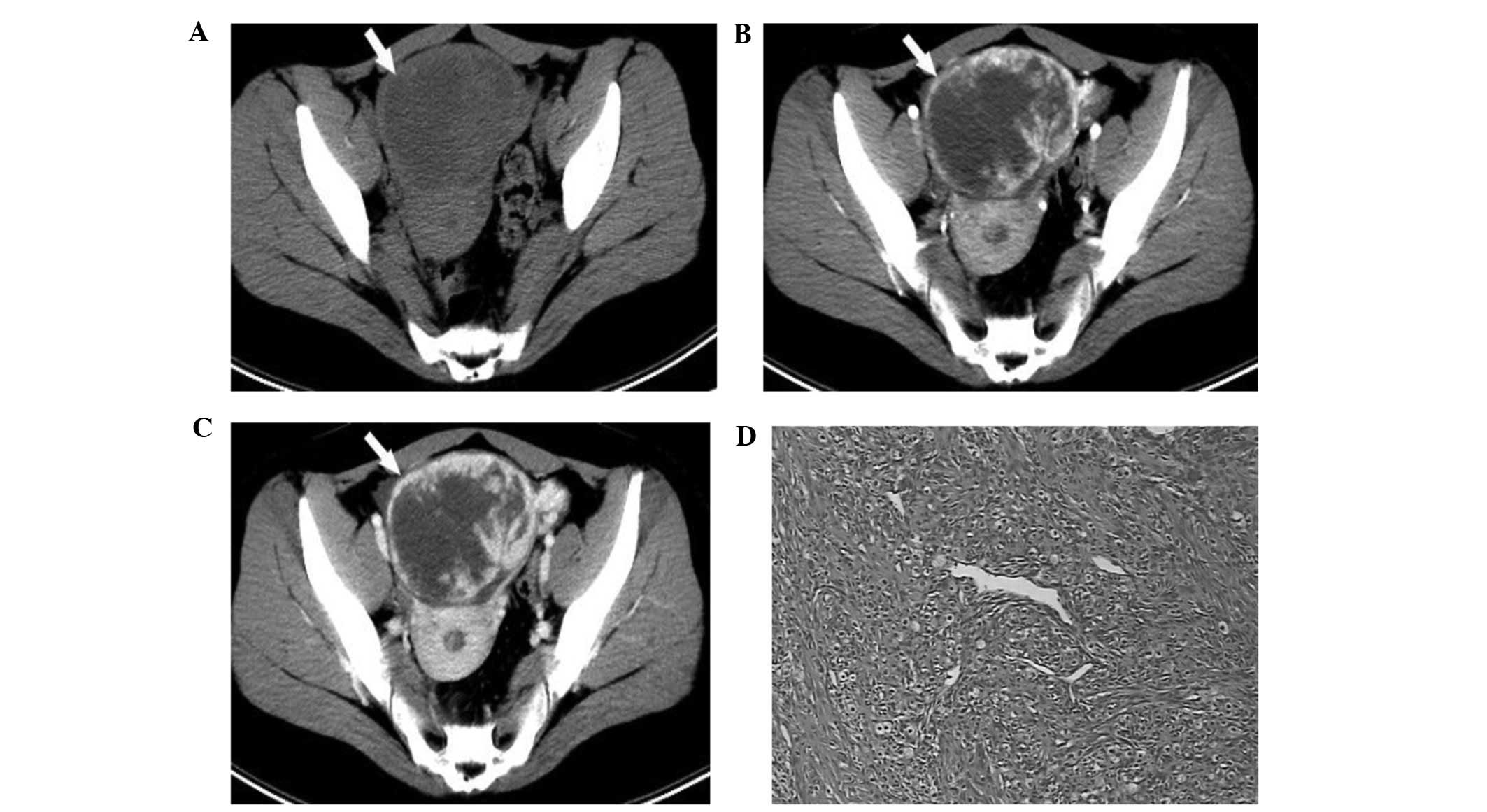
Non-enhanced CT (Lightspeed VCT 64; GE Healthcare,
Milwaukee, WI, USA) scan revealed a round soft tissue mass with
clear boundaries in the middle of the pelvis. The mass measured
76×77 mm and displayed non-homogeneous density, with solid,
non-calcified tissue at the periphery and a fluid, patch-shaped
area in the inner zone (Fig. 1A).
Plain CT values were 31–45 HU, with a mean value of 37.6 HU.
Intravenous bolus injection of iodinated contrast medium
(iopromide; Ultravist® 320; Bayer HealthCare
Pharmaceuticals, Berlin, Germany) yielded early nodular and ring
enhancement of the peripheral portion of the mass, which was as
high as that of the vessels in the arterial phase (Fig. 1B). In the venous phase, the degree of
enhancement was decreased, but the area of enhancement increased
with centripetal progression (Fig.
1C). The CT values in the arterial and venous phases were
145–150 HU, with a mean value of 147 HU, and 128–135 HU, with a
mean value of 130 HU, respectively. The cystic components of the
tumor were not enhanced in these phases, and no pelvic or
lumbo-aortic enlarged lymph nodes were observed.
It was confirmed that the mass originated from the
left ovarian tissue. Macroscopic examination revealed a 100×80-mm
surgical specimen, which was yellow-orange in color and contained
solid, cystic components. Resected tissue specimens were fixed in
10% formalin, paraffin-embedded and cut into 5-mm sections.
Sections were stained with hematoxylin and eosin (Shanghai Haiyi
Scientific & Trading Co., Ltd., Shanghai, China) for
histological examination and staining was visualized using a
microscope (JVC1481; Olympus Corporation, Tokyo, Japan).
Histological examination of the mass revealed cellular areas
separated by hypocellular areas of densely collagenous, edematous
or myxoid tissue, alongside prominent vasculature, thus resulting
in a pseudo-lobular pattern. The cellular areas were composed of
oval to spindle-shaped cells, with a single oval to round-shaped
nucleus and a single prominent nucleolus. The cytoplasm was
moderately abundant, eosinophilic and occasionally vacuolated
(Fig. 1D). Immunohistochemical
staining was performed using the avidin biotin peroxidase method,
and demonstrated focal positivity for actin, pan-cytokeratin (CK),
inhibin and calretinin, and negativity for S100, desmin and
epithelial membrane antigen. Based on these findings, a diagnosis
of SST of the left ovary was established. The patient exhibited
regular menstrual cycles and no signs of local or distal recurrence
2 years post-surgery.
Case 2
A 59-year-old woman was admitted to Subei People's
Hospital of Jiangsu Province in May 2013 with continuous pelvic
pain that had been ongoing for a year. Clinical examination
identified a large mass that was palpable in the right-side of the
lower pelvis. Ultrasonography revealed a well-defined solid-cystic
echogenic mass in the right ovary measuring 64×55 mm. Laboratory
tests and hormonal assays, including CA19-9 (13.11 KU/l; normal
range, <35.00 KU/l), carcinoembryonic antigen CA125 (16.15 KU/l;
normal range, <35.00 KU/l), α-fetoprotein (1.57 ng/ml; normal
range, <20.00 ng/ml), estradiol (31 pg/ml; normal range, 22–144
pg/ml), progesterone (11.13 ng/ml; normal range, 5.16–18.56 ng/ml)
and testosterone (21.6 ng/ml; normal range, 10–75 ng/ml) were
normal.
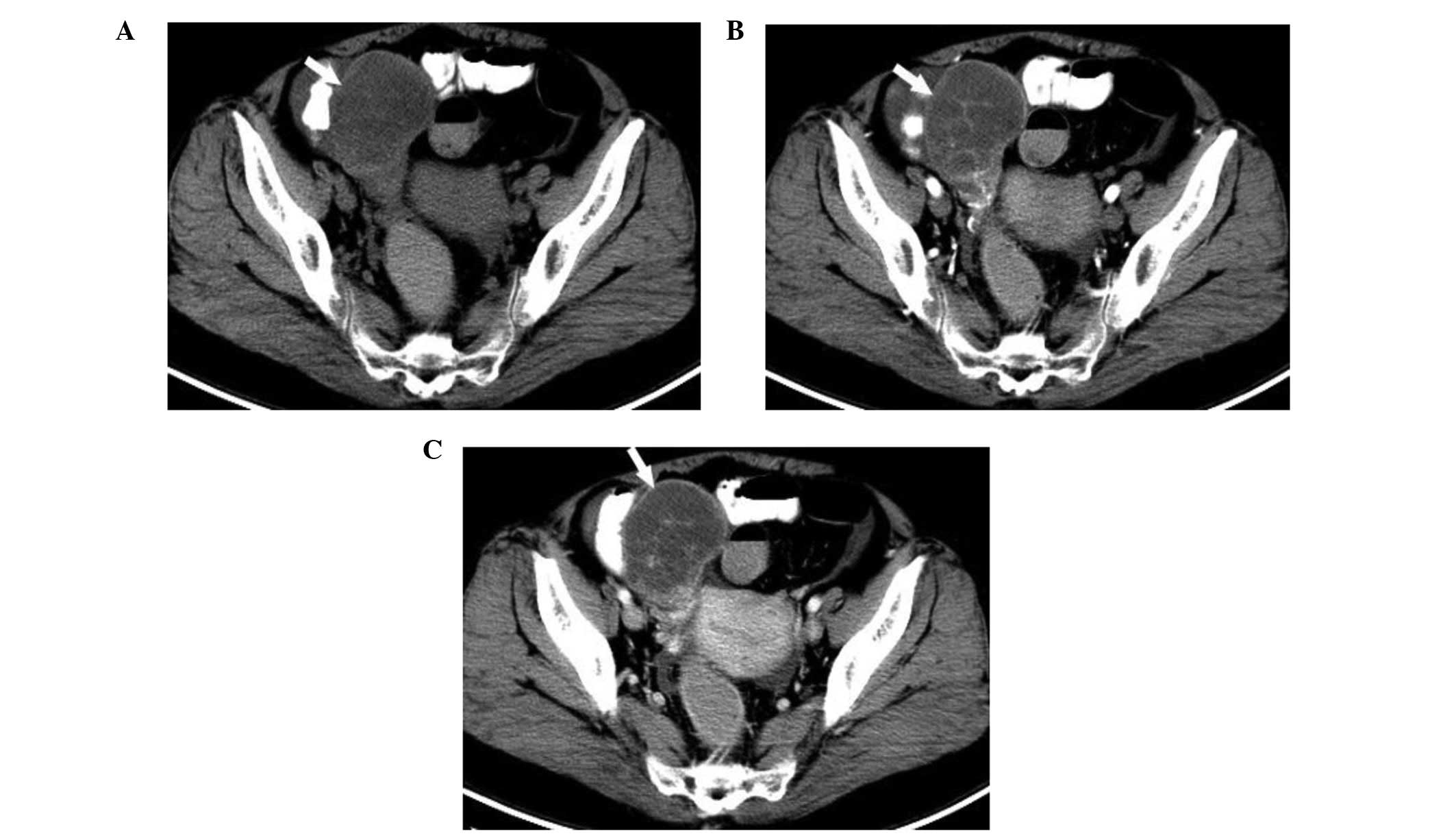
Plain CT scan revealed an ovoid soft tissue mass
located in the right pelvis. The tumor, which measured 64×55 mm in
size, had clear boundaries and showed non-homogeneous density with
solid tissue at the periphery (Fig.
2A). Plain CT scan values were 25–40 HU, with a mean value of
32.6 HU. Intravenous bolus injection of iodinated contrast medium
yielded early ring enhancement of the peripheral portion of the
mass (Fig. 2B). In the venous phase,
the degree of enhancement was decreased, but the area of
enhancement increased with centripetal progression (Fig. 2C). The CT values at the arterial and
venous phases were 125–140 HU, with a mean value of 132 HU, and
118–130 HU, with a mean value of 128 HU, respectively. The cystic
components of the inner region of the lesion were not enhanced in
these phases.
The patient underwent surgical removal of the
70×60-mm mass, which was well-circumscribed and presented a round
to oval-shape with a smooth outer surface. The resected section was
of pale yellow color with solid cystic areas. Histological
examination revealed that the mass was characterized by cellular
areas separated by hypocellular areas of densely collagenous,
edematous or myxoid tissue and prominent vasculature, thus creating
a pseudo-lobular pattern. The cellular areas were composed of oval
to spindle-shaped cells, with a single oval to round-shaped nucleus
and a single prominent nucleolus. Tumor cells stained positive for
smooth muscle actin and vimentin, and focally positive for inhibin.
The patient was disease-free with no imaging findings of recurrence
or metastasis 24 months following surgery.
Discussion
Ovarian SST is a considerably rare and distinctive
sex cord-stromal neoplasm, which was first described by
Chalvardjian and Scully in 1973 (1).
The histogenesis of this tumor remains unknown, and it
predominantly affects young women in the second and third decades
of life (mean age, 21 years) (2). To
the best of our knowledge, <100 cases of ovarian SST have been
reported in the English language literature thus far (2–4). Of these,
>80% of SSTs have been observed in young adults, in the second
and third decades of life (2,3). The most common clinical symptoms of
patients with SST of the ovary are menstrual irregularities, pelvic
pain and non-specific symptoms associated with the existence of a
mass in the pelvic area (2,4). Due to the rarity of this neoplasm, it is
not always possible to predict the presence of this tumor
preoperatively based solely on clinical and radiological findings
(5).
Microscopically, SST is characterized by cellular
areas separated by hypocellular areas of densely collagenous,
edematous or myxoid tissue and prominent vasculature, which creates
a pseudo-lobular pattern (6,7). In a previous study, the cellular areas
were observed to be composed of oval to spindle-shaped cells, with
a single oval to round-shaped nucleus and a single prominent
nucleolus (8). In addition, the
cytoplasm was moderately abundant, eosinophilic and occasionally
vacuolated (8). A previous study
revealed that the blood vessels within the cellular area were
mildly ectatic, and no evidence of malignancy was observed
(6). Following surgery, the patient's
menstrual condition returned to normal (6).
In previous studies, CT imaging demonstrated that
the density and enhancement patterns of SST are associated with the
cellularity, vascularity, collagen distribution and necrosis or
cystic degeneration observed during histopathological examination
of the tumor (6,7). On non-enhanced CT, SST manifests solid
densities corresponding to cellularity, vascularity and
distribution of collagenous or fibrous stroma, while the areas of
necrosis or cystic degeneration exhibit low densities (7). The SSTs of the present 2 cases presented
patchy areas of low attenuation.
The appearance of SSTs on imaging scans,
particularly the enhancement pattern observed in dynamic
contrast-enhanced CT images, may vary widely, depending on the
distribution of cellularity, vascularity and collagenous or fibrous
stroma (9). Previous studies
demonstrated that the heterogeneously enhancing masses observed in
contrast-enhanced CT images are associated with the tumor
vascularity, cellularity and collagen distribution (7,9). In the
present cases, following the administration of intravenous contrast
material, the early enhancement of the outer region of the tumor
was possibly due to the cellular area with numerous vascular
spaces. The maximum enhancement value was 150 HU. In the venous
phase, the area of prolonged enhancement observed in the inner
portion of the lesion was considered to be associated with the
collagenized hypocellular area. The CT values were 110–123 HU, with
a mean value of 116 HU. The part of the tumor that did not exhibit
any apparent enhancement possibly corresponded to the markedly
edematous area. The present CT findings were almost identical to
those of previous studies (6,10), and were particularly in agreement with
the results of Torricelli et al (11), who reported that the appearance of SST
on dynamic contrast-enhanced CT images is considerably similar to
that of cavernous hemangioma of the liver, and can be
pathologically defined as ‘hemangioma-like’.
In conclusion, differential diagnosis of SSTs should
include other thecoma-fibroma, metastatic and malignant epithelial
ovarian tumors (12), since, due to
the rarity of SST, prospective imaging diagnosis is not
possible.
The present case report described certain imaging
features of ovarian SST based on a small-population sample.
Therefore, further studies are required to confirm the diagnostic
accuracy of imaging in cases of SST, and to determine whether the
patterns observed in imaging scans may aid the differentiation
between SST and other tumors.
Acknowledgements
The present study was supported by the General
Program of Yangzhou Natural Science Foundation (Yangzhou, China;
grant no., YZ2015100) and National Natural Science Foundation
(Beijing, China; grant no., 81571652).
References
|
1
|
Chalvardjian A and Scully RE: Sclerosing
stromal tumors of the ovary. Cancer. 31:664–670. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chang W, Oiseth SJ, Orentlicher R, Agarwal
G, Yahr LJ and Cayten CG: Bilateral sclerosing stromal tumor of the
ovaries in a premenarchal girl. Gynecol Oncol. 101:342–345. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kaygusuz EI, Cesur S, Cetiner H, Yavuz H
and Koc N: Sclerosing stromal tumour in young women:
Clinicopathologic and immunohistochemical spectrum. J Clin Diagn
Res. 7:1932–1935. 2013.PubMed/NCBI
|
|
4
|
Ihara N, Togashi K, Todo G, Nakai A,
Kojima N, Ishigaki T, Suginami N, Kinoshita M and Shintaku M:
Sclerosing stromal tumor of the ovary: MRI. J Comput Assist Tomogr.
23:555–557. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Outwater EK, Wagner BJ, Mannion C,
McLarney JK and Kim B: Sex cord-stromal and steroid cell tumors of
the ovary. Radiographics. 18:1523–1546. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kawauchi S, Tsuji T, Kaku T, Kamura T,
Nakano H and Tsuneyoshi M: Sclerosing stromal tumor of the ovary: A
clinicopathologic, immunohistochemical, ultrastructural, and
cytogenetic analysis with special reference to its vasculature. Am
J Surg Pathol. 22:83–92. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tian TT, Wu JT, Hu XH, Yang GM, Sun J,
Chen WX and Tian XC: Imaging findings of solitary fibrous tumor in
the abdomen and pelvis. Abdom Imaging. 39:1323–1329. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Matsubayashi R, Matsuo Y, Doi J, Kudo S,
Matsuguchi K and Sugimori H: Sclerosing stromal tumor of the ovary:
Radiologic findings. Eur Radiol. 9:1335–1338. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kim JY, Jung KJ, Chung DS, Kim OD, Lee JH
and Youn SK: Sclerosing stromal tumor of the ovary: MR-pathologic
correlation in three cases. Korean J Radiol. 4:194–199. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kawamura N, Kamoi I and Shigyo R:
Sclerosing stromal tumour of the ovary. Br J Radiol. 60:1031–1033.
1987. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Torricelli P, Caruso Lombardi A, Boselli F
and Rossi G: Sclerosing stromal tumor of the ovary: US, CT, and MRI
findings. Abdom Imaging. 27:588–591. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Jung SE, Lee JM, Rha SE, Byun JY, Jung JI
and Hahn ST: CT and MR imaging of ovarian tumors with emphasis on
differential diagnosis. Radiographics. 22:1305–1325. 2002.
View Article : Google Scholar : PubMed/NCBI
|